

Abstract
BACKGROUND: In the modern era, many devices exist to support patients with respiratory insufficiency. There is currently no way to depict changes in the degree of support a patient is receiving over time.
METHODS: We enrolled 4,889 subjects undergoing 5,732 cardiac surgical visits between 2011 and 2017 and extracted data elements related to respiratory support from the electronic medical record. We created an algorithm to use these data to categorize a subject's respiratory support type and to calculate an empirically derived respiratory support score (RSS) at each postoperative minute; the RSS is scored on a scale of 0 to 100. The RSS was then used to identify the timing and incidence of nonprocedural re-intubations, which were electronically verified against secondary verification fields (eg, nursing extubation note). Rates of nonprocedural re-intubations and noninvasive ventilation were compared between surgical mortality risk scores (STAT scores).
RESULTS: Computerized assignment of RSS was performed for 3 million subject time points. Mechanical ventilation duration varied significantly by STAT score (P < .001). Nonprocedural re-intubations increased nonsignificantly with increasing STAT score (P = .059, overall 4.3%); time to nonprocedural re-intubation did not (P = .53). Noninvasive ventilation use was more common and was prolonged with increasing STAT score (P < .001).
CONCLUSIONS: Elements of respiratory support can be automatically extracted and transformed into a numerical RSS for visualization of respiratory course. The RSS provides a clear visual depiction of respiratory care over time, particularly in subjects with a complex ICU course. The score also allows for the automated adjudication of meaningful end points, including timing of extubation and incidence of nonprocedural re-intubation.
Introduction
Patients with critical illness and respiratory insufficiency require a spectrum of respiratory support to ensure sufficient gas exchange. This varies from supplemental oxygen administered via nasal cannula, noninvasive ventilatory assistance (eg, biphasic positive airway pressure), invasive ventilation, high-frequency oscillatory ventilation, high-frequency jet ventilation, or extracorporeal membrane oxygenation. Nested within these increasingly intense forms of support exist a spectrum of settings that are titrated to meet changing patient conditions. Although many patients require more than one setting and modality of support during their hospital course, there is currently no way to summarize a patient's progress over time using a single numerical score. Changes in the support provided to a patient are typically parameter-specific (eg, the PEEP was weaned from 8 cm H2O to 6 cm H2O). However, this approach limits the ability to describe changes in multiple variables over time or to visualize a patient's trajectory during a hospitalization.
Scores that describe a patient's response to illness are well established in critical care medicine and may be useful as end points in clinical trials and for benchmarking. For example, the Sequential Organ Failure Assessment (SOFA) score categorizes a patient's end organ function in response to an insult such as sepsis.1 Other scores, such as the oxygenation index, combine the degree of support provided to a patient with their response2 and represent a useful metric to follow a patient's trajectory over time. However, it is becoming increasingly recognized that data density in the ICU places a heavy cognitive load on providers,3 and that the use of dashboards and summary scores are useful tools to provide context for complex patients. We propose a numerical respiratory support score (RSS) that describes respiratory support over time. This score is intended to display variations in a patient's ventilator settings and support modes over time. This score incorporates all variables related to the respiratory support that a patient receives at a single point in time, independent of their response to it.
QUICK LOOK
Current knowledge
Subjects with critical illness and respiratory insufficiency may be supported using a spectrum of respiratory support devices and modes to ensure sufficient gas exchange. However, no numerical score that crosses devices and modes is available for the depiction of trends in respiratory support over time.
What this paper contributes to our knowledge
We present a respiratory support score ranging from 0 (room air) to 100 (full ECMO) that describes the device, mode and settings used in generally escalating order. The score over time may be used to plot changes in respiratory support over time, including intubations and extubations, changes between ventilatory modes, and ECMO support.
Methods
This study was performed under an approved institutional review board protocol at Boston Children's Hospital (IRB-CR00023338-2). We identified all subjects undergoing cardiac surgery at Boston Children's Hospital between February 2011 and December 2017. We excluded patients who were extubated prior to ICU admission, had a preexisting tracheostomy, were terminally extubated, were transferred to another facility while on a ventilator, or had not achieved hospital discharge at the time of analysis.
Assignment of Respiratory Support Type
We assigned all modes of respiratory support to a respiratory support type (RST), such as nasal cannula, biphasic positive airway pressure, or invasive ventilation (Table 1). All data elements that define respiratory support at our institution (see the supplementary materials at http://www.rcjournal.com) were identified and exported from an institutional electronic data warehouse (BCH360, IBM Netezza). The accuracy of a subset (5%) of each raw data element was confirmed against the clinical electronic medical record interface. These data elements were then processed according to a logic to assign an RST to each minute of hospitalization. Each RST was associated with defining, allowable, and conflicting entries in one or more fields of the electronic medical record (see the supplementary materials at http://www.rcjournal.com). In most cases, the RST was assigned based on one or more defining variables that identified the RST unambiguously. In other cases, however, there were simultaneous conflicting entries (eg, one entry was consistent with room air and another was consistent with mechanical ventilation). To manage these situations, we established a confidence scoring system associated with each score (see the supplementary materials at http://www.rcjournal.com).
