

Abstract
BACKGROUND: Commonly used thresholds for staging FEV1 have not been evaluated as standalone spirometric predictors of death in older persons. Specifically, the proportion of deaths attributed to a reduced FEV1, when staged by commonly used thresholds in L, percent of predicted (% pred), and Z scores, has not been previously reported.
METHODS: In 4,232 white persons ≥ 65 y old, sampled from the Cardiovascular Health Study, FEV1 was stratified as stage 1 (FEV1 ≥ 2.00 L, ≥80% pred, and Z score ≥−1.64), stage 2 (FEV1 1.50–1.99 L, 50–79%pred, and Z score −2.55 to −1.63), and stage 3 (FEV1 < 1.50 L, < 50% pred, and Z score < −2.55). Notably, a Z score threshold of −1.64 defines normal-for-age lung function as the lower limit of normal (ie, 5th percentile of distribution), and accounts for differences in age, sex, height, and ethnicity. Next, adjusted odds ratios and average attributable fractions for 10-y all-cause mortality were calculated, comparing FEV1 stages 2 and 3 against stage 1, expressed in L, % pred, and Z scores. The average attributable fraction estimates the proportion of deaths attributed to a predictor by combining the prevalence of the predictor with the relative risk of death conferred by that predictor.
RESULTS: FEV1 stage 2 and 3 in L, % pred, and Z scores yielded similar adjusted odds ratios of death: 1.40–1.51 for stage 2 and 2.35–2.66 for stage 3. Conversely, FEV1 stages 2 and 3 in L, % pred, and Z scores differed in prevalence: 12.8–28.6% for stage 2 and 6.4–17.5% for stage 3, and also differed in the adjusted average attributable fraction for death: 3.2–6.4% for stage 2 and 4.5–9.1% for stage 3.
CONCLUSIONS: In older persons, the proportion of deaths attributed to a reduced FEV1 is best stratified by Z score staging thresholds because these yield a similar relative risk of death but a more age- and sex-appropriate prevalence of FEV1 stage.
Introduction
The spirometric evaluation of lung function frequently includes FEV1 and FVC because these establish normal-for-age spirometry and the impairments of restrictive-pattern and air-flow obstruction.1–5 In older persons, however, values for FVC are less likely to meet quality control testing criteria than values for FEV1.6 This is because FVC is more effort-dependent, requiring a maximal and sustained forced exhalation from full inspiration to the lowest residual lung volume, whereas FEV1 is the expired volume in the first second of the FVC maneuver.1
Accordingly, the spirometric evaluation of older persons may be limited to FEV1.6 Such an approach, wherein FEV1 is interpreted as a standalone spirometric measure, has value for at least 3 reasons. First, because it predicts the maximum attainable ventilation during exercise, a low FEV1 establishes a reduced ventilatory capacity.7 Second, a low FEV1 in older persons is associated with dyspnea and slow gait speed, and these, in turn, lead to several adverse outcomes, including an increased risk of death.8–11 Third, in middle-aged and older persons, a low FEV1 is associated with adverse cardiovascular outcomes.12–15
In clinical practice, threshold values are used to stratify the severity of a spirometric impairment. Regarding FEV1, the most commonly applied thresholds are expressed in 3 ways: in liters, as in the preoperative evaluation of patients undergoing lung resection (ie, 2.00 and 1.50 L); in percent of predicted (% pred), as in the staging of air-flow obstruction by the Global Initiative for Chronic Obstructive Lung Disease (ie, 80% and 50% pred); or in Z scores, also in the staging of air-flow obstruction and previously validated in multiple cohorts of middle-aged and older persons (ie, Z scores of −1.64 and −2.55).5,8,16–20 Whether these thresholds are clinically meaningful when FEV1 is a standalone spirometric predictor has not been established in older persons. In particular, because of age-related changes in lung function, the commonly used thresholds for staging FEV1 may yield different associations with health outcomes.3–5,12,18–20
