

Abstract
BACKGROUND: COPD and bronchiectasis frequently coexist, which creates an emerging phenotype with a worse prognosis. However, the impact of bronchiectasis on the natural history of COPD has not been fully evaluated and is still controversial. This meta-analysis was performed to clarify the associations of the presence of bronchiectasis with the prognosis and quality of life of patients with COPD.
METHODS: A systematic review and meta-analysis was performed following a search of medical databases, and included articles published up to April 2019. The following outcome measures were analyzed: age, sex, smoking history, body mass index, exacerbation rate, lung function, inflammatory biomarkers, albumin, colonization by potentially pathogenic microorganisms, Pseudomonas aeruginosa isolates, Haemophilus influenzae isolates, hospital admissions, and mortality.
RESULTS: A total of 415,257 subjects with COPD from 18 observational studies were eligible; bronchiectasis was present in 25,929 subjects (6.24%). The coexistence of COPD and bronchiectasis occurred more often in older subjects with lower body mass index. The presence of bronchiectasis in the subjects with COPD increased the risk of daily sputum production (odds ratio [OR] 1.80, 95% CI 1.24–2.61), exacerbation (weighted mean difference [WMD] 0.72 times, 95% CI 0.59–0.85), frequent hospital admissions (WMD 0.35 times, 95% CI 0.21–0.49), and follow-up (>3 years) mortality (OR 2.26, 95% CI 0.95–5.36). The subjects with COPD and bronchiectasis showed poorer pulmonary function (FEV1/FVC: WMD –3.37%, 95% CI –5.63 to –1.11), lower albumin (Standardized mean difference [SMD] –0.17, 95% CI –0.26 to –0.08), elevated C-reactive protein (SMD 0.40, 95% CI 0.06–0.74), a greater proportion of chronic colonization by potentially pathogenic microorganisms (OR 6.65, 95% CI 4.44–9.95), and a higher isolation rate of P. aeruginosa (OR 5.13, 95% CI 4.89–5.38) or H. influenzae (OR 1.90, 95% CI 1.29–2.79) than the subjects with COPD without bronchiectasis.
CONCLUSIONS: This meta-analysis confirmed the significant associations of the presence of bronchiectasis with the natural history, disease course, and outcomes in COPD. The COPD-bronchiectasis phenotype had adverse effects on subjects’ health condition and prognosis.
Introduction
COPD is a common preventable, non-curable, and treatable disease characterized by persistent respiratory symptoms and air-flow limitation owing to airway and/or alveolar abnormalities that are usually caused by significant exposure to noxious particles or gases.1 In practice, there is some overlap between COPD and bronchiectasis. Bronchiectasis is a long-neglected disease, which is currently experiencing a surge in interest. The disease is characterized by irreversible widening of the bronchi and/or branches along with inflammation and chronic bacterial infection.2 The identification of bronchiectasis generally relies on computed tomography, a technique that has significantly increased the sensitivity and monitoring of the diagnosis of bronchiectasis.3 Bronchiectasis and COPD are probably linked and may present in patients in a variety of temporal and causal ways. Bronchiectasis has been proposed as a comorbidity of COPD in the Global Initiative for Chronic Obstructive Lung Disease (GOLD) since 2014.4 Thereafter, the updated version of GOLD highlights the impact of bronchiectasis on health status and prognosis in patients with COPD.5 Reviewing the literature has shown that the coexistence of both COPD and bronchiectasis define an emerging phenotype with a worse prognosis.6 The American Thoracic Society/European Respiratory Society guideline for COPD7 indicated that the COPD-bronchiectasis phenotype has been proposed but still required validation to confirm the relationship with clinically meaningful outcomes.8
In recent years, experts have conducted comparative studies of subjects with COPD with and without bronchiectasis. Two meta-analyses were performed to evaluate the association between COPD and bronchiectasis.9,10 This early research showed that the presence of bronchiectasis in COPD is associated with greater airway inflammation, more frequent and severe exacerbations, more colonization of airway mucosa by a potentially pathogenic microorganism, and, possibly, reduced survival.
However, controversial results on some clinical outcomes still exist in recent studies. For example, Crisafulli et al11 reported that, in subjects with COPD, the presence of bronchiectasis does not influence mortality in a long-term follow-up. Kawamatawong et al12 found no significant association between lower airway bacterial colonization and the presence of bronchiectasis. The impact of bronchiectasis on the natural history of COPD has not been fully evaluated, and no conclusive results are available. Therefore, investigators wanted to further explore the implications of bronchiectasis in patients with COPD. In recent years, a series of new published evidence added additional information on this topic, thus an updated systematic review and a meta-analysis were further performed to clarify the association of demographics, clinical manifestations, and laboratory parameters between subjects with COPD with and without bronchiectasis.