Numerical Bounds Assigned to Respiratory Support Types
Assignment of RSS and Association With Length of Stay
To create a continuous numerical score that allowed visualization and analysis of changes in device settings as well as changes in RST over time, we created an empiric RSS that ranged from 0 (room air) to 100 (full-flow extracorporeal membrane oxygenation). Briefly, the settings associated with each RST were assigned an empiric weighting and an age-stratified maximum and minimum setting. At each moment in time, the RSS varied within the bounds assigned for each RST based on device settings (see the supplementary materials at http://www.rcjournal.com). The RSS was plotted over time to provide a visual depiction of a subject's hospital course over time.
We used RSS assignments to determine the agreement between intubated RSS values (RSS > 25) versus nonintubated RSS values (RSS ≤ 25) against a separate reference field for the timing of extubation that was independent of any of the variables included in the RSS. This reference field was adjudicated based on separate extubation fields entered manually by nursing and respiratory therapy (see the supplementary materials at http://www.rcjournal.com).
We examined the associations between the area under the RSS-time plot prior to extubation for all subjects with the postextubation length of stays in the ICU and hospital using a linear regression analysis. We used the Mann-Whitney test to examine differences in the area under the RSS-time plot prior to extubation between subjects who subsequently did or did not fail extubation within 24, 48, and 72 h.
Statistical Analysis
Baseline demographics, body weight, surgical ischemic times, and lengths of stay were compared between subjects of differing surgical complexities (based on STAT score) with the Kruskal-Wallis test. The incidence of nonprocedural re-intubations and the number of extubations to noninvasive ventilation were compared between groups with the chi-square test. The fraction of subjects extubated by postoperative time was compared between STAT scores4,5 with non-linear regression analysis (second order quadratic). All graphs were produced in GraphPad Prism (GraphPad Software, La Jolla, California), and all statistical analyses were performed in R 3.4.1.
Results
Among 4,889 subjects, there were 5,732 cardiac surgical admissions meeting inclusion criteria, representing 5,732 initial intubations and 6,386 extubations. The most common operations fell within the STAT 2 category, which includes patent ductus arteriosus ligations, tetralogy of Fallot repair, bidirectional Glenn operations, and extracardiac Fontan operations. Of the 5,732 admissions, most were children age 1–12 y (39%), followed by 1–12 months (27%), followed by newborns < 1 month of age (14%) (Table 2). As expected, cardiopulmonary bypass ischemic times, the incidence of delayed sternal closure, and ICU and hospital length of stay all increased with increasing STAT score.
Subject Demographics Stratified by STAT Score of the Primary Procedure for Each Subject Admission*
Of the total 6,386 extubations, 6,355 (99.5%) were correctly matched with confirmatory extubation fields within the electronic medical record. A subset (120 extubations, 1.9% of all extubations) were correctly identified by the algorithm but were missed in the extubation fields manually entered by nurses and respiratory therapists. An additional 47 extubations (0.7% of total) were identified using the extubation fields and intentionally omitted by a rule in the algorithm that required 2 consecutive entries of an extubated RST (see the supplementary materials at http://www.rcjournal.com).