In primary analyses of older white subjects from the Cardiovascular Health Study (CHS),21 we have therefore evaluated associations between commonly used thresholds for FEV1 and the most definitive health outcome of all-cause mortality. Specifically, we staged FEV1 as a standalone, 3-level measure of severity in L, % pred, and Z scores, and we calculated adjusted odds ratios (ORs) and average attributable fractions (AAFs) for death, respectively. Importantly, the AAF estimates the proportion of deaths attributed to a predictor by combining the prevalence of the predictor with the relative risk of death conferred by that predictor.22,23 In addition, unlike other measures of attributable fraction, the AAF is additive in that the sum of the contribution of each predictor to the outcome does not exceed 100%.22,23
Based on prior work,24 we note that commonly used thresholds for FEV1 may not be equivalently low or high across the adult lifespan and in females versus males. Hence, in secondary analyses of healthy never-smokers from the Global Lung Function Initiative (GLI),4 we have evaluated age and sex differences in the calculation of a commonly used threshold, namely the lower limit of normal (LLN) for FEV1, expressed in L, % pred, and Z scores. Also based on prior work,15 associations with mortality may differ for FEV1 versus FVC. Hence, to further inform comparisons with FEV1, we have evaluated FVC, using the same statistical methods as described earlier.
We posit that the results of this study will further inform the role of FEV1 as a standalone spirometric predictor in geriatric risk stratification.
QUICK LOOK
Current knowledge
The proportion of deaths attributed to the FEV1 when staged by commonly used thresholds (ie, 2.0 L and 1.50 L), percent predicted (ie, 80% and 50%), and Z scores (−1.64 and −2.55) has not been previously reported in older persons. Notably, a Z score threshold of −1.64 defines normal-for-age lung function as the lower limit of normal (5th percentile of distribution) and accounts for differences in age, sex, height, and ethnicity.
What this paper contributes to our knowledge
In a large sample of white persons aged ≥ 65 y, the commonly used thresholds for staging FEV1 (ie, liters, percent predicted, and Z scores) yielded a similar relative risk of death but differed in the prevalence of FEV1 stage and, thus, in the average attributable fraction for death. Hence, the proportion of deaths attributed to a reduced FEV1 is best stratified by Z score staging thresholds because these yield a similar relative risk of death but a more age- and sex-appropriate prevalence of FEV1 stage.
Methods
Study Population
The CHS is a longitudinal study of persons aged ≥ 65 y, identified from a random sample of Medicare eligibility lists in 4 communities in the United States.21 For our analytical sample, we included CHS subjects from the initial 1989–1990 cohort, as only this group completed clinical and spirometric evaluations at the same visit (ie, at study entry). Moreover, consistent with prior work involving older persons,5,18,24,25 we required a spirometric test quality control grade of C or better, which included at least 2 acceptable FEV1 values matching within 200 mL.25 Lastly, because the proportion of African Americans was too small to support our analyses (5.3%), we evaluated only white participants. Therefore, our analytical sample included 4,232 white subjects (81.4% of the initial cohort). The institutional review boards from the Veterans Affairs Connecticut Healthcare System and Yale University approved this study.
Baseline Characteristics
Baseline characteristics included age, gender, body mass index, smoking status, and adjudicated cardiovascular conditions, as follows: hypertension (ie, systolic blood pressure ≥ 160 mm Hg or diastolic blood pressure ≥ 95 mm Hg, or history of hypertension requiring medication), dyslipidemia (ie, low-density lipoprotein cholesterol ≥ 160 mg/dL or high-density lipoprotein cholesterol < 40 mg/dL), diabetes mellitus (ie, taking insulin or oral hypoglycemic, or fasting glucose ≥ 126 mg/dL), cardiovascular disease (ie, myocardial infarction, angina, heart failure, or claudication), and cerebrovascular disease (ie, stroke or transient ischemic attack).21
Spirometry
Spirometry was performed in the seated position, using a water-sealed, Collins Survey II spirometer and contemporary protocols from the American Thoracic Society.21,25 The spirometric performance was reviewed by the CHS Pulmonary Function Reading Center,25 which assigned quality control grades for FEV1.
