

Abstract
BACKGROUND: Nocturnal noninvasive ventilation is recommended for patients with hypercapnic COPD. Long-term oxygen therapy improves survival in patients with hypoxemic disease. However, leaks during noninvasive ventilation are likely to reduce the fraction of inspired oxygen.
OBJECTIVES: To compare nocturnal inspired O2 fractions during noninvasive ventilation with daytime pharyngeal inspired O2 fractions during nasal cannula oxygen therapy (with the same O2 flow) in patients with COPD at home (ie, real-life conditions).
METHODS: This single-center prospective observational study included 14 subjects with COPD who received long-term O2 therapy. We analyzed pharyngeal inspired O2 fractions in the evening, with a nasopharyngeal probe (sidestream gas analyzer). The O2 flow was measured with a precision flow meter, at the usual flow. Then, the same O2 flow was implemented for noninvasive ventilation with a study’s home ventilator. The all-night noninvasive ventilation parameters were delivered in pressure mode with a single-limb leaking circuit. Daytime and nighttime inspired O2 fractions were compared.
RESULTS: The mean ± SD daytime pharyngeal inspired O2 fraction, measured with normobaric basal O2 flow, 0.308 ± 0.026%, was significantly higher than the mean ± SD nighttime inspired O2 fraction, measured during noninvasive ventilation (0.251 ± 0.011; P < .001).
CONCLUSIONS: The nighttime inspired O2 fraction decreased with a modern noninvasive ventilation pattern, pressure target, and intentional leaks. This partial lack of O2 therapy is likely to be harmful. It might explain the poor results in all but 2 randomized controlled trials on long-term noninvasive ventilation in COPD. (ClinicalTrials.gov registration NCT02599246.)
Introduction
Long-term oxygen therapy improves survival in patients with hypoxemic COPD.1,2 The minimum recommended duration of O2 therapy is 15 h/d.3 Noninvasive ventilation (NIV) is currently recommended for acute-on-chronic COPD respiratory distress, and chronic NIV use is recommended for hypercapnic COPD.4 However, the recent Global Initiative for COPD proposed that NIV should be used in selected patients.3 A number of clinical studies found that nocturnal NIV application improved the quality of life, blood gas values, and hospital admission rates.5,6 Two studies recently demonstrated a reduction in mortality with chronic NIV use in subjects with COPD.7,8 Most home ventilators deliver pressure support via a turbine and a constant O2 supply.9,10 In contrast, ICU ventilators have an integrated blender that delivers the appropriate O2 levels for achieving the set  during NIV. Because most home-care ventilators lack this delivery mode, we hypothesized that intentional and nonintentional leaks could influence the
during NIV. Because most home-care ventilators lack this delivery mode, we hypothesized that intentional and nonintentional leaks could influence the  of the patient. Modern home ventilators compensate for leaks by delivering higher flows. However, the flow is increased with additional intake from room air (ie,
of the patient. Modern home ventilators compensate for leaks by delivering higher flows. However, the flow is increased with additional intake from room air (ie,  = 0.21); thus, without changing the O2 supply, the
= 0.21); thus, without changing the O2 supply, the  must decrease. To our knowledge, few clinical studies have assessed the
must decrease. To our knowledge, few clinical studies have assessed the  delivered with a home-care ventilator.11 In the present study, we aimed to compare the daytime
delivered with a home-care ventilator.11 In the present study, we aimed to compare the daytime  , when O2 was supplied with a nasal cannula, to the nighttime
, when O2 was supplied with a nasal cannula, to the nighttime  , when O2 was supplied with NIV at the same O2 flow, in patients with COPD, under real conditions, at the patient’s home.
, when O2 was supplied with NIV at the same O2 flow, in patients with COPD, under real conditions, at the patient’s home.
Quick Look
Current Knowledge
Physiologic effects of noninvasive ventilation (NIV) should counteract COPD ventilation disorders. Surprisingly, only 2 recent randomized study’s showed mortality benefit to routine use of NIV in COPD. Only one study compared  with normobaric oxygen with
with normobaric oxygen with  with NIV in COPD but during daytime in laboratory conditions.
with NIV in COPD but during daytime in laboratory conditions.