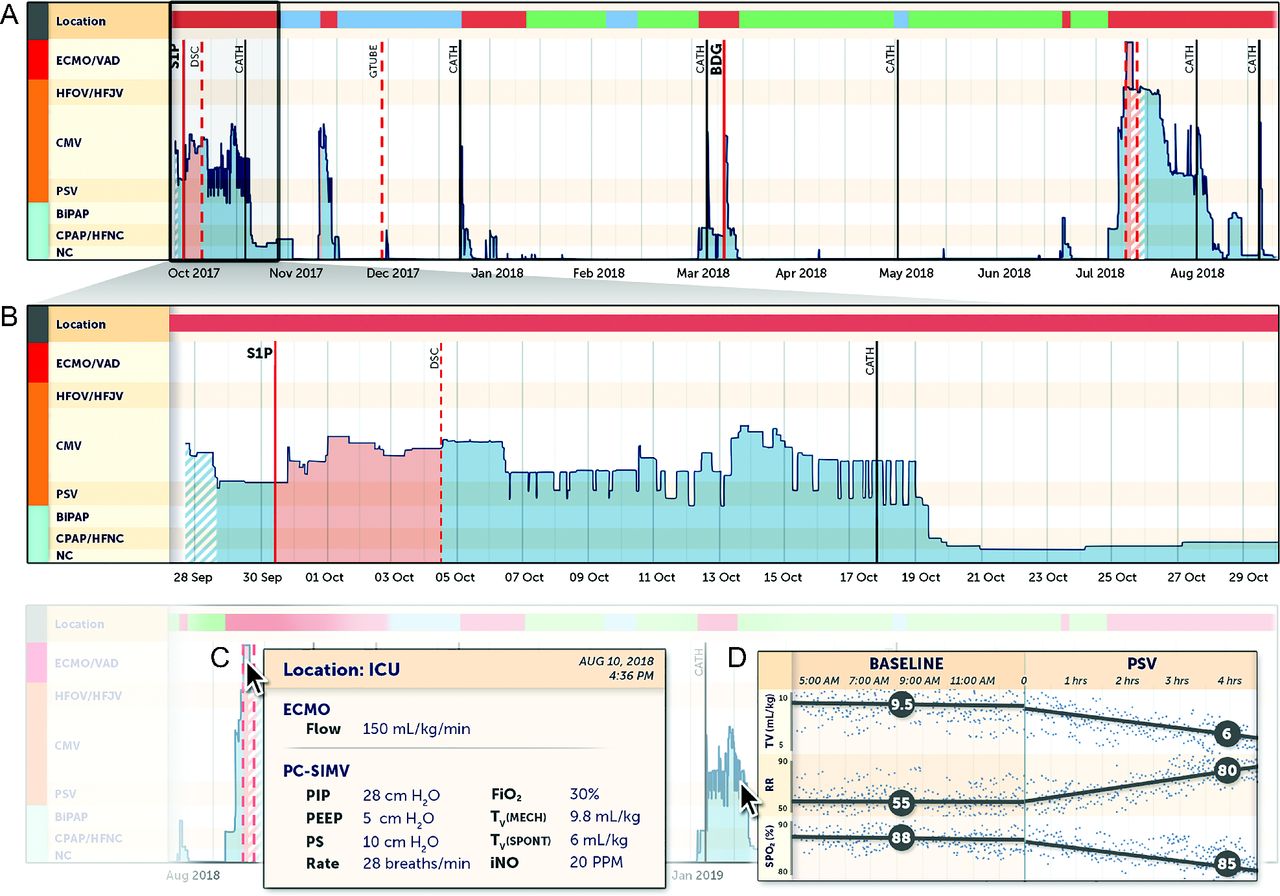
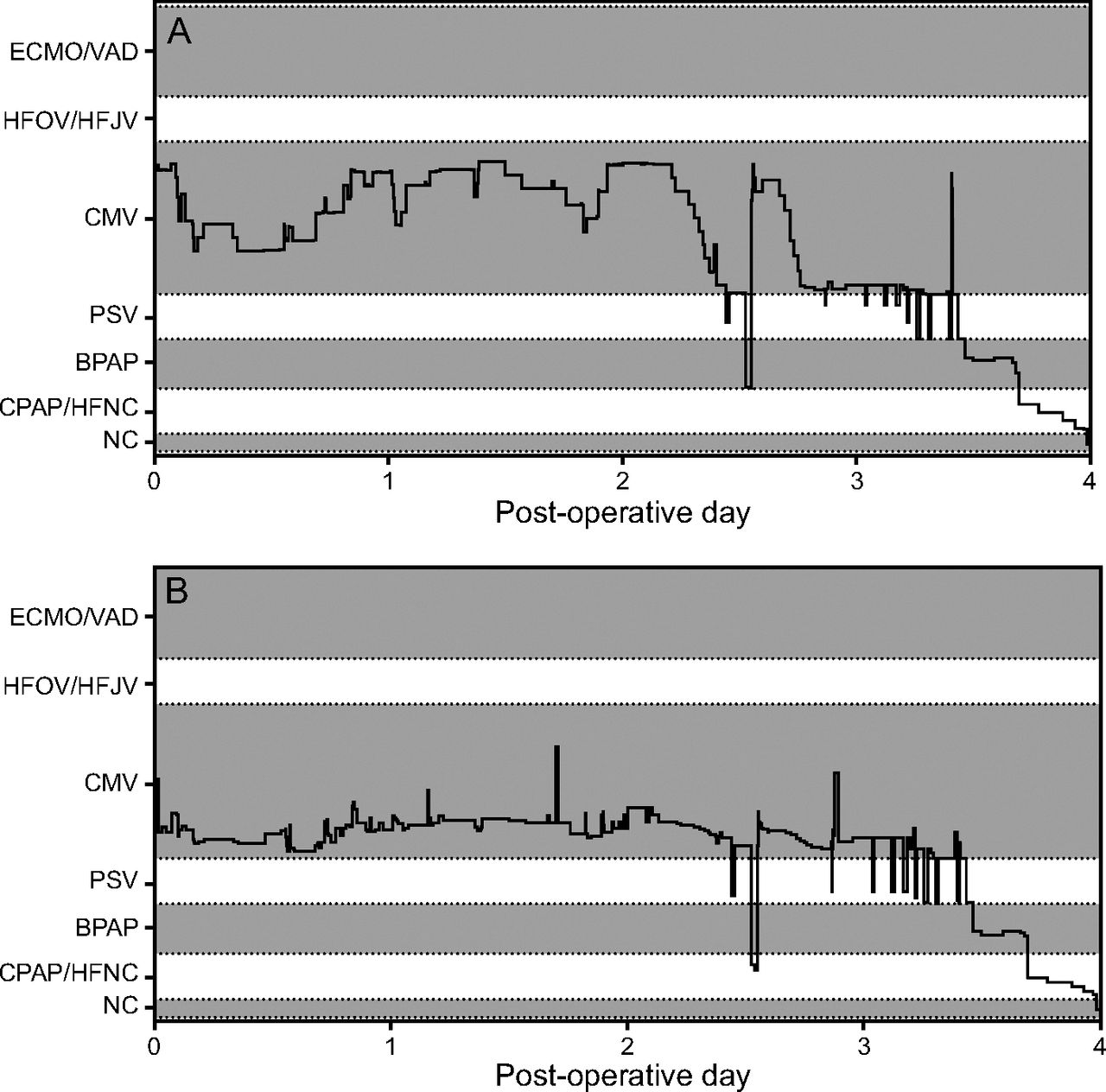
Plotting the RSS over time allows visualization of the fraction of time that a subject has been hospitalized and on each type of ventilatory support, as well as the weaning trajectory within each RST (Fig. 1). Pressure support trials, procedures, neuromuscular blockade use, and inhaled nitric oxide are plotted on the same image. The visual appearance of the score can also be optimized for a given patient population by differential weightings of the variables that are most often manipulated in a patient (Fig. 2).
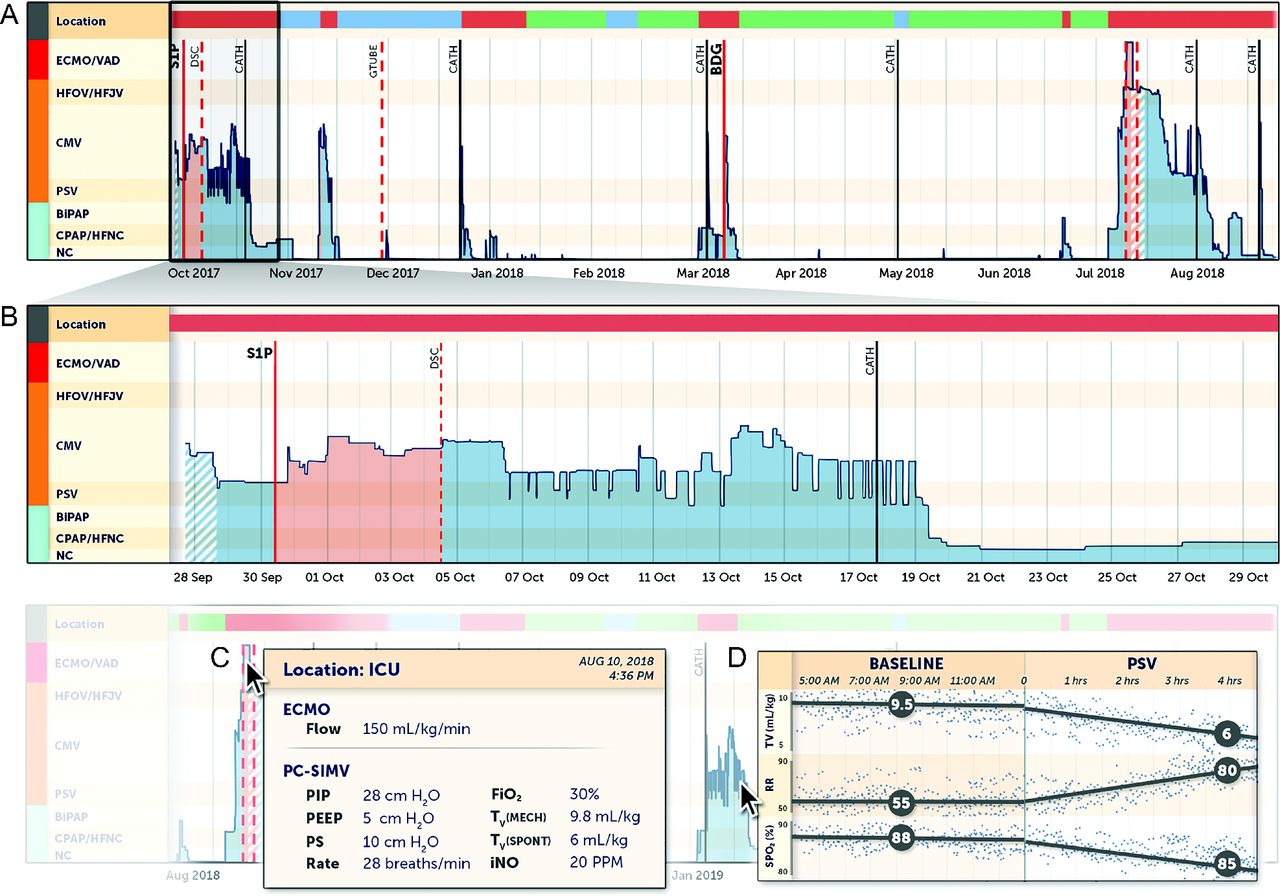
A: Respiratory support scores (RSS) for the first 11 months of life for a subject born with hypoplastic left heart syndrome. Dates and procedures have been modified. As visualized on the inset (B), the subject was mechanically ventilated from admission to the ICU (denoted by the red line to the right of Location) and was on inhaled nitric oxide (see dashed white/blue during the first 18 h of life) until undergoing a stage 1 palliation (S1P). Postoperatively, the subject was on neuromuscular blockade (peach shading) until undergoing delayed sternal closure (DSC), after which he underwent conventional ventilation for 2 weeks with several pressure support ventilation sprints (PSV, see downward divots in RSS). The subject was subsequently