Based on the highest measured FEV1 in L, we calculated % pred and Z score values for FEV1. % pred was calculated as ([measured FEV1]/[predicted mean for FEV1]) × 100. The predicted mean was established with regression equations from the GLI, which are based on reference populations of healthy never-smokers and include the predictor variables of age, height (measured standing), sex, and ethnicity.2,17 Z scores were calculated using the LMS (λ-μ-Sigma) method, also using GLI regression equations.3,4 Specifically, in addition to the predicted mean (μ), the LMS method included the coefficient of variation (Sigma), representing the spread of reference values (variability in spirometric performance), and skewness (λ), representing the departure from normality.3
Next, using the earlier described thresholds, FEV1 was stratified as stage 1 (FEV1 ≥ 2.00 L, ≥80% pred, and Z score ≥−1.64), stage 2 (FEV1 1.50–1.99 L, 50–79%pred, and Z score −2.55 to −1.63), and stage 3 (FEV1 < 1.50 L, < 50% pred, and Z score < −2.55).5,8,16–20 Regarding Z scores, −1.64 corresponded to the 5th percentile of distribution (defining the LLN), whereas −2.55 corresponded to the 0.5th percentile of distribution.5,8,18–20
To inform comparisons with FEV1 in subjects who achieved FEV1 acceptability criteria, we evaluated FVC in L, % pred, and Z scores. In these analyses, FVC was staged as a standalone, 3-level measure of severity, using the same thresholds as described for FEV1.
Vital Status
Vital status was available on all participants, ascertained over a 10-y follow-up period, with 1,438 confirmed deaths (34% of the analytical sample).
Statistical Analysis
Baseline characteristics of the CHS sample were first summarized as means and standard deviations, or as counts and percentages, and included frequency distributions for FEV1 stage 1–3 in L, % pred, and Z scores. To inform comparisons with FEV1, frequency distributions were also calculated for FVC stage 1–3 in L, % pred, and Z scores.
In primary analyses, using pooled logistic regression models and CHS data, adjusted ORs and 95% CIs for 10-y all-cause mortality were calculated for FEV1 stage 2 and 3, relative to stage 1. Covariates of interest were age ≥ 75 y (a group at high risk of death),27 male sex, body mass index ≥ 30 kg/m2, current smoker, ≥ 10 pack-years, and cardiovascular conditions. Goodness-of-fit was assessed by analysis of residuals. Because missing data were modest (4.2%), complete case analysis was conducted.
Next, using CHS data and the same covariates, adjusted AAFs for 10-y all-cause mortality were calculated for FEV1 stage 2 and 3, relative to stage 1. Notably, the AAF is symmetrical with the probability of the outcome based on all combinations of predictors observed in the data and with final values for individual AAFs obtained by averaging across these observed combinations.22,23 In addition, for the point estimate of each AAF, 5,000 bootstrap samples were generated to establish 95% CIs.
In secondary analyses, using data from GLI, age and sex differences in the LLN for FEV1 when expressed in L, % pred, and Z scores were evaluated in a white individual of average height (white female: average height = 163 cm; white male: average height =178 cm) at ages 25, 45, 65, and 85 y. In these analyses, the LLN (5th percentile of distribution) was calculated from GLI regression equations that are based on reference populations of healthy never-smokers and account for differences in age, height, sex, and ethnicity.2–4
Lastly, to inform comparisons with FEV1, associations of FVC in L, % pred, and Z scores with 10-y all-cause mortality were evaluated, using CHS data and the same statistical methods as described earlier. In addition, using data from GLI, the LLN for FVC in L, % pred, and Z scores was calculated in a white female and male of average height, as described earlier.