Methods
This systemic review was performed in accordance with the PRISMA 2015 statement.13
Literature Search Strategy for Identification of Studies
A systemic search of PubMed, Embase, Web of Science, and the Cochrane library (Wiley InterScience, Cambridge, United Kingdom) databases was performed for potential English articles by using a combination of search terms up to April 2019, without publication year restrictions. The following search terms were used: (“pulmonary disease, chronic obstructive” [Medical Subject Heading] or “chronic air flow obstruction or chronic airway obstruction” or “chronic obstructive bronchitis” or “COPD” or “chronic obstructive pulmonary disease” or “COAD” or “chronic obstructive airway disease” or “chronic obstructive pulmonary disease” or “air flow obstruction, chronic or air flow obstructions, chronic or chronic air flow obstructions or chronic air flow obstruction”) and (“bronchiectasis [Medical Subject Heading] or bronchiectasis”). The references of potential articles were also manually screened.
Study Selection
Study selection and de-duplication were managed in EndNote X7 (Clarivate Analytics, Philadelphia, Pennsylvania). Titles and abstracts retrieved from the database were screened first and then full texts of potentially eligible studies were obtained and reviewed by 2 authors (SL and MTT) independently. We resolved all disagreements through consensus or recourse to the senior review author (WYX). Multiple studies based on the same sample of participants were treated as duplicates.
Inclusion Criteria
Authors included observational studies that met the following criteria:
On the basis of GOLD guidelines,1 COPD was diagnosed with persistent respiratory symptoms and airflow limitation (post-bronchodilator FEV1/FVC < 0.70).
The presence of bronchiectasis was confirmed by computed tomography and by an experienced pulmonary physician and a pulmonary radiologist (WYX) according to (1) lack of tapering of bronchi, (2) dilation of bronchi if the internal diameter was larger than that of the adjacent pulmonary artery, or (3) visualization of the peripheral bronchi within 1 cm of the pleural surface.14
One or more variables of interest below were compared between the subjects with COPD and with and without bronchiectasis: (1) characteristics, including age, sex, smoking history, body mass index (BMI); (2) clinical manifestations, including daily sputum production, exacerbation rate, hospital admissions, length of hospitalization, and mortality; and (3) pulmonary testing and laboratory parameters, including post-bronchodilator FEV1/FVC, post-bronchodilator FEV1% predicted, C-reactive protein, albumin, colonization by potentially pathogenic microorganisms, P. aeruginosa isolates, and H. influenzae isolates.
Exclusion Criteria
Studies were excluded for any of the following: (1) unable to extract data; (2) not an original publication; (3) bronchiectasis was assessed by chest radiograph only; (4) duplicate data, case reports, letters to editors, systematic reviews, and conference abstracts; or (5) did not meet the inclusion criteria.
Data Extraction and Quality Assessment
The following characteristics were independently collected for each eligible study by 2 investigators (SL and MTT): first author’s name, published year, study design, study period and location, number of participants, and baseline demographic and clinical manifestation of participants, as mentioned above. After extraction, the first author (SL) checked all the data. Two investigators (SL and MTT) independently assessed the quality of the included studies by using the Newcastle-Ottawa Scale, which is a validated quality assessment instrument for observational studies that assesses 3 parameters of quality.15 A score of ≥5 was regarded as a high-quality, a score of <5 or was considered as poor quality.
Ethics Approval
No ethics approval was required because the data were extracted from previously published articles.
Statistical Analysis
A meta-analysis was performed by using the Review Manager software (RevMan v.5.3) (Wiley InterScience, Cambridge, United Kingdom). We presented dichotomous outcomes as odds ratio (OR) and continuous variables as weighted mean differences (WMD), which were weighted according to study sample size, or as standardized mean difference if continuous outcomes were reported in different scales. Pooled effect estimates were also reported with 95% CI. The methods by Hozo et al16 were used to estimate the mean ± SD for those manuscripts that only reported a median. A meta-analysis was performed only on categories with sufficient data. Forest plots were used to display the results graphically. P < .05 was considered statistically significant.
Heterogeneity was statistically evaluated by using the I2 statistic, and the test value with I2 ≥ 50% was considered a substantial level of heterogeneity. The random-effect model was used if the heterogeneity was substantial (I2 ≥ 50%); otherwise, the fixed-effect model was used (I2 < 50%). To investigate possible reasons for heterogeneity, we performed a subgroup analysis and sensitivity analysis. Sensitivity analysis was performed to examine the consistency of the results by excluding each study and redoing the analysis. The method of sensitivity analysis can reduce the heterogeneity of studies to a certain extent. If there was an appropriate number of studies in a pooled analysis, then inverted funnel plots was used to investigate potential publication bias.