extubated to CPAP/HFNC for an additional 10 d prior to weaning to nasal cannula and transfer to the ward; see blue shading to the right of Location in (A). The subject's course can be subsequently followed graphically including location (green = home), mechanism and trajectory of respiratory support, and superimposed procedures. Note that the numerical value of the RSS in this schema is used primarily to visualize the respiratory support type and trajectory thereof. C: Using simple mouse-over gestures, time-relevant details can be displayed. D: Alternatively, relevant end points, such as tidal volume (VT), breathing frequency (rate), and arterial saturation ( ) can be compared prior to and following initiation of a pressure support trial. HFNC = high-flow nasal cannula.
) can be compared prior to and following initiation of a pressure support trial. HFNC = high-flow nasal cannula.
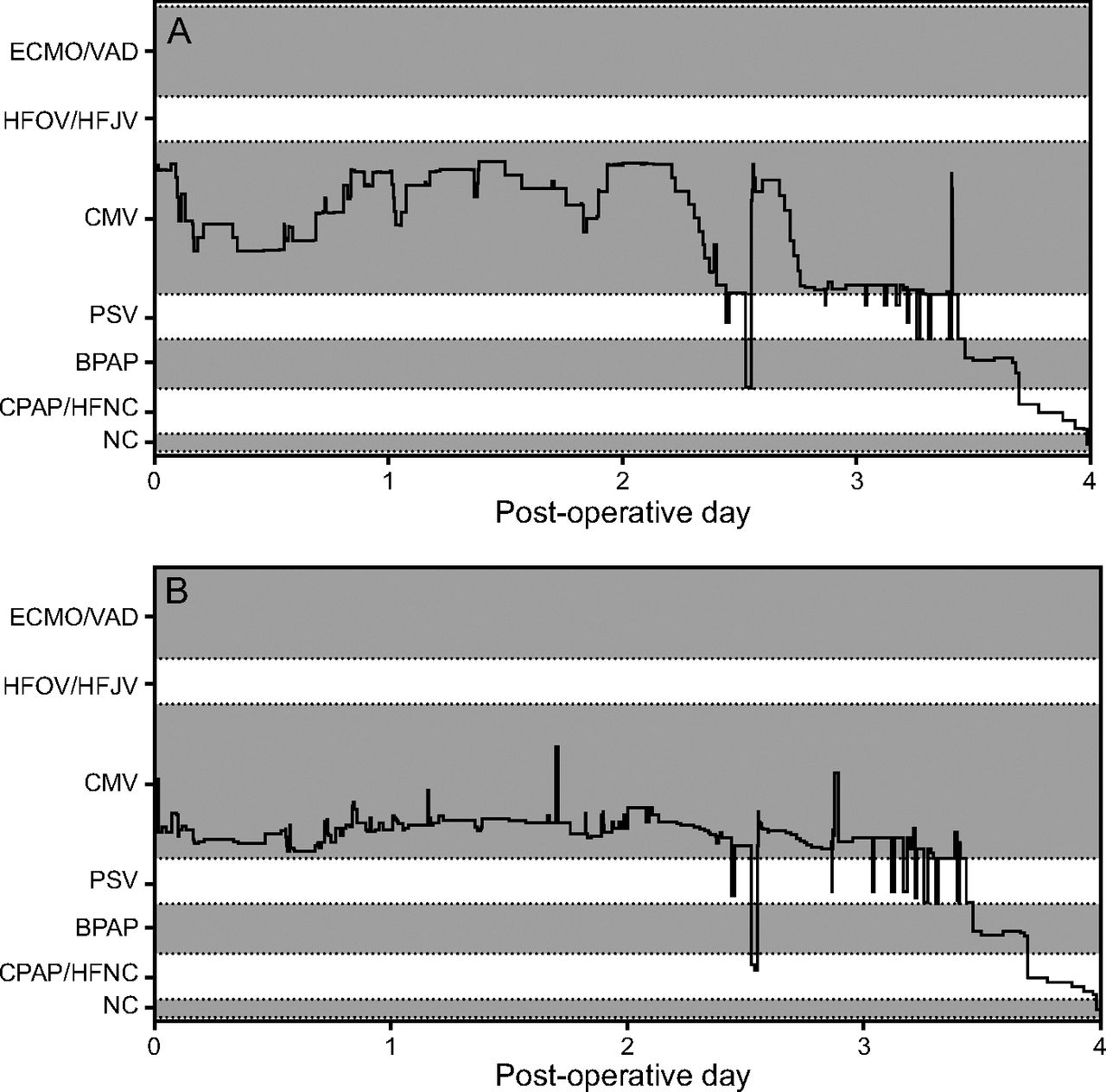
Examples of 2 RSS plots based on different weightings as shown for ventilator rate,  , and PEEP. Because mechanical ventilation is more titrated based upon ventilator rate in this patient population, the plot in which the ventilator rate is more heavily weighted (A) is the most demonstrative of changes in mechanical ventilation. ECMO = extracorporeal membrane oxygenation; VAD = ventricular assist device; HFOV = high-frequency oscillatory