SAS/STAT 14.2 software (SAS Institute, Cary, North Carolina) was used for estimating the survival models, and MATLAB software (The MathWorks, Natick Massachusetts) was used to compute the AAFs.
Results
Primary Analyses (CHS Sample)
Table 1 reports baseline characteristics of the CHS sample: mean age was 72.6 y, 43.1% were male, mean body mass index was 26.2 kg/m2, and 54.5% were former or current smokers (average 18.9 pack-years). Cardiovascular conditions were prevalent, including hypertension (41.3%), dyslipidemia (36.7%), diabetes (14.7%), cardiovascular disease (19.3%), and cerebrovascular disease (5.3%).
Baseline Characteristics of Cardiovascular Health Study Sample*
Table 1 also reports baseline FEV1: mean values were 2.09 L, 86.5% pred, and Z score of −0.77 (denoting 22nd percentile, well above the LLN [5th percentile]). Regarding FEV1 stage 1–3, frequency distributions varied when expressed in L, % pred, and Z scores. For FEV1 stage 1, the Z score threshold identified the largest group (79.1% vs 53.9% and 67.0% for L and % pred, respectively). For FEV1 stage 2, the L and % pred thresholds identified the largest groups (28.6% and 26.6% for L and % pred, respectively, vs 12.8% for Z scores). For FEV1 stage 3, the L threshold identified the largest group (17.5% vs 6.4% and 8.2% for % pred and Z scores, respectively). Compared with FEV1, Table 1 also shows that FVC had greater representation in stage 1 but lower representation in stages 2 and 3, whether in L, % pred, or Z scores. For example, based on Z scores ≥ −1.64 (stage 1), 89.0% of participants had normal-for-age FVC (≥ LLN) versus only 79.1% having normal-for-age FEV1 (≥ LLN). Conversely, based on Z scores < −1.64 (combined stages 2 and 3), only 11.0% had abnormal-for-age FVC (< LLN) versus 21.0% having abnormal-for-age FEV1 (< LLN).
Figure 1 graphs adjusted survival over 10 y by FEV1 stage. Although variable separation of survival curves is shown in the first 5 y of follow-up, the adjusted 10-y survival was similar across L, % pred, and Z scores, ranging from 0.70–0.71 for FEV1 stage 1, 0.60–0.62 for FEV1 stage 2, and 0.46–0.51 for FEV1 stage 3, respectively. Compared with FEV1, and whether in L, % pred, or Z scores, Figure 2 shows that the adjusted 10-y survival was similar for FVC stage 1 (0.68–0.69) but lower and more varied for stages 2 and 3 (0.45–0.54 and 0.34–0.45, respectively). Notably, survival in FVC stage 3 as % pred decreased abruptly at 3 y into follow-up, but this included a baseline sample of only 124 subjects.

Adjusted survival curves over 10 y of follow-up, stratified by FEV1 stage in (A) liters, (B) % predicted, and (C) Z scores, using data from the Cardiovascular Health Study sample. Based on estimates from 3 separate pooled logistic regression models (FEV1 in liters, % predicted, and Z score, respectively), adjusted for age ≥75 y, male sex, body mass index ≥ 30, current smoker, ≥ 10 pack-years, and cardiovascular conditions.
