

Abstract
BACKGROUND: Extubation failure may have several causes, including swallowing dysfunction, aspiration, and excessive upper airway secretions. We hypothesized that a bedside global swallowing pattern assessment including 9 criteria (volume of pharyngeal secretions, 5 swallowing motor items, swallowing reflex, and 2 gag reflexes) performed prior to extubation could identify patients at risk of extubation failure.
METHODS: In a multicenter prospective observational study, all consecutive patients intubated and mechanically ventilated for ≥6 d were included. Before a planned extubation, a physiotherapist evaluated the 9 criteria of the swallowing assessment. The final extubation decision was left to the physician's discretion, blinded to the swallowing assessment. Extubation failure was defined as the need for re-intubation related to aspiration or excessive upper airway secretions within the first 72 h after extubation. Results are expressed as median (interquartile range [IQR]).
RESULTS: The study included 159 subjects (age 61 y [IQR 48–75]; male/female ratio 1.5; Simplified Acute Physiologic score II 54 [IQR 42–66]; duration of mechanical ventilation 11 d [IQR 8–17]). A total of 23 subjects (14.5%) required re-intubation, with 16 occurring within the first 72 h after extubation and 7 related to aspiration or excessive secretions. Swallowing assessment was significantly lower in subjects with re-intubation related to aspiration or excessive secretions within the first 72 h after extubation versus those not re-intubated for aspiration or excessive secretions (6 [IQR 5–7] vs 8 [IQR 7–8], P = .008, respectively). Among the 9 swallowing assessment criteria, normal right pharyngeal gag reflex was associated with a lower incidence of re-intubation related to aspiration or excessive secretions (odds ratio 0.12, 95% CI 0.03–0.59, P = .01), as well as normal left pharyngeal gag reflex (odds ratio 0.13, 95% CI 0.03–0.63, P = .01), with a negative predictive value of 0.98 for each reflex.
CONCLUSIONS: In subjects with prolonged ventilation, the presence of one or both gag reflexes could predict a reduction in extubation failure related to aspiration or excessive upper airway secretions. (Clinical trials.gov registration NCT00780078.)
Introduction
Extubation failure, usually defined as the need for re-intubation 24–72 h after a planned extubation, leads to worse prognosis, prolonged hospitalization, and increased mortality.1 Extubation failure occurs in 2–25% of patients. It may have several causes, including cardiac dysfunction, respiratory failure, encephalopathy, upper airway obstruction, swallowing dysfunction, inadequate cough, and excessive respiratory secretions, and it can eventually lead to aspiration and an excess of upper airway secretions actually defined as witnessed aspiration or inability to maintain airway patency because of pulmonary secretions.1–3 These excessive upper airway secretions could be responsible for up to 16% of extubation failures.2
Swallowing dysfunction depends on several mechanisms, such as pharyngo-lingual muscle atrophy and impaired sensitivity, which lead to inconsistent gag reflexes, independent of potential underlying neurological disorders.4,5 Endotracheal intubation for > 48 h impairs the swallowing reflex, which may also contribute to aspiration pneumonia after extubation.6 The usual extubation criteria are poor predictors of extubation failure due to aspiration or excessive upper airway secretions.5 A score that evaluates the patient's ability to protect the lower airway against secretions may improve the prediction of extubation failure related to aspiration or excessive upper airway secretions. In a previous single-center pilot study enrolling subjects ventilated for > 6 d, we observed a significant correlation between a bedside global swallowing pattern assessment performed before extubation and extubation failure related to aspiration or excessive upper airway secretions.7
We hypothesized that a global swallowing pattern assessment evaluating 9 criteria (ie, volume of pharyngeal secretions, 5 swallowing motor items, swallowing reflex, and 2 gag reflexes) performed before extubation could identify subjects at risk of extubation failure related to aspiration or excessive upper airway secretions.
QUICK LOOK
Current knowledge
Usual weaning criteria are poor risk predictors of extubation failure related to aspiration or excess upper airway secretions. Previous studies have evaluated the potential impact of gag reflex impairment in predicting extubation failure with controversial results. No multi-center studies have evaluated the global swallowing pattern assessment including gag reflex performed before extubation to identify patients at risk of extubation failure.