What This Paper Contributes to Our Knowledge
In a physiologic observational study, we showed that the inspired fraction of oxygen is dramatically decreased by NIV. If we consider O2 treatment as the number of  points above 0.21, half of O2 treatment was removed during NIV in our study. This partial withdrawing of an important treatment could explain the unexpected poor result of chronic NIV for COPD.
points above 0.21, half of O2 treatment was removed during NIV in our study. This partial withdrawing of an important treatment could explain the unexpected poor result of chronic NIV for COPD.
Methods
Study Design
This single-center, prospective, observational study was conducted at the Military Teaching Hospital Sainte Anne, Toulon, France. The study protocol was reviewed and approved by the French ethical committee of the CPP Méditerranée I (2015-A01087-42), and it was registered at clinicaltrials.gov registration NCT02599246.
Study Participants
Eligible patients had COPD and received both normobaric long-term oxygen therapy and nighttime NIV at the same O2 flow according to French common practice. Subjects were screened by the lung specialist at our hospital and 2 intensivists (PG, MC), who prescribed long-term oxygen therapy and NIV to patients with COPD. All the subjects provided signed informed consent. Exclusion criteria were the following: acute respiratory failure, history of cranial traumatism, history of epistaxis, local anesthetic intolerance, and high dependence on O2 supply (O2 flow of >3 L/min). We also excluded any patient who wanted to stop the study and withdrew consent.
Study End Points
The primary end point was the difference between the  measured during NIV and the
measured during NIV and the  measured during daytime long-term oxygen therapy with a nasal cannula. The O2 flow was similar in both treatments for each patient. The secondary end points were the following: the time spent below different reference O2 levels during NIV (despite constant O2 flow) and the level of O2 adjustment needed to maintain a stable
measured during daytime long-term oxygen therapy with a nasal cannula. The O2 flow was similar in both treatments for each patient. The secondary end points were the following: the time spent below different reference O2 levels during NIV (despite constant O2 flow) and the level of O2 adjustment needed to maintain a stable  during NIV.
during NIV.
Data Collection and Measurements
We prospectively collected data on demographics, O2 flow, the last arterial blood gas measurements, and spirometry for each subject. All subjects were studied in their home environment, and data collection started in the evening. The pharyngeal  was measured during the day, whereas O2 was delivered with a nasal cannula. Briefly, after local anesthesia, a nasopharyngeal cannula (Vygon SA, Paris, France) was introduced (an assembly diagram is provided, see the supplementary materials at http://www.rcjournal.com). Pharyngeal gases were analyzed with a side-stream gas analyzer (G5 gas module, Intellivue MP70 Philips, Philips Healthcare, Suresnes, France). The O2 source was a 15-L hyperbaric bottle (Air Liquide SA, Paris, France). The O2 flow was controlled with a precision flow meter (VT305 Gamida, Gamida SA, Paris, France). Several different O2 flow were applied, and the corresponding
was measured during the day, whereas O2 was delivered with a nasal cannula. Briefly, after local anesthesia, a nasopharyngeal cannula (Vygon SA, Paris, France) was introduced (an assembly diagram is provided, see the supplementary materials at http://www.rcjournal.com). Pharyngeal gases were analyzed with a side-stream gas analyzer (G5 gas module, Intellivue MP70 Philips, Philips Healthcare, Suresnes, France). The O2 source was a 15-L hyperbaric bottle (Air Liquide SA, Paris, France). The O2 flow was controlled with a precision flow meter (VT305 Gamida, Gamida SA, Paris, France). Several different O2 flow were applied, and the corresponding  was measured. The measurement of
was measured. The measurement of  was done during closed mouth breathing. We started with the baseline flow (the subject’s habitual O2 flow) and then tested 150, 75, 50, and 25% of the baseline flow. For example, when the subject’s baseline O2 flow was 2 L/min, we measured pharyngeal
was done during closed mouth breathing. We started with the baseline flow (the subject’s habitual O2 flow) and then tested 150, 75, 50, and 25% of the baseline flow. For example, when the subject’s baseline O2 flow was 2 L/min, we measured pharyngeal  at O2 supply flows of 3, 2, 1, and 0.5 L/min. The
at O2 supply flows of 3, 2, 1, and 0.5 L/min. The  was noted when stabilized for at least 8 cycles.
was noted when stabilized for at least 8 cycles.