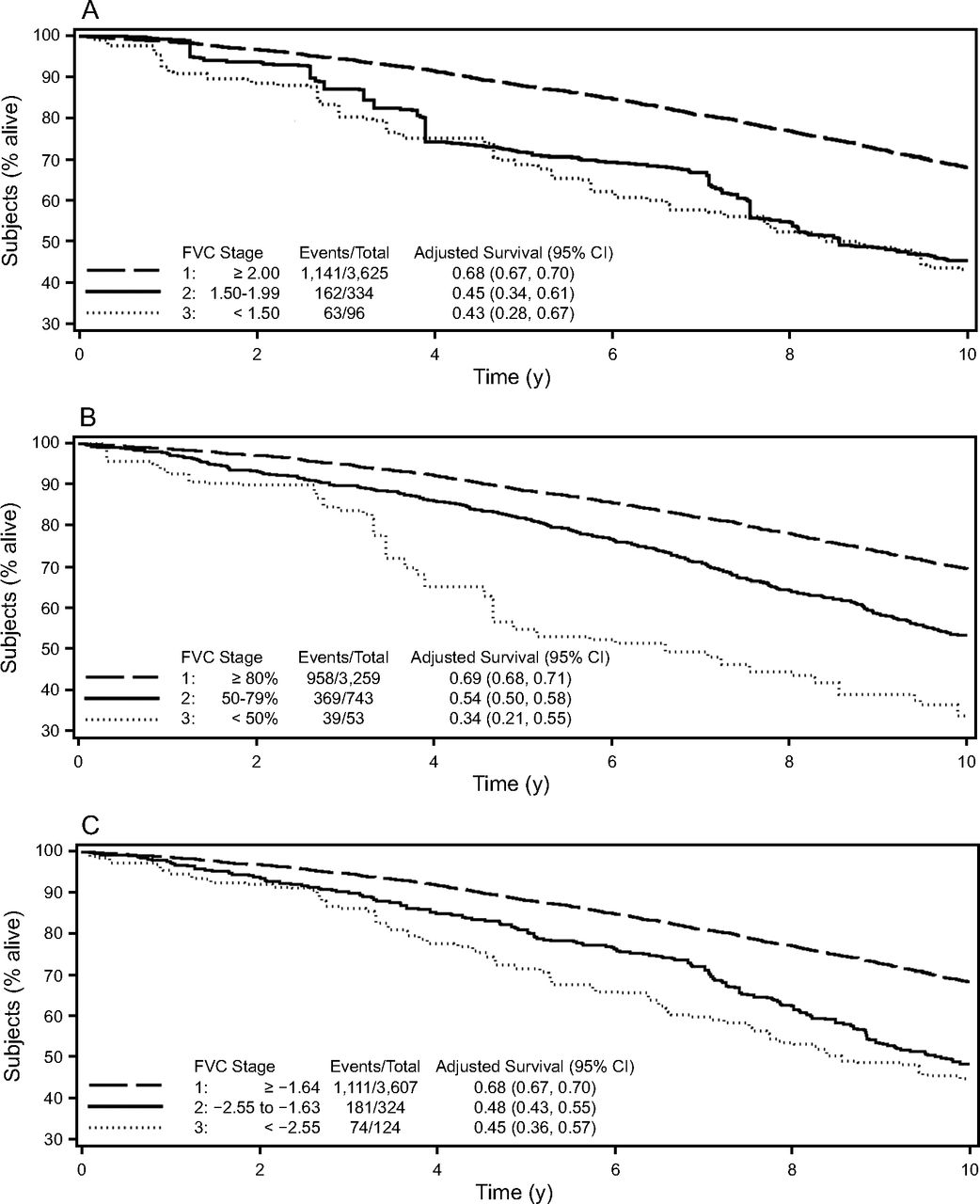
Adjusted survival curves over 10 y of follow-up, stratified by FVC stage in (A) liters, (B) % predicted, and (C) Z scores, using data from the Cardiovascular Health Study sample. Based on estimates from 3 separate pooled logistic regression models (FVC in liters, % predicted, and Z score, respectively), adjusted for age ≥75 y, male sex, body mass index ≥ 30, current smoker, ≥ 10 pack-years, and cardiovascular conditions.