ventilation; HFJV = high-frequency jet ventilation; CMV = conventional mechanical ventilation; PSV = pressure support ventilation; BPAP = biphasic intermittent positive airway pressure; HFNC = high-flow nasal cannula; NC = nasal cannula.
, and PEEP. Because mechanical ventilation is more titrated based upon ventilator rate in this patient population, the plot in which the ventilator rate is more heavily weighted (A) is the most demonstrative of changes in mechanical ventilation. ECMO = extracorporeal membrane oxygenation; VAD = ventricular assist device; HFOV = high-frequency oscillatory ventilation; HFJV = high-frequency jet ventilation; CMV = conventional mechanical ventilation; PSV = pressure support ventilation; BPAP = biphasic intermittent positive airway pressure; HFNC = high-flow nasal cannula; NC = nasal cannula.
The duration of mechanical ventilation varied significantly with STAT category; at 24 h, 87% of subjects following a STAT 1 operation were extubated, compared with 8.3% following a STAT 5 operation, for whom the median time to extubation was 5.6 d (Fig. 3).

Cumulative fraction of subjects extubated by postoperative time based on STAT score over the first 17 d (A) and within the first 72 h (B, zoomed in for enhanced resolution for lower STAT scores). P < .001, Kruskal-Wallis test.
Because we excluded all nonintubated ICU admissions, the total number of initial intubations was equivalent to the total number of admissions. The overall number of nonprocedural re-intubations throughout the study period was 4.3% and did not significantly change over the era studied (P = .70, linear regression). The rates of nonprocedural re-intubation trended to increase with increasing STAT score (P = .059) (Fig. 4A; see the supplementary materials at http://www.rcjournal.com). Among subjects undergoing a STAT 5 operation, 7% underwent nonprocedural re-intubation within 72 h of extubation, compared with 1.1% of subjects following STAT 1 operation (P = .74). The timing of nonprocedural re-intubation was similar between subjects with different STAT scores (P = .53) (Fig. 4B). The total number of re-intubations (procedural and nonprocedural) prior to hospital discharge increased significantly with STAT score (P < .001), with 22% of STAT 5 subjects undergoing re-intubation, half of which were procedural.

A: Fraction of subjects undergoing procedural and nonprocedural re-intubation prior to hospital discharge (P = .059, Kruskal-Wallis test). B: Cumulative timing of nonprocedural re-intubation was not different (P > 0.1) between subjects of varying STAT scores. Graph truncated at 10 d postoperative. C: Cumulative fraction of subjects requiring noninvasive ventilation during their hospitalization stratified by STAT score (P < .001).
