

Abstract
BACKGROUND: Detection of diaphragmatic muscle activity during invasive ventilation may provide valuable information about patient-ventilator interactions. Transesophageal electromyography of the diaphragm ( ) is used in neurally adjusted ventilatory assist. This technique is invasive and can only be applied with one specific ventilator. Surface electromyography of the diaphragm (
) is used in neurally adjusted ventilatory assist. This technique is invasive and can only be applied with one specific ventilator. Surface electromyography of the diaphragm ( ) is noninvasive and can potentially be applied with all types of ventilators. The primary objective of our study was to compare the ability of diaphragm activity detection between
) is noninvasive and can potentially be applied with all types of ventilators. The primary objective of our study was to compare the ability of diaphragm activity detection between  and
and  .
.
METHODS: In this single-center pilot study,  and
and  recordings were obtained simultaneously for 15 min in adult subjects in the ICU who were invasively ventilated. The number of breathing efforts detected by
recordings were obtained simultaneously for 15 min in adult subjects in the ICU who were invasively ventilated. The number of breathing efforts detected by  and
and  were determined. The percentage of detected breathing efforts by
were determined. The percentage of detected breathing efforts by  compared with
compared with  was calculated. Temporal and signal strength relations on optimum recordings of 10 breaths per subject were also compared. The Spearman correlation coefficient was used to determine the correlation between
was calculated. Temporal and signal strength relations on optimum recordings of 10 breaths per subject were also compared. The Spearman correlation coefficient was used to determine the correlation between  and
and  . Agreement was calculated by using Bland-Altman statistics.
. Agreement was calculated by using Bland-Altman statistics.
RESULTS: Fifteen subjects were included. The  detected 3,675 breathing efforts, of which 3,162 (86.0%) were also detected by
detected 3,675 breathing efforts, of which 3,162 (86.0%) were also detected by  . A statistically significant temporal correlation (r = 0.95, P < .001) was found between
. A statistically significant temporal correlation (r = 0.95, P < .001) was found between  and
and  in stable recordings. The mean difference in the time intervals between both techniques was 10.1 ms, with limits of agreement from –410 to 430 ms.
in stable recordings. The mean difference in the time intervals between both techniques was 10.1 ms, with limits of agreement from –410 to 430 ms.
CONCLUSIONS: Analysis of our results showed that  was not reliable for breathing effort detection in subjects who were invasively ventilated compared with
was not reliable for breathing effort detection in subjects who were invasively ventilated compared with  . In stable recordings, however,
. In stable recordings, however,  and
and  had excellent temporal correlation and good agreement. With optimization of signal stability,
had excellent temporal correlation and good agreement. With optimization of signal stability,  may become a useful monitoring tool.
may become a useful monitoring tool.
- mechanical ventilation
- neurally adjusted ventilatory assist (NAVA)
- electromyography of the diaphragm (EAdi)
- surface electromyography
Introduction
Patient-ventilator asynchrony frequently occurs during invasive ventilation and is associated with patient discomfort, a prolonged duration of invasive ventilation, and increased hospital and ICU length of stay.1–4 Although adjustments of the ventilator settings and reducing analgosedation can sometimes resolve patient-ventilator asynchrony, detection in clinical practice is difficult.5–8 Patient-ventilator interactions are not assessed continuously, and waveform interpretation can be complex.9
Information about diaphragm muscle activity during invasive ventilation could improve monitoring of patient-ventilator interactions.10 Currently, the electrical activity of the diaphragm ( ) can be recorded by transesophageal electromyography (
) can be recorded by transesophageal electromyography ( ). This requires insertion of a specialized nasogastric tube (
). This requires insertion of a specialized nasogastric tube ( catheter) with electrodes at the level of the gastroesophageal junction. The
catheter) with electrodes at the level of the gastroesophageal junction. The  is used in neurally-adjusted ventilatory assist mode.11 Because
is used in neurally-adjusted ventilatory assist mode.11 Because  is a reflection of spontaneous breath initiation, Neurally-adjusted ventilatory assist mode improves synchrony between the patient and the ventilator compared with conventional assisted modes.12,13 Despite the great potential of
is a reflection of spontaneous breath initiation, Neurally-adjusted ventilatory assist mode improves synchrony between the patient and the ventilator compared with conventional assisted modes.12,13 Despite the great potential of  , its use in general ICU practice is limited because only one specific type of ventilator supports neurally-adjusted ventilatory assist mode ventilation.