Results
The electronic database search yielded 2,082 potentially relevant articles, including 2,076 records identified through database searching and 6 records through other sources. Of all of these, 14 duplicates were removed. After reviewing the titles and abstracts, 76 full-text articles were identified and reviewed, and, finally, 18 studies11,17-33 were included in this systematic review and meta-analysis. The flow diagram of article selection according to the PRISMA guideline13 is illustrated in Figure 1.

Flow chart.
Study Characteristics
A total of 415,257 subjects with COPD from 18 observational studies11,17-33 were eligible for this meta-analysis, and bronchiectasis was present in 25,929 subjects (6.24%). The sample size ranged from 54 to 386,646, and 6 studies17-18,20,22,25,33 had a small population (N < 100). Ten studies11,17-20,25,27-28,32-33 were prospective (cohort studies) and 821-24,26,29-31 were retrospective (case-control studies) in design. The minimum study duration lasted for 1 year and the maximum lasted for 10 years. Research was conducted in 8 countries: England, Spain, Turkey, Egypt, The Republic of North Macedonia, China, Taiwan, and Korea. Subjects were selected from hospitalized, out-patient, or primary care subjects in each included study; their characteristics are described in Table 1. The quality evaluation of the included studies by using the Newcastle-Ottawa Scale is available online (see the supplementary materials at http://www.rcjournal.com). The mean Newcastle-Ottawa Scale quality score across all the studies was 7.8 (range, 7–9) and was evaluated as the high-quality studies because the NOS score was greater than 5.
Basic Characteristics of Included Studies
Demographic Characteristics of Subjects With COPD and With and Without Bronchiectasis
Overall, the pooled data from the 18 studies11,17-33 found that subjects with COPD and with bronchiectasis were older than those without bronchiectasis (WMD 0.57 y, 95% CI 0.45–0.70; P < .001, I2 = 46%). Pooled estimates from the 1611,17-19,21-31 studies found that there were no statistical differences with respect to sex (OR 0.95, 95% CI 0.84–1.09; P = .48, I2 = 66%), as show in Table 2. Ten studies11,19,22-27,28-29,32 were included in the assessment of BMI, and these showed that the presence of bronchiectasis in the subjects with COPD was associated with a lower BMI (WMD –0.42 kg/m2, 95% CI –0.73 to −0.11; P = .007, I2 = 43%) compared with subjects with COPD and without bronchiectasis. Pooled data from the 10 studies11,17-19,20,22,24,26-27,29 showed that there was no significant difference in smoking history (pack-years) (WMD 1.29 pack-years, 95% CI –3.67 to 6.26); P = .61, I2 = 46%) between the subjects with COPD and with and without bronchiectasis.
Demographic Characteristics of the Subjects With COPD and With and Without Bronchiectasis
Sensitivity Analysis and Publications Bias
Sensitivity analysis showed that the robustness of the results did not change after excluding any of the included studies. Publication bias was not observed in age, sex, or BMI, but there was a significant publication bias for smoking history. In the present research, 10 studies11,17-19,21-31 were included in the assessment of smoking history, but we found no significant difference between the groups. A study by Crisafulli et al11 showed that subjects with COPD and bronchiectasis were more frequently former smokers, but our results showed no significant difference in smoking history (pack-years) between groups. Zhang et al26 and Dou et al29 found that the percentage of smokers and the smoking index in subjects with COPD and without bronchiectasis were significantly higher than in those with bronchiectasis. The smoking history of the subjects with COPD and bronchiectasis was also significantly longer. Our results differed from many relevant studies, most likely because of how smoking history was quantified in these studies, usually by the smoking index or with a dichotomous variable of smoking or no smoking. For comparability between studies, we only included results for smoking history in pack-years, which eliminated other research, which led to an analytical bias.
Clinical Manifestation of Subjects With COPD and With and Without Bronchiectasis.