What this paper contributes to our knowledge
This prospective multicenter study evaluated a bedside global swallowing pattern assessment including the gag reflex performed before extubation as a potential factor associated with re-intubation related to aspiration or excessive upper airway secretions. In a medico-surgical population ventilated for > 6 d, risk of extubation failure related to aspiration or excessive upper airway secretions within the first 72 h after a planned extubation was significantly reduced in the presence of at least one gag reflex.
Methods
Design and Setting
In this multi-center observational study, all consecutive patients intubated for > 6 d were prospectively screened during a 2-year period in 8 ICUs from 4 French university hospitals (Lariboisière, Paris; Bichat-Claude Bernard, Paris; Antoine Béclère, Clamart; North Hospital, Grenoble). Each participating ICU enrolled 20 subjects.
Ethics
This study was approved by our institutional review board and ethics committee (CEERB GHU Nord, no. IRB 00006477) and registered at ClinicalTrials.gov prior to subject enrollment. Informed consent was obtained from all subjects participating in the study.
Primary Objective
Our primary objective was to assess whether a global swallowing pattern assessment evaluating 9 criteria before extubation could correctly predict extubation failure, defined as the need for re-intubation related to aspiration or excessive upper airway secretions within 72 h after extubation.
Subject Selection
Inclusion criteria were: age ≥18 y; oro- or naso-tracheal intubation lasting for > 6 d; patients meeting usual weaning criteria (hemodynamic stability without vasopressors, PaO2/FIO2 ≥ 180 mm Hg, PEEP ≤ 5 cm H2O, Glasgow Coma Scale score ≥ 8/15, Ramsay score ≤ 3, with a completed successful spontaneous breathing trial or successful pressure support test with pressure support ≤ 12 cm H2O).5 Exclusion criteria were patients hospitalized for ear, nose, or throat surgery; known previous swallowing disorders; or chronic persistent vegetative state.
Study Protocol
Subjects were included as soon as extubation was considered by the responsible attending physician (see Supplementary Figure S1 at http://www.rcjournal.com). A respiratory therapist (physiotherapist) who was not directly involved in subject's care nor the extubation decision performed a global swallowing pattern assessment after inclusion and ≤ 24 h before extubation. Physicians were unaware of the result of this evaluation. Physiotherapists systematically assessed the 9 criteria defining the global swallowing pattern assessment (Table 1). The swallowing assessment ranged from 0 to 9 points, scored as 1 point if the subject correctly performed the test or 0 if subject was partially or completely unable to perform the test). The full description of all tests performed by physiotherapists has been previously described.7 Briefly, the cervico-oro-labio-lingual motor controls include the ability to spontaneously hold the head, open the mouth, purse the lips, clench the teeth, and stick the tongue over the inferior teeth. The swallowing reflex was considered to be complete if the larynx rose and moved visibly forward and ausculation for the pharyngeal compression phase was heard. For left and right gag reflex evaluation, a 10-mL syringe was placed between the subject's teeth to prevent biting, and the physiotherapist introduced a finger in the mouth at the side of the reflex assessment to trigger the corresponding gag reflex. Gag reflex scoring was herein binary, being defined as either present or absent (instead of absent, weak, or normal as used in a previous preliminary study).7 A normal gag reflex is defined as a contraction of the pharynx in response to stimulus of the pharyngeal posterior wall or the pharyngeal pillars.8 Additionally, the volume of pharyngeal secretions was measured using the total amount of oro-pharyngeal secretions suctioned during 1 h before the planned extubation. Suctioning and extubation processes were performed according to guidelines.9,10 Extubation failure was defined as the need for re-intubation within 72 h. The main reasons for re-intubation were classified by the responsible attending physician as heart failure (ie, diastolic or systolic dysfunction), aspiration or excessive upper airway secretions (ie, witnessed aspiration or inability to maintain airway patency because of pulmonary secretions),2 respiratory failure (ie, hypoxemic excluding aspiration or excessive upper airway secretions), upper-airway obstruction (ie, the presence of an upper airway stridor),11 or encephalopathy.