In a second phase, the subjects’ prescribed NIV parameters were entered into the home ventilator controller (Vivo 50; Breas Medical AB, Mölnlycke, Sweden). The ventilator was equipped with an  sensor (E-17/J, Nuova, Ratzeburg, Germany) connected at the air outlet of the ventilator. The
sensor (E-17/J, Nuova, Ratzeburg, Germany) connected at the air outlet of the ventilator. The  sensor was calibrated at the hospital site, immediately before going to the patient’s home. The measurements were compared with the measurements obtained with an O2 gas analyzer. Once the ventilator was in place, after removing the pharyngeal probe to avoid increasing leaks, we checked the accuracy of the ventilation parameters and the comfort of the mask (Comfort gel facial mask, Philips Respironics, Suresnes, France). All subjects used the same type of mask to standardize the intentional leak. To test the adequacy of the settings, we checked the
sensor was calibrated at the hospital site, immediately before going to the patient’s home. The measurements were compared with the measurements obtained with an O2 gas analyzer. Once the ventilator was in place, after removing the pharyngeal probe to avoid increasing leaks, we checked the accuracy of the ventilation parameters and the comfort of the mask (Comfort gel facial mask, Philips Respironics, Suresnes, France). All subjects used the same type of mask to standardize the intentional leak. To test the adequacy of the settings, we checked the  delivered by the ventilator at the basal O2 flow, then we titrated the O2 flow to achieve the same
delivered by the ventilator at the basal O2 flow, then we titrated the O2 flow to achieve the same  as that measured during daytime oxygen therapy at the basal O2 flow. Before we left the subject’s home, we installed the ventilator in the subject’s bedroom; the O2 supply was set at the basal flow, controlled with the precision flow meter. We also measured the
as that measured during daytime oxygen therapy at the basal O2 flow. Before we left the subject’s home, we installed the ventilator in the subject’s bedroom; the O2 supply was set at the basal flow, controlled with the precision flow meter. We also measured the  near the ventilator, but, on our home ventilators, O2 was admitted at the rear of the ventilator, which probably provided a perfect mixing of gases through the turbine; therefore, the
near the ventilator, but, on our home ventilators, O2 was admitted at the rear of the ventilator, which probably provided a perfect mixing of gases through the turbine; therefore, the  was unlikely to be overestimated. Also, the ventilator flow monitoring was exact because O2 was admitted before the flow meter. Subjects received the prescribed NIV nighttime treatment. The next morning, the subject was visited again, and all materials were retrieved.
was unlikely to be overestimated. Also, the ventilator flow monitoring was exact because O2 was admitted before the flow meter. Subjects received the prescribed NIV nighttime treatment. The next morning, the subject was visited again, and all materials were retrieved.
The recorded ventilator parameters from the night recordings were analyzed with Breas software (software that allows recovery of the recorded ventilator parameters and that extracts them in the form of an Excel table, Microsoft Ireland Operations, Dublin, Ireland). For each breath, the following parameters were available:  , tidal volume, total flow (from the ventilator), minute volume (of the patient), and breathing frequency. With the ventilator (Vivo 50, Breas) intentional leaks (from the mask) and nonintentional leaks are not distinguished. Therefore, we calculated the mean airway pressure for each subject to estimate the intentional leaks (due to the mask).
, tidal volume, total flow (from the ventilator), minute volume (of the patient), and breathing frequency. With the ventilator (Vivo 50, Breas) intentional leaks (from the mask) and nonintentional leaks are not distinguished. Therefore, we calculated the mean airway pressure for each subject to estimate the intentional leaks (due to the mask).
Statistical Analysis
For this observational study with consecutive sampling, we performed a statistical power analysis with α = 0.05, β = 0.2, and an estimated 6.375% drop in  overnight compared with the daytime
overnight compared with the daytime  . The analysis indicated that at least 10 subjects should be included. This analysis was based on a 9-subjects sample in which the same measurement was done in a short NIV trial in an ICU. (see the supplementary materials at http://www.rcjournal.com.)