Pooled data from 5 studies17,19,21,23,27 showed that the coexistence of bronchiectasis with COPD was associated with greater daily sputum production (OR 1.80, 95% CI 1.24–2.61; P = .002, I2 = 53%), a higher exacerbation rate over a 12-month period (WMD 0.72 times, 95% CI 0.59–0.85; P < .001, I2 = 94%), and more-frequent hospital admissions (WMD 0.35, 95% CI 0.21–0.49; P < .001, I2 = 0%) compared with COPD without bronchiectasis, as show in Table 3. In addition, pooled data from 3 studies11,28,30 showed that subjects with COPD and bronchiectasis had more-frequent hospital admissions (OR 1.84, 95% CI 1.60–2.11; P < .001, I2 = 48%) compared with those without bronchiectasis. Moreover, 4 studies reported that the length of hospitalization was significantly longer in subjects with COPD who were comorbid for bronchiectasis.11,23,31,34
Clinical Characteristics of the Subjects With COPD and With and Without Bronchiectasis
Six studies11,19,21,23,27,31 reported results for mortality. Time frames varied, with 3 studies21,27,31 that reported in-hospital deaths, and 311,19,23 reported deaths within 3 years. Therefore, subgroup analyses were conducted to estimate the relative risk for all-cause mortality over time. In the subgroup analyses, stratified according to the duration of follow-up, we observed material differences in ORs between studies that reported an in-hospital mortality or follow-up (>3 years) mortality, OR 2.26, 95% CI 0.95–5.36 (P = .07), and OR 0.83, 95% CI 0.78–0.90 (P < .001), respectively. There was greater heterogeneity between studies11,19,23 with a follow-up mortality compared with studies21,27,31 that reported in-hospital mortality (I2 = 82%, P = .004; and I2 = 0%, P = .39, respectively) (see the supplementary materials at http://www.rcjournal.com).
Sensitivity Analysis and Publications Bias
Sensitivity analysis indicated unacceptable levels of heterogeneity among Crisafulli11 and the other studies.19,21,23,27,31 After excluding this study,11 comorbid COPD and bronchiectasis were associated with an increased risk for follow-up mortality (OR 3.37%, 95% CI 1.29–8.79; P = .01, I2 = 76%). Each of the other pooled ORs changed only marginally after omitting successive studies. Significant heterogeneity was observed between studies for each outcome except for hospital admissions. Publication bias was only observed in the exacerbation rate, which was mostly due to clinical heterogeneity of the various study settings and populations. Sensitivity analysis confirmed the stability of our result.
Laboratory Parameters of Subjects With COPD and With and Without Bronchiectasis
In the pooled analysis, the presence of bronchiectasis in the subjects with COPD was associated with a worse pulmonary function, with a lower post-bronchodilator FEV1/FVC (WMD –3.37%, 95% CI –5.63 to –1.11; P = .003, I2 = 86%) (see the supplementary materials at http://www.rcjournal.com) and post-bronchodilator FEV1 % predicted (WMD –6.45%, 95% CI –10.09 to –2.81; P < .001, I2 = 91%).
Pooled estimates found that C-reactive protein levels were elevated (Standardized mean difference [SMD] 0.40, 95% CI 0.06–0.74; P = .02, I2 = 89%) in subjects with COPD and with bronchiectasis. Moreover, 3 studies reported that the fibrinogen level was significantly higher in subjects with COPD and with bronchiectasis compared with subjects without bronchiectasis.17,24,29 In the pooled analysis, subjects with comorbid bronchiectasis and COPD had significantly worse nutritional status, with lower albumin levels (SMD –0.17, 95% CI –0.26 to –0.08; P < .001, I2 = 0%) (Supplementary Fig. 3 [see the supplementary materials at http://www.rcjournal.com]) and lower BMIs (WMD –0.42 kg/m2, 95% CI –0.73 to –0.11; P = .007, I2 = 43%) (see the supplementary materials at http://www.rcjournal.com).
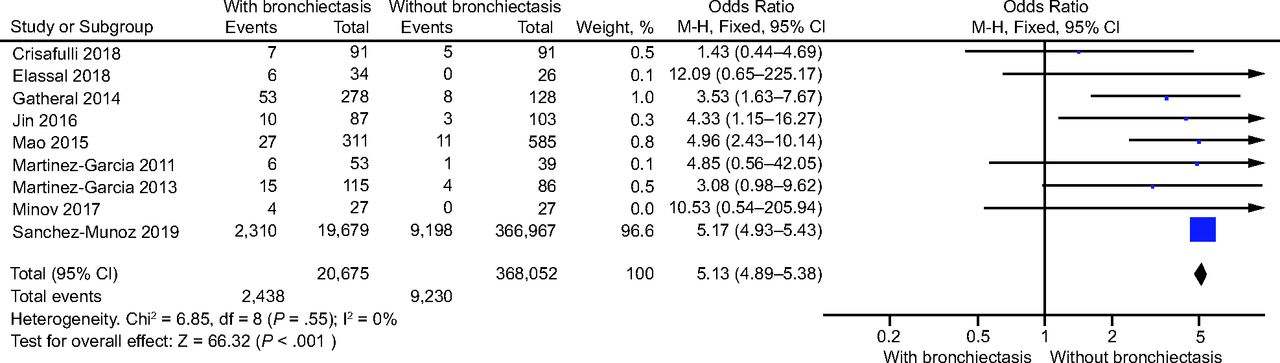
Pooling data found that the presence of bronchiectasis in subjects with COPD was associated with an increased risk for chronic potentially pathogenic microorganism colonization in the airways (OR 6.65, 95% CI 4.44–9.95; P < .001, I2 = 0%) (Fig. 2). Moreover, subjects with COPD and with bronchiectasis showed a higher positive rate of P. aeruginosa (n = 9) (OR 5.13, 95% CI 4.89–5.38; P < .001, I2 = 0%) (Fig. 3) as well as H. influenzae (OR 1.90, 95% CI 1.29–2.79; P = .001, I2 = 17%) (see the supplementary materials at http://www.rcjournal.com).