Analysis of the 9 Criteria Defining the Global Swallowing Pattern
Data Collection
General subject characteristics collected after admission in the ICU were age, sex, weight, Simplified Acute Physiologic II (SAPS II) score, Acute Physiologic and Chronic Health Evaluation II (APACHE II) on admission, and previous medical history. The main subject parameters collected on the day of extubation were Glasgow Coma Scale score, breathing frequency, heart rate, SpO2, arterial pressure, duration of mechanical ventilation, associated critical illness polyneuropathy, and cough ability. Critical illness polyneuropathy was diagnosed by using the Medical Research Council muscle strength scale; a score ≤ 48 defined the presence of a critical illness polyneuropathy. Cough ability was considered normal if subjects were able to trigger a cough reflex or were able to mobilize their secretions. Paramedical staff also assessed retained secretions via lung auscultation and the forced expiratory test. This evaluation was considered positive (eg, showing evidence of bronchial congestion) if airway secretions were mobilized during this forced expiration test. The volume of endotracheal suctioning during the previous 24 h before extubation was also collected.
After extubation, signs of dyspnea, clinical signs of upper airway secretion retention, a need for chest physiotherapy, use of noninvasive ventilation, pneumonia occurrence, cardiac arrest, and death were documented. Pneumonia was diagnosed with the modified clinical pulmonary infection score and microbiology results.12,13