Extubation to CPAP or biphasic positive airway pressure was significantly more common as STAT score increased, varying between 4.6% in STAT 1 subjects to 27.6% in STAT 5 subjects (P < .001). Among STAT 1 subjects, 2.6% required noninvasive ventilation for at least 72 h compared with 25.7% of STAT 5 subjects (P < .001 per Kruskal-Wallis test) (Fig. 3C).
Association of RSS Scores Over Time With Postextubation Course
The area under the RSS-time curve prior to extubation correlated weakly with postextubation ICU stay (r2 = 0.21) and hospital stay (r2 = 0.23). The area under the curve prior to extubation was significantly different between subjects who subsequently failed extubation at 24, 48, and 72 h (P < .001) (see the supplementary materials at http://www.rcjournal.com). However, these findings were similar to correlations with the total duration of invasive ventilation prior to extubation.
Discussion
We have created a methodology for the automated extraction and presentation of many data elements related to respiratory support within a continuous numerical score. The development of this score was made possible by the presence of an electronic data warehouse, a pipeline that allows end users to access electronic medical record data for a large number of patients. As electronic data warehouses become more prevalent in health care, the extraction, transformation, and use of similarly large and complex datasets will become increasingly possible.
We developed this score with several goals in mind. First and foremost, this tool will allow bedside providers in diverse settings to visualize a patient's complete respiratory history by annotating the RSS curve with relevant events, including surgical procedures or hospital events such as an infection or transplant. Because respiratory support tends to track with illness severity, the RSS is in some ways a broadly useful “illness score” that can be quantified continuously over time. Therefore, it may also be useful as a backdrop against which one might visualize other factors that may either result from (eg, a change in serum creatinine) or cause (eg, degree of valvar regurgitation) critical illness. More immediately, the RSS allows for a visual depiction of a patient's trajectory over time regardless of RST. In this first iteration, we empirically weighted the variables toward those typically weaned in a pediatric cardiac ICU, a population generally absent pulmonary pathology. However, the score can be easily customized for different environments by applying different weightings or even different variables within a similar construct (eg, more heavily weighting peak inspiratory pressure, PEEP, and  in the ARDS setting). The score facilitates visualization of changes in RST, such as pressure support (or spontaneous breathing) trials, including the number and duration of those trials. This may be useful to communicate such information in the ICU environment, in which providers change regularly. As illustrated in Figure 1D, hyperlinks to changes in RST might allow for visualization of contemporaneous changes in vital signs or other relevant patient-level responses.
in the ARDS setting). The score facilitates visualization of changes in RST, such as pressure support (or spontaneous breathing) trials, including the number and duration of those trials. This may be useful to communicate such information in the ICU environment, in which providers change regularly. As illustrated in Figure 1D, hyperlinks to changes in RST might allow for visualization of contemporaneous changes in vital signs or other relevant patient-level responses.
Similar to other composite scores that have been developed for early warning of subject deterioration,6,7 with further score optimization, the RSS may permit early identification of changes in patient respiratory status (when manifest with increasing respiratory support). The addition of vital signs or measured variables (rather than settings) may improve the power of the RSS to predict extubation readiness.8–10 It may also permit early identification of trends in a patient's degree of respiratory support that may be represented more subtly in individual variables. The RSS may also identify when a patient's ventilator weaning trajectory has stalled, which may prompt clinical reevaluation.
The second purpose of the RSS was to enable the automated adjudication of meaningful end points, such as the duration of mechanical ventilation, incidence of nonprocedural re-intubation, and the use of noninvasive ventilation. Such end points are commonly used for quality improvement, benchmarking, and central reporting purposes. For some events (eg, extubation), there are discrete fields in which care providers are able to record the event within the electronic medical record. Even when present, though, these fields lacked the time resolution that a more comprehensive approach yields. Creating logic around all available respiratory data allowed us to refine the timing of extubation in 68% of subjects and allowed us to identify the timing of extubation accurately in 1.9% of subjects in whom extubation was not otherwise recorded discretely. This improvement in accuracy resulted from the use of all available data elements related to respiratory support to make a judgment regarding a subject's intubation status. For instance, at times one member of the care team neglected to record an extubation within the extubation field, but others recorded that the subject was on a nasal cannula, and that extubation was only captured accurately using the algorithm. Although the creation of the double-entry rule precluded the algorithm from identifying the fraction of subjects with nearly immediate re-intubations, the use of the RSS combined with a verification field allowed nearly perfect identification of the presence and timing of extubations and re-intubations in automated fashion. As the streaming and capture of continuous data becomes more prevalent, the mapping of data directly from devices to electronic medical record systems will ensure consistency in data entry protocols, remove typographical errors, and increase the detail of data recorded. As this occurs, the utility of such data for quality improvement, benchmarking, and reporting purposes will significantly increase. The importance of scores that amalgamate such data into useful matrices is therefore paramount.