. The analysis indicated that at least 10 subjects should be included. This analysis was based on a 9-subjects sample in which the same measurement was done in a short NIV trial in an ICU. (see the supplementary materials at http://www.rcjournal.com.)
All statistical analyses were performed with Graph Pad Prism version 6.5 (GraphPad software, San Diego). Continuous data are reported as the mean ± SD. The Shapiro-Wilk test was applied to test the normal distribution of data. When data were not normally distributed, we reported the median and interquartile range [25th–75th percentile]. Nominal variables are reported as the number and proportion (%). A univariate analysis was conducted with the chi-square test to compare categorical variables. The Wilcoxon signed-rank test and Student t test were used to compare continuous variables (medians and means, respectively) between groups. For all tests, P < .05 was considered statistically significant.
Results
Between December 2015 and March 2016, we enrolled 14 subjects in the study, 11 men and 3 women, with a mean ± SD age of 71 ± 1.65 y. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) classification of air-flow limitation,3 we classified 6 subjects as GOLD stage 4, 5 subjects as GOLD stage 3, and 3 subjects as GOLD stage 2. All the subjects were previously prescribed a treatment with nighttime pressure-support ventilation; the O2 flow and ventilator settings are summarized in Table 1.
Subject Characteristics and Ventilators Setting
Day Time Pharyngeal 

The mean ± SD pharyngeal  with a normobaric baseline O2 flow was 0.308 ± 0.026. The mean ± SD
with a normobaric baseline O2 flow was 0.308 ± 0.026. The mean ± SD  gain was 2.6 ± 0.7 points above 0.21 for each 0.5 L/min increase in O2 supply.
gain was 2.6 ± 0.7 points above 0.21 for each 0.5 L/min increase in O2 supply.
Daytime NIV Short Adaptation Trial
The mean  measured during a daytime NIV trial was 0.244. The mean ± SD NIV O2 flow that was required to reach an
measured during a daytime NIV trial was 0.244. The mean ± SD NIV O2 flow that was required to reach an  equal to the previous pharyngeal
equal to the previous pharyngeal  was 4.7 ± 1.4 L/min, equivalent to a mean ± SD increase in the baseline flow by 2.5 ± 0.7–fold.
was 4.7 ± 1.4 L/min, equivalent to a mean ± SD increase in the baseline flow by 2.5 ± 0.7–fold.
Nighttime NIV
We recorded 104 h 22 min of nocturnal NIV in 14 subjects. The mean ± SD individual NIV use was 7 h 27 min ± 1 h 3 min. The mean flow from nonintentional leaks was 4 L/min.
during Nighttime NIV

The  values (recorded breath by breath) during nocturnal NIV were compared with the subjects’ own daytime pharyngeal
values (recorded breath by breath) during nocturnal NIV were compared with the subjects’ own daytime pharyngeal  level at the same O2 flow. The results of all 14 subjects showed that the mean ± SD nighttime
level at the same O2 flow. The results of all 14 subjects showed that the mean ± SD nighttime  measurement (0.251 ± 0.01) was much lower than the mean ± SD daytime measurement (0.308 ± 0.026; P < .001) (Fig. 1). For each subject, we stratified the nighttime
measurement (0.251 ± 0.01) was much lower than the mean ± SD daytime measurement (0.308 ± 0.026; P < .001) (Fig. 1). For each subject, we stratified the nighttime  according to the daytime measured at the baseline O2 flow and at 75, 50, and 25% of the baseline O2 flow. During nocturnal NIV, none of the subjects achieved a
according to the daytime measured at the baseline O2 flow and at 75, 50, and 25% of the baseline O2 flow. During nocturnal NIV, none of the subjects achieved a  that corresponded to the
that corresponded to the  recorded during the day with baseline O2 flow.
recorded during the day with baseline O2 flow.

Nighttime  during noninvasive ventilation (NIV) and daytime pharyngeal
during noninvasive ventilation (NIV) and daytime pharyngeal  during oxygen therapy, measured at the same O2 flow. Values show the mean ± SD. LTOT = long-term oxygen therapy.
during oxygen therapy, measured at the same O2 flow. Values show the mean ± SD. LTOT = long-term oxygen therapy.