Statistical Analysis
Continuous data are expressed as mean ± SD with normal distribution and median (interquartile range [IQR]) with non-Gaussian distribution. Qualitative data are expressed as n (%). Chi-square test was used to compare binary variables. Univariate analysis was performed for the global swallowing pattern assessment to compare subjects re-intubated because of aspiration or excessive upper airway secretions within the 72 h after extubation versus those without aspiration or excessive upper airway secretions-related extubation failure with a significant threshold of 5%. Univariate logistic regression was performed to analyze the relationship between the 9 swallowing assessment criteria and the need for re-intubation. Odds ratios (OR) and 95% CIs are presented. All tests involved the use of SAS 9.2 (SAS Institute, Cary, North Carolina).
Results
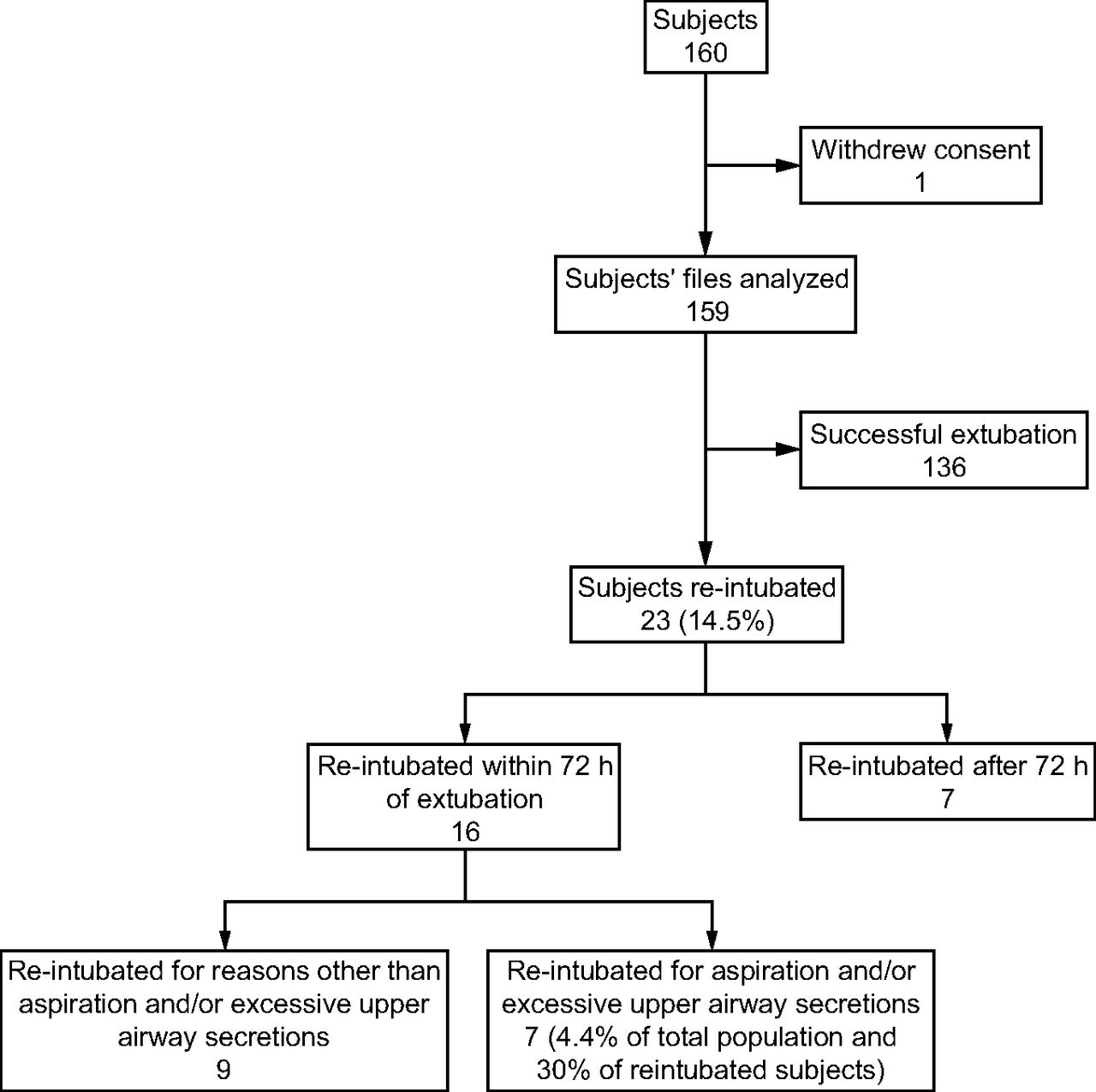
After excluding 1 subject because of secondary consent withdrawal, 159 subjects were included and analyzed (Fig. 1). Baseline subject characteristics on ICU admission are described in Table 2 (treatments received during mechanical ventilation and weaning are detailed in the Supplementary Table S1 at http://www.rcjournal.com). The main subject parameters collected on the day of extubation are shown in Table 3.
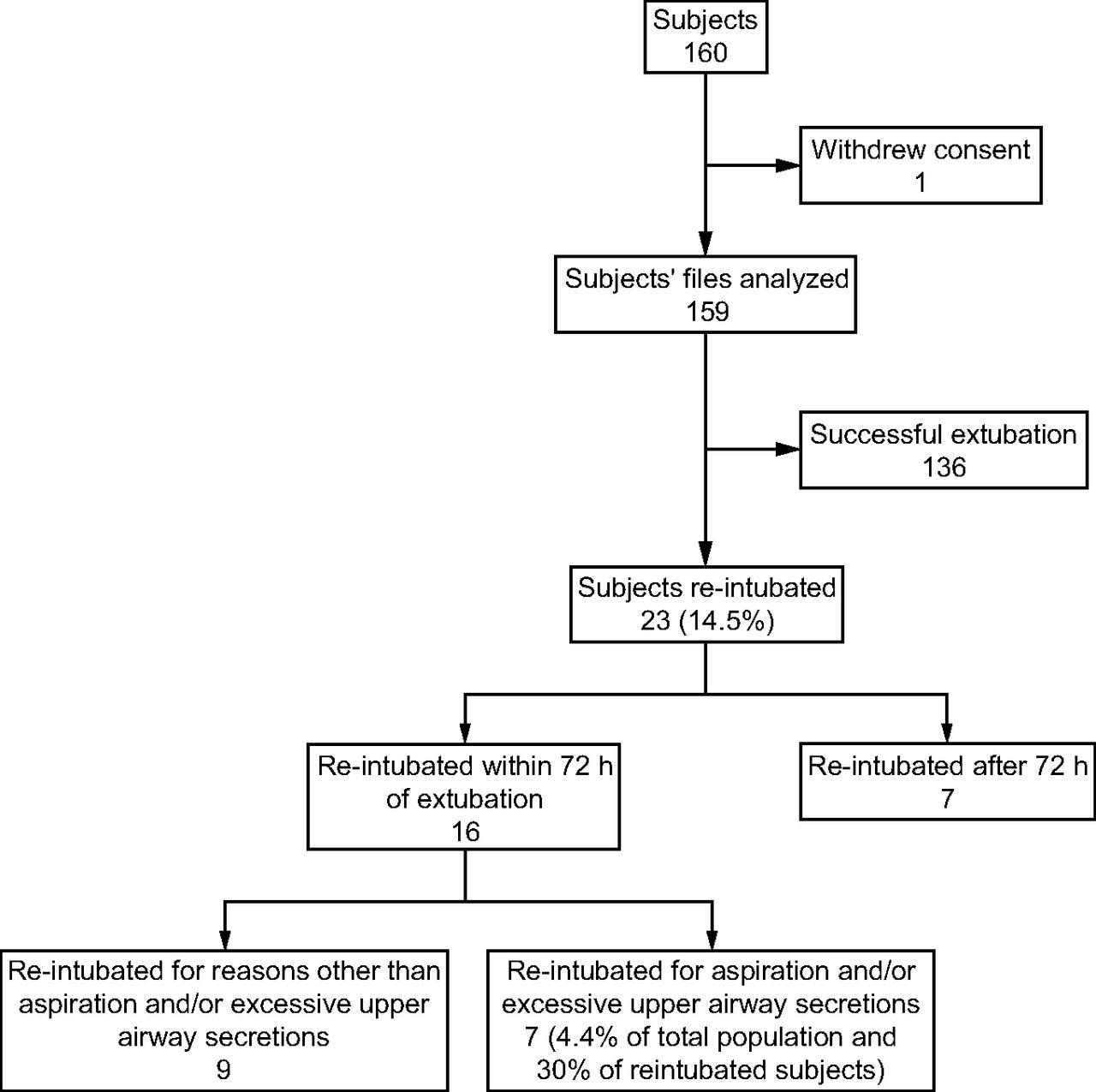
Flow chart. Re-intubation within 72 h of extubation was considered as early extubation failure.