However, the use of data in this way requires several caveats. Ensuring data accuracy (ie, that we are reporting what we intend to report) requires systematic and rigorous validation of data. We found that the most common and impactful error was a systematic misunderstanding of what data are entered into particular fields and what is meant by it. Field names in the electronic medical record are often nonintuitive, confusing, and even misleading. Rules preventing erroneous entry are incomplete. Navigating such errors requires knowledge of clinical workflows, including how data were entered (by whom and at what times), to anticipate common human error patterns (eg, recording room air for  of 0.21 in ventilated subjects within a field intended to connote that an extubated subject is breathing spontaneously). The use of a confidence score was an electronic manifestation of such judgments and will likely be an important component for others who choose similar approaches. The validation process also requires a robust reference standard, which will in most cases be manually adjudicated data. However, once data are mapped and verified in this way, reporting may become substantially more efficient and even more accurate, particularly because connectivity between medical devices and the electronic medical record improves and data recording is increasingly consistent. Similarly, the granularity of detail in central repositories may increase when this approach is used, allowing for the exploration of new variables and hypotheses.
of 0.21 in ventilated subjects within a field intended to connote that an extubated subject is breathing spontaneously). The use of a confidence score was an electronic manifestation of such judgments and will likely be an important component for others who choose similar approaches. The validation process also requires a robust reference standard, which will in most cases be manually adjudicated data. However, once data are mapped and verified in this way, reporting may become substantially more efficient and even more accurate, particularly because connectivity between medical devices and the electronic medical record improves and data recording is increasingly consistent. Similarly, the granularity of detail in central repositories may increase when this approach is used, allowing for the exploration of new variables and hypotheses.
The third, and admittedly secondary, purpose of our work was to describe the demographics of mechanical and noninvasive ventilation in a large cohort of subjects at a single center, and to describe associations of each with a surgical complexity score (ie, STAT). A recent registry reported that the extubation failure rate across 15 pediatric cardiac ICUs was 1.1–9.8%, and the only factor significantly associated with re-intubation was duration of mechanical ventilation prior to attempted extubation.11 Similarly, we found that the incidence of nonprocedural re-intubation at 24, 48, and 72 h was significantly associated with both time on mechanical ventilation and the area under the RSS-time curve. Additionally, the incidence of noninvasive ventilation use in this report is lower than that reported in a recent multicenter study of comparable subjects, although we did not include high-flow nasal cannula as a type of noninvasive ventilation.12 It is likely that the broad use of tools such as RSS may allow centers to compare bedside behaviors that may contribute to this phenomenon, such as the recurrent use of pressure support trials to determine readiness for extubation.
Limitations
Our work represents a first iteration of an empiric respiratory support score. Our primary intention was to summarize multiple respiratory data into a single score, allowing classification into RST and visualization of trajectory. In doing so, we focused primarily on data accuracy and not on score optimization. In the future, the score may be optimized for different care environments to enhance not only the visualization of common changes in ventilation but also its predictive power. Although we identified a poor correlation between the area under the RSS-time curve prior to extubation with subsequent length of stay, it is possible that a statistical optimization of the score (including the parameters included and their limits and weights) toward this end could improve this correlation; particularly in patients with primary respiratory disease, it seems likely that a rigorously weighted score quantifying the most predictive ventilator parameters could be predictive of such meaningful outcomes.
Conclusions
Elements of respiratory support can be automatically extracted and transformed into a single numerical RSS for visualization of respiratory course. The RSS also allows for the automated adjudication of multiple meaningful end points, including timing of extubation and incidence of nonprocedural re-intubation. In the future, RSS may be optimized for visualization in different patient groups and for prediction of events that may be related to the degree of respiratory support over time.
Acknowledgments
The authors thank Kiran Guntipalli, Julie Ferullo, and Tracy Chen for assistance with the data extraction process. Figure 1 was provided courtesy of Kai Ou Tang MA. Boston Children's Hospital has filed a provisional patent application covering the RSS as a data visualization tool.
Footnotes
- Correspondence: John N Kheir MD, 300 Longwood Ave, Boston, Massachusetts 02115. E-mail: john.kheir{at}childrens.harvard.edu
This work was supported by the Gerber Foundation, the Hess Family Cardiac Innovation Fund, and the Heart Center Strategic Investment Fund. The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}