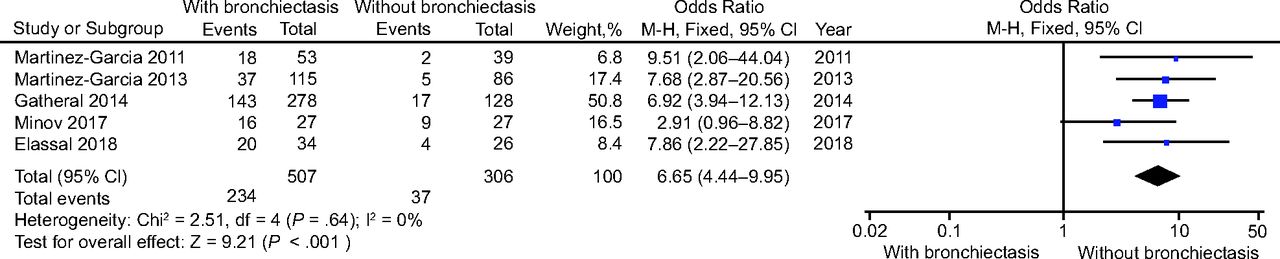
Forest plot of comparison: odds ratio of chronic potentially pathogenic microorganism colonization in subjects with COPD and with and without bronchiectasis.
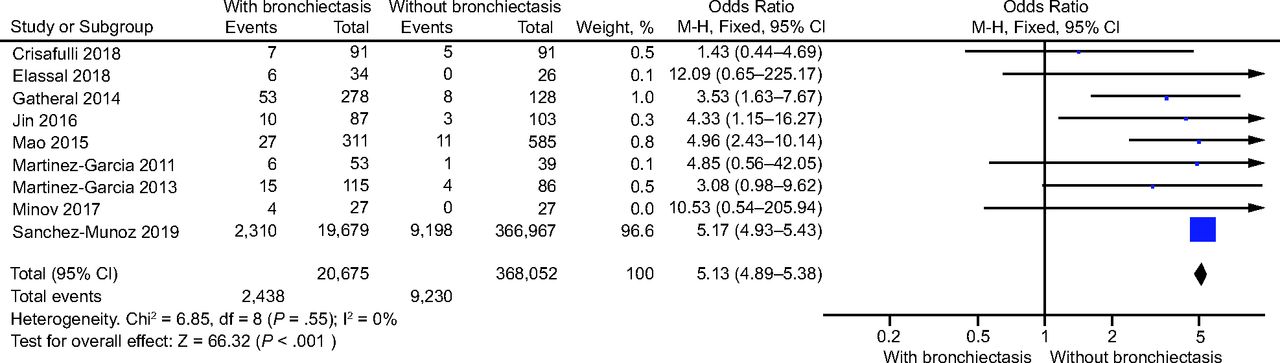
Forest plot of comparison: odds ratio of Pseudomonas aeruginosa (P. aeruginosa) isolation in subjects with COPD and with and without bronchiectasis.
Sensitivity Analysis and Publications Bias
We detected significant between-study heterogeneity in lung function and C-reactive protein. Sensitivity analysis in C-reactive protein showed that removing the studies by Tulek et al,20 Martínez-García et al,19 and Jin et al24 could considerably change the result respectively. That is C-reactive protein level will lower in subjects with COPD and with bronchiectasis compared with subjects without bronchiectasis when removing those studies. The sensitivity analyses after omitting each study showed no material influence on the robustness of the other results. Funnel plots showed no publication bias in post-bronchodilator FEV1/FVC, post-bronchodilator FEV1 predicted, albumin, and microbiologic variables (Fig. 4).