General Subject Characteristics After Admission to the ICU
Subject Characteristics on the Day of Extubation
Respiratory Function and Outcome After Extubation
No unplanned extubations occurred, and 136 subjects were successfully extubated. After extubation, 133 subjects received daily chest physiotherapy, and 39 received noninvasive ventilation. Hospital-acquired pneumonia occurred in 10 subjects after extubation. A total of 23 subjects (14.5%) required re-intubation (Fig. 1). The delay between extubation failure and re-intubation was 26 h (IQR 15–84). The main and associated causes of re-intubation among all 23 re-intubated subjects were acute heart failure (n = 3), respiratory failure not related to aspiration or excessive upper airway secretions (n = 16), upper airway obstruction (n = 4), and severe encephalopathy (n = 4); multiple causes of re-intubation were described in 4 subjects. Among the 23 re-intubated subjects, 16 were re-intubated during the first 72 h, with 7 subjects experiencing aspiration or excessive upper airway secretions. Six subjects (4%) died within the first week after extubation.
Global Swallowing Pattern Assessment Before Extubation
The global swallowing pattern assessment was significantly lower in subjects re-intubated within the first 72 h after extubation because of aspiration or excessive upper airway secretions versus those not re-intubated for aspiration or excessive upper airway secretions (6 [IQR 5–7]) vs 8 [7–8], P = .008). Among the 9 criteria evaluating swallowing pattern, only right and left gag reflexes were associated with re-intubation related to aspiration or excessive upper airway secretions within the first 72 h after extubation (P = .01 and .02, respectively; Table 1). Logistic regression analysis indicated that the risk of extubation failure related to aspiration or excessive upper airway secretion was reduced with a normal right or left gag reflex (OR 0.12, 95% CI, 0.03–0.59, P = .01; and OR 0.13, 0.03–0.63, P = .01, respectively), with a negative predictive value of 0.98 regardless of the location of the pharyngeal gag reflex (ie, right or left).
Discussion
To our knowledge, our study is the first prospective multi-center trial evaluating global swallowing pattern before extubation, using 9 criteria including the gag reflex as a potential factor associated with re-intubation related to aspiration or excessive upper airway secretions. In this medico-surgical population ventilated for > 6 d, the presence of at least one gag reflex before a planned extubation was associated with the absence of extubation failure related to aspiration or excessive upper airway secretions occurring within the first 72 h after extubation.
Previous studies evaluated the potential impact of gag reflex impairment in predicting extubation failure with controversial results. On the one hand, Davies et al14 showed that 37% of healthy subjects had an absent gag reflex, but Coplin et al15 showed that 32 of 36 brain-injured subjects with absent or weak gag could be successfully extubated. Similarly, in 150 stroke subjects, Guru et al16 did not found any association between the presence of gag reflex and successful extubation. On the other hand, gag reflex evaluation (in addition to other criteria including cough, swallowing evaluation, and neurologic examination) has been found to correctly predict extubation failure. In 285 neurocritically ill subjects intubated for > 6 h, Anderson et al17 observed an association between an intact gag reflex and the absence of extubation failure. In 140 brain-injured subjects intubated for > 48 h, Godet et al18 reported an association between the absence of gag reflexes and extubation failure, with 67% of extubation failure being related to hypersecretion. This literature is concordant with our results in intubated subjects. The impact of an intact gag reflex in protecting the upper airway has also been described in non-intubated stroke subjects.19 The gag reflex, or evaluation of pharyngeal sensitivity and glossopharyngeal nerve functionality, is one of the upper-airway protection reflexes, in addition to cough and swallow.