Table 2 reports adjusted ORs and AAFs for 10-y all-cause mortality of FEV1 stages 2 and 3, relative to stage 1. Our results indicate that FEV1 in L, % pred, and Z scores yielded similar increases in the adjusted OR of death, ranging from 1.40–1.51 for stage 2 to 2.35–2.66 for stage 3. Otherwise, FEV1 in L, % pred, and Z scores varied in the adjusted AAF of death, ranging from 3.2–6.4% for stage 2 (46–92 attributable deaths) to 4.5–9.1% for stage 3 (65–131 attributable deaths). Compared with FEV1, Table 2 also shows that FVC in L, % pred, and Z scores yielded higher adjusted ORs of death, ranging from 1.71–1.92 for stage 2 to 2.55–3.37 for stage 3. However, FVC stage 3 as % pred, despite having the highest adjusted OR of death (3.37), yielded the lowest adjusted AAF for death (1.2%) and the lowest number of attributable deaths (n = 17), a consequence of the very low prevalence of 1.3% for FVC stage 3 as % pred (see Table 1); similar results were shown for FVC stage 3 in L and Z scores. Additionally, for combined stages 2 and 3 defined by Z scores < −1.64 (< LLN), only 80 deaths were attributed to abnormal-for-age FVC, whereas 118 deaths were attributed to abnormal-for-age FEV1; similar results were shown for combined stages 2 and 3 when in L and Z scores.
Adjusted Odds Ratio and Average Attributable Fraction for 10-Y All-Cause Mortality*
Secondary Analyses (GLI Sample)
Table 3 reports age and sex differences in the LLN for FEV1 in a GLI sample of healthy never-smokers. Specifically, in a white female and a white male of average height, FEV1 at the LLN decreased across the adult lifespan when in L and % pred, but not Z scores, and was lower in females versus males only when in L. Similar to FEV1, Table 3 also shows that FVC at the LLN decreased across the adult lifespan when in L and % pred, but not in Z scores, and was lower in females versus males only when in L.
Age and Sex Differences in the LLN Spirometric Values* in Subjects of Average Height†
Discussion
In older white subjects from CHS,21 our results indicate that FEV1, staged by commonly used thresholds in L, % pred, and Z scores, yielded similar adjusted ORs of death (Table 2). Thus, commonly used thresholds for staging FEV1 similarly stratified the relative risk of death, because these thresholds similarly compared lung function across three levels of severity.
In contrast, adjusted AAFs for 10-y all-cause mortality varied when FEV1 was staged by commonly used thresholds in L, % pred, and Z scores. For example, the adjusted AAF for death was 6.4% for FEV1 stage 2 as % pred, but only 4.6% and 3.2% for FEV1 stage 2 in L and Z scores, respectively (Table 2). As discussed earlier, the AAF estimates the proportion of deaths attributed to a predictor (FEV1 stage 2) by combining the prevalence of the predictor with the relative risk of death (adjusted OR) conferred by that predictor.22,23 Given that adjusted ORs of death were similar (Table 2), the variability in the adjusted AAF for death was therefore due to differences in the prevalence of the FEV1 stage 2 predictor when expressed in L, % pred, and Z scores (Table 1). A similar pattern of AAF variability was seen with FEV1 stage 3 when expressed in L, % pred, and Z scores (Table 2).
In healthy never-smokers from GLI,4 our results indicate that commonly used FEV1 thresholds are only age- and sex-appropriate when expressed as Z scores, but not when expressed in L or % pred. This is shown in Table 3 by calculating the LLN for FEV1 in L, % pred, and Z scores. Specifically, in white individuals of average height, FEV1 at the LLN decreased across the adult lifespan, including in older persons (≥ 65 y) and when expressed in L and % pred, and it was lower in females versus males but only when expressed in L. We further note that the 80% pred threshold for FEV1, which distinguishes stage 1 from stage 2, is often proposed as an estimate of the LLN, but this is only appropriate in young adults, as shown in our study and in prior work.3,4 Otherwise, across the adult lifespan and in females and males, the Z score value at the LLN remains the same because it is a fixed percentile distribution that accounts for age- and sex-related changes in lung function.