Funnel plots of the laboratory parameters, 442 × 302 mm. BD = bronchodilator, SMD = standard mean difference, WMD = weighted mean difference.
Discussion
This systematic review and meta-analysis summarized the association between multiple outcomes and the presence of bronchiectasis in subjects with COPD. From a demographic point of view, the coexistence of COPD and bronchiectasis occurred more often in older subjects with a lower BMI. As for clinical manifestations, comorbid COPD and bronchiectasis increased the risk of daily sputum production, exacerbation, frequent hospital admissions, longer hospital stays, and mortality. There also were significant differences in laboratory parameters, including poorer pulmonary function, lower albumin, elevated C-reactive protein, a greater proportion of chronic colonization by potentially pathogenic microorganisms, and higher isolation rates of P. aeruginosa and H. influenzae in subjects with COPD and with bronchiectasis. Sensitivity analysis showed that there was no change in the significance of any other outcomes except C-reactive protein and mortality. It indicated that selection bias of demographics and clinical data was small between groups.
In addition, this present study had a number of advantages over the previous meta-analysis. First, the published observational studies, including both case-control studies and cross-sectional studies, were included up to now. Second, to the best of our knowledge, this meta-analysis was the first that compared BMI, hospitalization rate, length of hospital stay, and isolation rates for H. influenzae between subjects with COPD and with and without bronchiectasis.
Bronchiectasis has an increasing profile within pulmonary medicine, with the emerging epidemic of chronic and progressive immune-infective-inflammatory airway disease, which results in a vicious cycle of repeated exacerbations and irreversible damage that now clearly necessitates greater global focus and investment.35 Some previous studies reported a prevalence of bronchiectasis, ranging from 4% to 72%, in subjects with COPD.36 The previous meta-analysis by Du et al10 showed that the mean prevalence of bronchiectasis in subjects with COPD was 54.3%. In contrast, the present meta-analysis showed that the mean prevalence of bronchiectasis in subjects with COPD was 6.24%, which was significantly lower than previous studies.10 There is such a wide range in the prevalence so that the actual prevalence of bronchiectasis in patients with COPD remains unclear. Explanations for the wide variability in reported prevalence include, at least in part, differences in study methodology, inclusion and exclusion criteria of subjects with COPD, GOLD grading of subjects with COPD, subject characteristics, and diagnostic criteria.
For example, only 8.1% of subjects with COPD had bronchiectasis in the study by Dou et al,29 which may be secondary to the exclusion of patients with bronchiectasis that occurred before the age of 40 years, a history of measles and pertussis, or a definite history of pulmonary tuberculosis and overlap of the original site with bronchiectasis from computed tomographies. In the study by Sánchez-Muñoz et al,31 the prevalence of bronchiectasis in subjects with COPD was 5.1%. They selected all admissions of patients with COPD exacerbation and bronchiectasis by International Classification of Diseases, 9th Revision, Clinical Modification code, which might have led to underestimation of the prevalence of bronchiectasis.31
Because the study by Sánchez-Muñoz et al31 had significant weight in this meta-analysis, the current 6.24% prevalence may be an underestimation of the number of subjects who were comorbid for both bronchiectasis and COPD. In fact, establishing a diagnosis of COPD with bronchiectasis is important for future intervention and prevention of disease progression because both diseases have different and complementary therapeutic approaches.37 Therefore, a set of updated consensus criteria is needed for defining radiologic and clinical bronchiectasis in patients with COPD to better estimate the prevalence and the potential prognostic value of identification.
In many chronic lung diseases, there is an age-related increased prevalence given the multifactorial impact of the aging process on respiratory physiology.35 The increasing incidence and prevalence of bronchiectasis in patients with COPD, possibly related to population aging and greater diagnostic awareness, is a significant concern for health-care systems in view of the excess morbidity and mortality, and the high utilization of health-care resources.38 As a chronic comorbidity, bronchiectasis is a prominent contributor to the clinical severity of patients with COPD and often affects patient-centered outcomes.36,37 Patients with COPD and with bronchiectasis showed worse nutritional status, with a lower BMI and albumin than those without bronchiectasis. Measurement of BMI and albumin is a simple method for screening malnutrition.39 A meta-regression published recently assessed the role of biomarkers in describing the severity of malnutrition, the investigators concluded that BMI was a useful marker of malnutrition.40 Qi et al found that an underweight status was highly prevalent among subjects with bronchiectasis.39 BMI has served as an independent prognostic factor for COPD, with a clear association between a low BMI and increased mortality.40 Subjects with a lower BMI were prone to developing more exacerbations, worse pulmonary function, amplified systemic inflammation, and chronic colonization by P. aeruginosa.39 Therefore, BMI was a major determinant of hospitalization and death risks, and thus should be considered in the routine assessment of patients with COPD and with bronchiectasis.