Twelve subjects spent the entire night with an  level below the
level below the  level that corresponded to 75% of baseline flow (ie, 1.5 L/min for a subject with 2 L/min baseline flow). Three subjects spent the entire night with an
level that corresponded to 75% of baseline flow (ie, 1.5 L/min for a subject with 2 L/min baseline flow). Three subjects spent the entire night with an  level below the
level below the  level that corresponded to 50% of baseline flow. When considering the entire patient population (N = 14), the
level that corresponded to 50% of baseline flow. When considering the entire patient population (N = 14), the  measured during NIV was below the baseline
measured during NIV was below the baseline  flow level for 100% of the time; below the 75%-flow
flow level for 100% of the time; below the 75%-flow  level for 99% of the time; below the 50%-flow
level for 99% of the time; below the 50%-flow  level for 47% of time; and below the 25%-flow
level for 47% of time; and below the 25%-flow  level for 20% of the time (Fig. 2). The mean nonintentional leakage was low in our study: 4 L/min.
level for 20% of the time (Fig. 2). The mean nonintentional leakage was low in our study: 4 L/min.
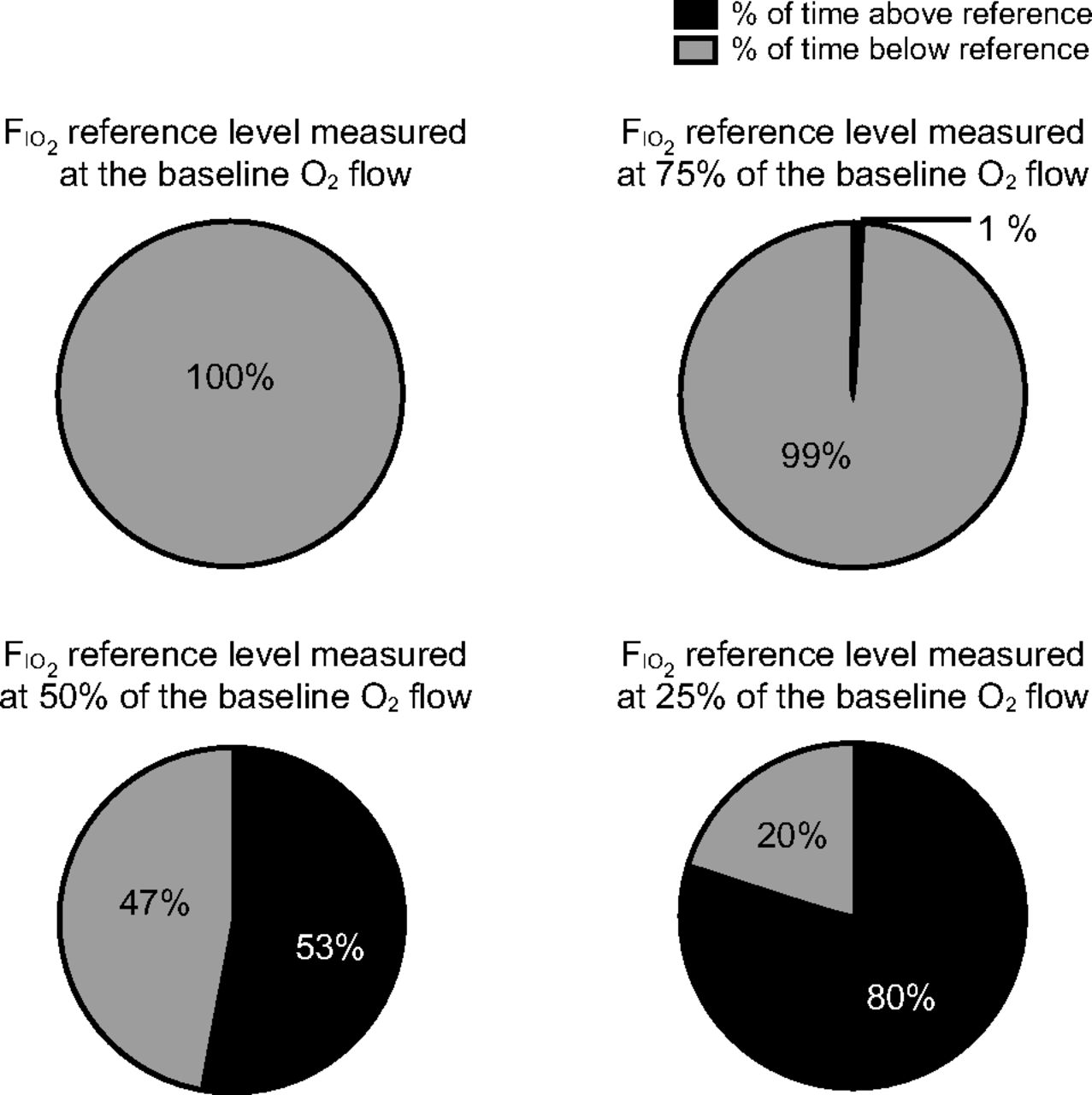
The percentage of the time that the noninvasive ventilation supported  levels were above or below the daytime
levels were above or below the daytime  reference levels, measured at different O2 flows.