Accounting for age-related changes is a crucial step in interpreting lung function. In particular, the FEV1 declines across the adult lifespan, principally due to increased stiffness of the chest wall and decreased elastic recoil of the lung.3–5 Advancing age also leads to variability in spirometric performance, increasing the coefficient of variation (ie, the spread of reference values).3,4 Likewise, sex, height, and ethnicity must be considered because these predict the FEV1.3,4 Notably, the LMS approach for GLI calculation of spirometric Z scores accounts for age-related changes in lung function and variability in spirometric performance, as well as the predictors of sex, height, and ethnicity.3,4 In contrast, the % pred approach does not account for age-related changes in spirometric performance, and the L approach does not account for age-related changes in lung function or spirometric performance, nor for the predictors of sex, height, and ethnicity.
Accordingly, a major limitation of using FEV1 thresholds in L and % pred is most evident when distinguishing normal-for-age lung function (≥ LLN) from respiratory disease (< LLN).2 To illustrate, we compared a measured (observed) FEV1 in L and % pred with the LLN value expressed in L and % pred. As shown in Table 3, wherein all reported values correspond to the LLN, we find that a white male of average height with a measured FEV1 of 2.0 L would be above the LLN value of 1.86 L at age 85 y (thus having normal-for-age FEV1), but below the LLN values of 2.52, 3.22, and 3.74 L at ages 65, 45, and 25 y, respectively (thus potentially having respiratory disease). Similarly, a white male of average height with a measured FEV1 of 70% pred will be above the LLN value of 67.9% pred at age 85 y (thus having normal-for-age FEV1), but below the LLN values of 73.9, 78.8, and 80.6% pred at ages 65, 45, and 25 y, respectively (thus potentially having respiratory disease). Similar results occur in a white female of average height.
A related limitation of using FEV1 thresholds in L and % pred is the staging of severity. This is because FEV1 in L and % pred assumes incorrectly that a threshold value is equivalently low or high across the adult lifespan and in females or males. For example, by age and sex alone, an 85-y-old female with a measured FEV1 of 1.40 L is classified as having FEV1 stage 3 when expressed in L, despite having FEV1 > LLN (Table 3). Similarly, by age alone, an 85-y-old female or male with FEV1 of 70% pred is classified as having FEV1 stage 2 when expressed as % pred, despite having FEV1 > LLN (Table 3). This misclassification leads to a miscalculation of the prevalence of FEV1 stage and, in turn, to a miscalculation of the AAF. Consequently, the proportion of deaths attributed to a reduced FEV1 is best stratified by Z score staging thresholds because these yield a similar relative risk of death but a more age- and sex-appropriate prevalence of FEV1 stage.
Prior work has suggested that associations with mortality are stronger for FVC than for FEV1.15 Hence, to inform comparisons with FEV1, we evaluated FVC, using the same statistical methods for mortality and LLN as described earlier. Our results suggest that FEV1 compares favorably with FVC for 2 major reasons. First, based on the LLN, FEV1 identified a larger at-risk population than FVC. For example, for combined stage 2 and stage 3 defined by Z scores < −1.64 (< LLN), 21.0% had abnormal-for-age FEV1 but only 11.0% had abnormal-for-age FVC. Second, the number of attributable deaths was substantially higher for FEV1 than for FVC. In particular, for combined stage 2 and stage 3 defined by Z scores < −1.64 (< LLN), 118 deaths were attributed to abnormal-for-age FEV1, whereas only 80 deaths were attributed to abnormal-for-age FVC. Another comparison that merits emphasis is the capacity to complete a given test.6 As discussed earlier, prior work in older subjects has shown that values for FEV1 are more likely to meet quality control testing criteria, as compared with FVC.6
Our study has several strengths. We evaluated FEV1 as a predictor of death, using adjusted ORs and AAFs and data from a well-established cohort of older persons (ie, CHS). In addition, we staged the severity of FEV1 based on thresholds that are commonly used in the preoperative assessment of lung resection and when stratifying lung function in COPD.5,8,16–20