Frequent exacerbations of COPD is the strongest predictor of an unfavorable prognosis in patients with COPD and is associated with a progressive decline in lung function.41 The effect of bronchiectasis on the frequency of exacerbations and rapid lung function decline has been evaluated in previous meta-analyses9,10 and confirmed in this meta-analysis. However, significant heterogeneity (I2 = 94%) was present after doing a random effects meta-analysis, and, therefore, we could not estimate these variables or this variable. A sensitivity analysis confirmed the stability of our results. In addition, we carefully read the included 7 papers that mentioned the assessment of the exacerbation rate, and all these studies showed that comorbid bronchiectasis and COPD were associated with a higher exacerbation rate compared with subjects with COPD alone.17-20,24-26
For the mortality risk, according to a Chinese study, the presence of bronchiectasis was independently associated with mortality during a median 21-month follow-up. Subjects with COPD and with bronchiectasis were 1.77 times more likely to die compared with those without bronchiectasis.23 However, Sánchez-Muñoz et al31 revealed a significant reduction in mortality over time in subjects with COPD and concomitant bronchiectasis (OR 0.97, 95% CI 0.88–1.01). Crisafulli et al11 reported that the presence of bronchiectasis in subjects with COPD did not influence mortality over a 3-year follow-up period. Likewise, our data showed, after subgroup analyses, that comorbid COPD and bronchiectasis directly increased the 3-year mortality but did not influence in-hospital mortality.
However, there was significant heterogeneity (I2 = 76%) in the subgroup analysis for a 3-year follow-up, therefore, we could not provide a meta-analytic estimate. Thus, further research is required to evaluate the effect of the presence of bronchiectasis on mortality risk over time in patients with COPD. In addition, previous studies also reported that cost, length of hospital stay, and number of readmissions were higher in subjects with COPD and with bronchiectasis.42 The presence of bronchiectasis defines a group of patients with COPD who generally seem to have more-severe disease and poorer prognosis.
The most significant results of this meta-analysis were the high OR of chronic potentially pathogenic microorganism colonization, P. aeruginosa, and H. influenzae isolation (6.65, 5.13, and 1.90, respectively). From previous results and data, P. aeruginosa and H. influenzae were the most common bacteria detected in subjects with COPD and with bronchiectasis airways globally.18,43,44 P. aeruginosa can exhibit adaptive behaviors, which allow it to survive in a hostile environment, such as the human airways, and the production of biofilms obstructs exposure of the bacteria to antibiotics and phagocytes. P. aeruginosa also produces virulence factors that allow it to evade phagocyte killing and slow ciliary beat frequency, which further allowed it to maintain its presence.
Patients with chronic infection due to P. aeruginosa have an increased burden of disease, including a higher frequency of exacerbations, worse health-related quality of life, increased risk of hospital admissions, and greater morbidity and mortality.3,45,46 Meanwhile, the major phenotype identified in all cohorts of subjects with bronchiectasis is chronic infection with P. aeruginosa.3 In this sense, this provides a new therapeutic target for such patients, that is, to improve the prognosis by eliminating P. aeruginosa to control disease progression.47 However, a recent study by Millares et al48 found that subjects with stable COPD and with severe disease and P. aeruginosa colonization showed a similar biodiversity to subjects who were not colonized.
Exacerbations in subjects with severe COPD showed the same microbiologic pattern, independent of previous colonization of P. aeruginosa. Analysis of this finding indicated that antibiotic treatments prescribed for exacerbations in patients colonized with P. aeruginosa need to target common potentially pathogenic microorganisms rather than the initial colonization of the potentially pathogenic microorganism.48 Therefore, further investigation needs to be done to gain a deeper understanding of the contribution of the lung microbiome, how host-microbe interactions impact disease, and to search for therapeutic targets for pathogenic microorganisms.
The American Thoracic Society/European Respiratory Society statement7 for COPD recommends more studies to relate potential phenotypic traits with outcomes and enhance understanding of the treatment impact of various COPD phenotypes. Matkovic et al48 indicated that an infective phenotype of COPD could be described as patients with chronic bronchial infection by potentially pathogenic microorganisms during a stable state, recurrent bacterial exacerbation, and frequently associated bronchiectasis. Simply put, the COPD-bronchiectasis phenotype may be a subphenotype or an evolution of the infective phenotype of COPD.49 Just as with previous reports, COPD airway epithelial cells are poorly regenerative and differentiated, reducing the function of the host defense and airway barrier, which makes it susceptible to infections, which leads to persistent inflammation and remodeling.