reference levels, measured at different O2 flows.
Variability of Nighttime

Because of the latency of the chemical O2 probe, we could not directly correlate  and turbine flow. We found a good correlation between the SD of the turbine flow and SD of
and turbine flow. We found a good correlation between the SD of the turbine flow and SD of  : R2 0.48 (Fig. 3).
: R2 0.48 (Fig. 3).

Linear regression between  SD and total-flow SD.
SD and total-flow SD.
Discussion
To our knowledge, this study was the first to compare daytime pharyngeal  , measured during normobaric O2 flow, with nighttime
, measured during normobaric O2 flow, with nighttime  , measured during NIV with the same O2 flow, in subjects with COPD. Moreover, measurements were performed at home in the real condition of NIV use with the mode, ventilator settings, and circuit used on a daily basis by the subjects. Our main finding was that, with NIV, the nighttime
, measured during NIV with the same O2 flow, in subjects with COPD. Moreover, measurements were performed at home in the real condition of NIV use with the mode, ventilator settings, and circuit used on a daily basis by the subjects. Our main finding was that, with NIV, the nighttime  (mean ± SD 0.251 ± 0.011) was much lower than that achieved during daytime O2 therapy (mean ± SD 0.308 ± 0.026; P < .001).
(mean ± SD 0.251 ± 0.011) was much lower than that achieved during daytime O2 therapy (mean ± SD 0.308 ± 0.026; P < .001).
Few previous studies measured pharyngeal  during low O2 flow. The most relevant was performed by Wettstein et al.12 They reported a pharyngeal
during low O2 flow. The most relevant was performed by Wettstein et al.12 They reported a pharyngeal  of 0.30 when O2 was delivered at 2 L/min through a nasal cannula in 20 subjects. However, that study was conducted under physiologic conditions in healthy volunteers. Bazuaye et al13 studied
of 0.30 when O2 was delivered at 2 L/min through a nasal cannula in 20 subjects. However, that study was conducted under physiologic conditions in healthy volunteers. Bazuaye et al13 studied  in subjects with COPD who received O2 at 2 L/min through a nasal cannula. The mean ± SD
in subjects with COPD who received O2 at 2 L/min through a nasal cannula. The mean ± SD  at 2 L/min was 0.293 ± 0.137 (indirect measurement). In our study, the mean ± SD daytime
at 2 L/min was 0.293 ± 0.137 (indirect measurement). In our study, the mean ± SD daytime  of 0.304 ± 0.62 was consistent with previous findings, but we measured
of 0.304 ± 0.62 was consistent with previous findings, but we measured  directly in the subjects with COPD. With an average
directly in the subjects with COPD. With an average  gain of 0.0245 above 0.21 for each 0.5 L/min increase in O2 supply, our findings are a little above the common 0.02
gain of 0.0245 above 0.21 for each 0.5 L/min increase in O2 supply, our findings are a little above the common 0.02  gain for each 0.5 L/min of O2 supply.
gain for each 0.5 L/min of O2 supply.