Our study also has several limitations. First, our CHS sample included only white subjects aged ≥ 65 y. Second, we did not evaluate less commonly used spirometric approaches, such as FEV1 indexed to the residual standard deviation, to height (squared or cubed), or to the sex-specific lowest first percentile (ie, the FEV1 quotient), nor did we evaluate the forced expiratory volume in 6 s (FEV6) as a proxy for FVC.28,29 These alternative approaches have merit but are not commonly used in clinical practice, have not applied the LMS method, or lack regression equations for predictive values in those aged > 80 y.5,8,16–20,29 Third, we did not apply an alternative, 5-level Z score staging for FEV1, although we do note that the latter stratification did not have a corresponding threshold specifically set at the LLN (ie, Z score of −1.64).30 As discussed earlier, the LLN is a standard criterion for establishing normal-for-age lung function and, therefore, is a crucial threshold for staging FEV1.2
Our focus on FEV1 as a standalone measure may be also considered as a limitation, given that a combined evaluation of FEV1 and FVC is required to distinguish normal-for-age spirometry from a spirometric impairment.2 This, however, may be a minor limitation. In our study, for example, of the 3,206 subjects with a normal-for-age FEV1 (≥ LLN), we found that 2,933 (91.5%) had normal-for-age spirometry (FEV1/FVC ≥ LLN and FVC ≥ LLN), whereas only 229 (7.1%) had mild air-flow obstruction (FEV1/FVC < LLN but FEV1 ≥ LLN) and only 44 (1.4%) had restrictive pattern (FEV1/FVC ≥ LLN but FVC < LLN).5,18–20,26 Prior work has shown that mild air-flow obstruction represents an early stage of disease and that the FVC criterion for restrictive-pattern (< LLN) may represent a suboptimal effort in the setting of a normal-for-age FEV1.6,18 Nonetheless, in the setting of respiratory symptoms (eg, dyspnea) and risk factors (eg, smoking history), further pulmonary evaluation may be required, given that normal-for-age spirometry or FEV1 cannot definitively exclude respiratory disease.5
Finally, clinical practice often uses thresholds to stratify physiologic impairments (eg, FEV1, left ventricular ejection fraction, and creatinine clearance). However, lung function and many clinical phenomena occur in a continuum, precluding definitive cut points.31–33 Despite this limitation, staging spirometric severity has high value in clinical decision making and public health policy, given that patient care is improved by prioritizing severe over milder physiologic impairments, particularly in older persons with multimorbidity and polypharmacy.35,36 Regarding the staging of spirometric severity according to Z score thresholds, the latter have a strong mathematical, physiological, and clinical rationale, previously evaluated in multiple cohorts of middle-aged and older persons3–5,8,12,18–20,23,26,34,35 and now, in this study, evaluated as a standalone FEV1 predictor.
Conclusions
In a large sample of older white subjects and in a reference population of healthy never-smokers, we have shown that Z score staging thresholds best stratify the proportion of deaths attributable to a reduced FEV1 because these yielded a similar relative risk of death but a more age- and sex-appropriate prevalence of FEV1 stage. Moreover, based on frequency distributions and the number of attributable deaths, our results suggest that FEV1 compares favorably with FVC as a standalone spirometric predictor of death. Hence, FEV1 as a standalone spirometric predictor has a strong rationale in geriatric risk stratification, potentially having broad applicability in patient care and public health policy, given that measuring FEV1 is also more likely to meet quality control testing criteria in older persons.6
Footnotes
- Correspondence: Carlos A Vaz Fragoso MD, 950 Campbell Ave, West Haven, CT 06516. E-mail: carlos.fragoso{at}yale.edu.
The authors were partially supported by a grant from the Claude D Pepper Older Americans Independence Center at Yale University School of Medicine (#P30AG021342 NIH/NIA). The authors have disclosed no other conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}