The same pathogenesis may also induce the development of bronchiectasis.37 It has been proposed that bronchiectasis develops as a result of some various disorders that lead to structural and functional changes in the airways that increase susceptibility to chronic bronchial infections secondary to potentially pathogenic microorganisms. The persistent presence of these organisms causes chronic inflammation, airway remodeling, and further damage to local defense mechanisms, which further enables these potentially pathogenic microorganisms to persist in the airways despite the repeated administration of antibiotics, which thus creates a vicious cycle as proposed by Cole et al.50
Lin et al50 found that COPD-bronchiectasis overlap significantly increases the likelihood of community-acquired pneumonia. Andréjak et al52 reported that bronchiectasis increased the risk of non-tuberculosis mycobacteria infection by 16-fold, with an increase of 29 times in the presence of COPD and inhaled corticosteroid therapy. Therefore, non-tuberculosis mycobacteria infection should be considered in patients with COPD and bronchiectasis. Such evidence may provide more individualized prognostic information.
Understanding the true clinical importance of COPD-bronchiectasis overlap is now critical from an antibiotic stewardship and patient outcomes perspective.53 Many respiratory diseases are associated with a loss of bacterial diversity or by the dominance of a single taxon or small group of taxa,54 which may be related to microaspiration and/or the potential impact of inhaled corticosteroid use and frequent antibiotic use.55 In addition, protection of microbial diversity is associated with epithelial integrity, immune regulation, and colonization resistance, and changes in microbial community composition may impair respiratory health and lead to disease progression.56
This is particularly important because more patients with COPD and bronchiectasis are receiving long-term macrolide treatment, with the potential to induce macrolide resistance in non-tuberculosis mycobacteria if used inappropriately. Thus, these study data are beneficial to further refine the management and treatment of this phenotype. At the clinical level, our findings highlight the importance of sputum surveillance for all patients with COPD with bronchiectasis; at the research level, we advocate for better evidence on the effectiveness of eradication or long-term suppressive therapy for potentially pathogenic microorganism or non-tuberculosis mycobacteria infection.57
Our meta-analysis showed that subjects with COPD and with bronchiectasis had different demographic characteristics, clinical manifestations, and also laboratory parameters, and that these factors were individually associated with prognosis. Therefore, early diagnosis and management of bronchiectasis is of major importance for the prognosis of patients with COPD. Unfortunately, indications or recommendations specifically made for the management of bronchiectasis associated with COPD are not available.
It is important to increase our understanding of the strong correlation between bronchiectasis and the poor prognosis of COPD because it will help ensure that future observational studies include adequate attention for the presence of bronchiectasis among patients with COPD. In the future, well-designed, multi-center longitudinal studies are required to help us better demonstrate the associations of the presence of bronchiectasis in COPD. The subsequent findings may then be translated into preventive strategies to provide an opportunity for early identification and therapeutic intervention aimed at improving the outcome in patients with COPD.
There were several limitations when analyzing and interpreting results in our meta-analysis. There were significant heterogeneities among the studies, especially in the comparison of the continuous data, including smoking history, exacerbations, C-reactive protein, and lung function. This could be due to differences in study sample size, year of publication, length of follow-up, diagnostic criteria for bronchiectasis, and outcome definitions. We expected to address this by using random-effects and sensitivity analyses. However, significant heterogeneity was present after doing a random-effects meta-analysis on sex, smoking, daily sputum, mortality in follow-up, exacerbation, lower post-bronchodilator FEV1 and FEV1% predicted, and C-reactive protein. Therefore, there was no meta-analytic estimate due to heterogeneity.
Conclusions
This systematic review and meta-analysis confirmed the significant associations of the presence of bronchiectasis with the natural history, disease course, and outcomes in COPD. COPD-bronchiectasis phenotype has adverse effects on patients’ health condition and prognosis. Determining the diagnosis is important because it could have a bearing on optimal management. Further research is now required to understand the etiology and pathogenesis of this phenotype and to determine strategies for its prevention and treatment.
Acknowledgment
We thank ZT Pang for her advice regarding the English editing of this manuscript.
Footnotes
- Correspondence: Yixin Wan MD, Department of Respiratory Medicine, Lanzhou University Second Hospital, Cuiyingmen 82, Chengguan District, Lanzhou 730030, Gansu Province, China. E-mail: 861105766{at}qq.com
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}