It is well established that NIV has numerous positive physiologic effects in COPD. In one study, NIV reduced the effort in breathing and increased endurance muscle strength, counteracted intrinsic PEEP, and improved gas exchange.14 Therefore, it is surprising that so few studies demonstrate an impact of NIV on mortality. This lack of benefit might be explained by our finding that the  decreased during nighttime NIV. Moreover, we believe that leakages were the key cause of the drop in
decreased during nighttime NIV. Moreover, we believe that leakages were the key cause of the drop in  .In fact, previous studies showed that
.In fact, previous studies showed that  could decrease with O2 leaks during NIV.11 Samolski et al15 studied 10 healthy volunteers to evaluate determinants in
could decrease with O2 leaks during NIV.11 Samolski et al15 studied 10 healthy volunteers to evaluate determinants in  with intermittent positive pressure. They found that continuous airway pressure provided greater
with intermittent positive pressure. They found that continuous airway pressure provided greater  than bi-level positive airway pressure.15 The investigators explained this result by showing that important leaks were present with bi-level positive airway pressure.15
than bi-level positive airway pressure.15 The investigators explained this result by showing that important leaks were present with bi-level positive airway pressure.15
Storre et al16 investigated the effects of leaks. First, they showed that leakage might be better compensated with ventilators that were pressure limited rather than volume limited.16 Recently, they studied oxygen supplementation in noninvasive home mechanical ventilation.17 They compared  in subjects who received daytime ventilation with 4 different kinds of ventilatory circuits; leakages led to worse
in subjects who received daytime ventilation with 4 different kinds of ventilatory circuits; leakages led to worse  levels.17 The highest
levels.17 The highest  level was achieved with an active valve circuit with no artificial leak; and the lowest
level was achieved with an active valve circuit with no artificial leak; and the lowest  level was achieved with intentional and artificial leaks.17 In the latter configuration, they found mean
level was achieved with intentional and artificial leaks.17 In the latter configuration, they found mean  levels of 0.249 near the mask and 0.33 near the ventilator.17 With the “no leak” circuit, the mean
levels of 0.249 near the mask and 0.33 near the ventilator.17 With the “no leak” circuit, the mean  levels were 0.362 and 0.33, respectively.17 The difference represented a 16.7 mm Hg
levels were 0.362 and 0.33, respectively.17 The difference represented a 16.7 mm Hg  drop between the “no leak” and “maximal leak” circuits. These investigators found a higher
drop between the “no leak” and “maximal leak” circuits. These investigators found a higher  than that found in our study with NIV. This difference could be explained by the higher O2 flow used in their study (2.7 L/min vs 1.9 L/min17) and probably by the greater leaks that occurred during nighttime NIV, particularly with the mask we used. Indeed, our mask had intentional leaks of 18.9, 27.4, and 39.4 L/min at pressures of 5, 10, and 20 cm H2O, respectively.18
than that found in our study with NIV. This difference could be explained by the higher O2 flow used in their study (2.7 L/min vs 1.9 L/min17) and probably by the greater leaks that occurred during nighttime NIV, particularly with the mask we used. Indeed, our mask had intentional leaks of 18.9, 27.4, and 39.4 L/min at pressures of 5, 10, and 20 cm H2O, respectively.18
What is the clinical impact of these results? Long-term oxygen therapy is currently recommended in severe COPD for at least 15 h/d.5 We found that, during nocturnal NIV (average time, 7 h 20 min), 50% of the time, the  was below the
was below the  measured at half the flow needed for adequate oxygen therapy. Alveolar hypoxia is known to induce pulmonary vasoconstriction, and long-term oxygen therapy was shown to lower or to stabilize pulmonary hypertension.19,20 Therefore, we should be concerned about delivering constant O2 treatment.21
measured at half the flow needed for adequate oxygen therapy. Alveolar hypoxia is known to induce pulmonary vasoconstriction, and long-term oxygen therapy was shown to lower or to stabilize pulmonary hypertension.19,20 Therefore, we should be concerned about delivering constant O2 treatment.21
Although high-intensity NIV might seem to be more effective,8 in fact, the  decreased further during high-pressure ventilation.22 Several studies demonstrated that applying the highest pressure led to the greatest leaks,22-24 which, in turn, led to lower
decreased further during high-pressure ventilation.22 Several studies demonstrated that applying the highest pressure led to the greatest leaks,22-24 which, in turn, led to lower  levels. We believed that withdrawing half of the O2 treatment during the night would worsen pulmonary hypertension evolution.
levels. We believed that withdrawing half of the O2 treatment during the night would worsen pulmonary hypertension evolution.