Finally, the previous studies evaluating gag reflex specifically considered the global extubation failure rate, whereas our study focused on extubation failure related to aspiration or excessive upper airway secretions. Interestingly, our study indicates that gag reflex is an important determinant of extubation failure related to aspiration or excessive upper airway secretions in a medico-surgical population intubated for ≥ 6 d.
Our study has some limitations. The number of extubation failures related to aspiration or excessive secretions within the first 72 h was rather low (4.4%). This rate did not allow us to perform multivariate analyses or scores of prediction of early aspiration and excessive secretions–related extubation failure according to statistical issues.20 In our study, there may have been differences in baseline characteristics between subjects re-intubated because of aspiration or excess upper airway secretions versus those who were not re-intubated. However, we did not perform further statistical tests in order to limit statistics only to the tested hypothesis. These potential differences between subgroups could identify a specific population particularly at risk of extubation failure related to aspiration and excess secretions that needs further evaluation. It could be argued that the studied population was highly selected. However, a re-intubation rate of 14.5% in our subjects was similar to commonly reported rates of 10–20%.1 Conversely, the rate of extubation failure related to aspiration or excessive upper airway secretions in our study seemed higher than the rate initially described by Epstein et al2 (ie, 30% vs 16%). Finally, subjects enrolled in our study were mixed medico-surgical ICU subjects, whereas previous studies have only included brain-injured subjects.14–17 Despite specific inclusion criteria, our results highlight the potential role of gag reflexes in extubation failure evaluation in subjects ventilated for prolonged duration.
Conclusions
Subjects with prolonged intubation experiencing early extubation failure related to aspiration or excessive upper airway secretions had lower scores on a global swallowing pattern assessment, including a gag reflex evaluation, prior to extubation. The gag reflex systematic assessment before extubation could be added to the usual criteria for extubation to prevent extubation failure related to aspiration or excessive upper airway secretions in specific mechanically ventilated patient populations. Use of the gag reflex as a potential predictor of extubation failure secondary to aspiration or excessive secretions requires further investigation.
Acknowledgments
We acknowledge the following additional contributors: Frederic Baud, Dan Benhamou, François Brivet, Claude Jacquot, Philippe Montravers, Didier Payen de la Garanderie, Bernard Régnier, Jean-François Timsit, Philippe Colonel, Nathalie Debarle, Annie Gouverneur, Sandra Crispin, Valérie Mazur, Céline Araujo, Camille Beauvair, Françoise Bizouard, Annie Boudol, Astrid Cammarata, Martine Costille, Guillaume Cottereau, Anne Marie Cousse, Cyril De Vaumas, Yohann Dubois, Sylvie Dumesnil, Oïkana Gaztelurrutia, Romain Habrias, Fanny Hamon, Nicolas Deye, Marie-Hélène Houzé, Claude Jacquot, Anthony Lanceleur, Pierre Lavagne, Walid Makhlouf, Joaquim Matéo, Bruno Mégarbane, Laura Navaro, Luminita Neculaita, Pedro Pereira-Pasos, Sylvia Perez, Dominique Prat, Judith Remy, Ana Maria Ruiz, Hélène Rousseau, Clément Trincat, Eric Vicaut, Julie Weyrech, Alain P. Yelnik. The complete list of investigators and collaborators participating in the EVAKIN study is provided in the supplementary materials available at http://www.rcjournal.com.
Footnotes
- Correspondence: Nicolas Deye MD PhD, Medical Intensive Care Unit, GHU Saint Louis-Lariboisière-Fernand Widal, AP-HP, Inserm UMRS-942, 2 Rue Ambroise Paré, 75010 Paris, France. E-mail: nicolas.deye{at}aphp.fr.
This work was supported by a research grant from the Assistance Publique - Hôpitaux de Paris (Recherche en Soins Courants SCR 06013). The authors have disclosed no conflicts of interest.
A version of this paper was presented at the French congresses of Intensive Care and of Physical and Rehabilitation Medicine (Paris and Reims, January and October 2013).
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}