According to the GOLD recommendation,3 the aim of chronic NIV use is to clear the CO2. Mask exhalation ports reduce CO2 rebreathing.3,25,26 Therefore we must not avoid an intentional leak.
Should we maintain  throughout the night? During the short evening NIV trial that we performed to allow the subjects to adapt to the mask and ventilator settings, we titrated the O2 flow to achieve the previous pharyngeal
throughout the night? During the short evening NIV trial that we performed to allow the subjects to adapt to the mask and ventilator settings, we titrated the O2 flow to achieve the previous pharyngeal  level obtained at the baseline O2 flow (nasal cannula). The daytime
level obtained at the baseline O2 flow (nasal cannula). The daytime  was achieved with NIV by increasing the baseline O2 flow by an average of 2.46-fold (minimum, 1.5-fold; maximum, 4.25-fold). Modern O2 concentrators are able to achieve those O2 flows. Thus, the increase in the O2 flow could correct the decrease in
was achieved with NIV by increasing the baseline O2 flow by an average of 2.46-fold (minimum, 1.5-fold; maximum, 4.25-fold). Modern O2 concentrators are able to achieve those O2 flows. Thus, the increase in the O2 flow could correct the decrease in  linked to leaks. However, an increase in the patient’s inspiratory effort will also result in an increase in the turbine flow and, therefore, in a decrease in
linked to leaks. However, an increase in the patient’s inspiratory effort will also result in an increase in the turbine flow and, therefore, in a decrease in  despite the increase in the O2 flow.
despite the increase in the O2 flow.
Limitations
This study had the limitations inherent in an observational physiologic study. The  measurement during nasal cannula O2 delivery was done only once, with the patient’s mouth closed. But this one-time measurement may not reflect the O2 delivery consistency over the entire daytime and especially during the increase of the subject’s inspiratory efforts. We did not perform a second-night measurement, in which we increased the O2 flow; therefore, we could only hypothesize that increasing the flow might correct the
measurement during nasal cannula O2 delivery was done only once, with the patient’s mouth closed. But this one-time measurement may not reflect the O2 delivery consistency over the entire daytime and especially during the increase of the subject’s inspiratory efforts. We did not perform a second-night measurement, in which we increased the O2 flow; therefore, we could only hypothesize that increasing the flow might correct the  . Further prospective studies that evaluate long-term NIV in subjects with COPD should pay attention to nighttime
. Further prospective studies that evaluate long-term NIV in subjects with COPD should pay attention to nighttime  levels.
levels.
Conclusions
We demonstrated that, with a modern NIV pattern of application, a pressure target, and intentional leaks, the nighttime  decreased during NIV in subjects with COPD. We speculated that this partial reduction in O2 therapy might be harmful. Moreover, it might explain the poor results reported previously, in all but 2 randomized controlled trials on long-term NIV in COPD.9,24
decreased during NIV in subjects with COPD. We speculated that this partial reduction in O2 therapy might be harmful. Moreover, it might explain the poor results reported previously, in all but 2 randomized controlled trials on long-term NIV in COPD.9,24
Footnotes
- Correspondence: Michael Cardinale MD, Fédération d’Anesthésie – Réanimation. Hôpital d’Instruction des Armées Sainte-Anne. Boulevard Sainte-Anne. BP 20545 - 83041 Toulon Cedex 9, France. E-mail: mickaelcardinale{at}hotmail.fr
Dr Goutorbe discloses a relationship with Breas Medical, in addition, Dr Goutorbe has a patent systems and methods for automatically adjusting a determined supply of FIO2 generated from a CPAP, NIV or other ventilator system issued. Dr Arnal discloses a relationship with Hamilton Medical. The remaining authors have no conflict of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
The study was performed at Military Teaching Hospital Sainte Anne, Toulon, France.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}