, its use in general ICU practice is limited because only one specific type of ventilator supports neurally-adjusted ventilatory assist mode ventilation.
Surface electromyography of the diaphragm ( ) could overcome this disadvantage. It is easy to apply, noninvasive, and can theoretically be used in combination with all type of ventilators. Over the past decade, surface electromyography of the respiratory muscles has been investigated.14–16 However, this technique has not been compared with
) could overcome this disadvantage. It is easy to apply, noninvasive, and can theoretically be used in combination with all type of ventilators. Over the past decade, surface electromyography of the respiratory muscles has been investigated.14–16 However, this technique has not been compared with  in adult patients who are invasively ventilated. The primary objective of our study was to investigate the ability of breathing effort detection with
in adult patients who are invasively ventilated. The primary objective of our study was to investigate the ability of breathing effort detection with  compared with
compared with  during invasive ventilation. Because this was a pilot study, we were also interested in the best possible performance of
during invasive ventilation. Because this was a pilot study, we were also interested in the best possible performance of  . As a proof of concept, we determined the temporal relation between
. As a proof of concept, we determined the temporal relation between  and
and  on optimal recordings.
on optimal recordings.
Quick Look
Current Knowledge
Patient-ventilator asynchrony is a common problem in invasive ventilation. Information about transesophageal electrical activity of the diaphragm ( ) during invasive ventilation can improve interaction between the patient and the ventilator. Surface electromyography of the diaphragm (
) during invasive ventilation can improve interaction between the patient and the ventilator. Surface electromyography of the diaphragm ( ) is noninvasive and can potentially be applied with all ventilators. Yet, it has not directly been compared with
) is noninvasive and can potentially be applied with all ventilators. Yet, it has not directly been compared with  in the clinical ICU setting.
in the clinical ICU setting.
What This Paper Contributes to Our Knowledge
In stable recordings,  provided accurate information about patient-ventilator interaction. Due to signal disturbances, however,
provided accurate information about patient-ventilator interaction. Due to signal disturbances, however,  is not yet sufficient to perform as a reliable monitoring tool in current ICU practice.
is not yet sufficient to perform as a reliable monitoring tool in current ICU practice.
Methods
Study Design
This prospective observational cohort study was conducted in the ICU of the Amsterdam University Medical Center, location Academic Medical Center, Amsterdam, the Netherlands. The study protocol was approved by the medical ethics committee of the Amsterdam University Medical Center, location Academic Medical Center (NL5006.018.14). Subjects were included after written informed consent was signed by the legal representative. Adult patients who were invasively ventilated were eligible for inclusion if (1) ventilation was expected for at least 48 h, (2) they were ventilated with a Servo-i ventilator (Maquet, Wayne, New Jersey), (3) on a spontaneous mode of ventilation, and (4) an EAdi catheter was inserted. The exclusion criteria were (suspected) neuromuscular disease or cervical spinal cord injury, known phrenic nerve injury, and contraindication for surface electrode placement (eg, severe skin infections at the electrode site). Because of the pilot character of this study, a sample size calculation was not performed.
The ethical committee of the Amsterdam University Medical Center (MEC 10/107 # 10.17.0921) approved this study (registration number NTR4766, 01/09/2014). Detailed written and verbal information about this study was provided to patients' legal representatives. When subjects were mentally recovered after study inclusion, confirmatory consent was asked of the subjects to use the recordings for research purposes. The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Recordings of  and
and


The  and
and  recordings were obtained simultaneously for a period of 15 min. Ventilator settings were not adjusted during the recordings. For
recordings were obtained simultaneously for a period of 15 min. Ventilator settings were not adjusted during the recordings. For  recordings, 4 disposable electrodes (Covidien, Dublin, Ireland) were placed bilaterally below the lower frontal and dorsal ribs. An additional electrode (ie, ground) was placed on the sternum (see the supplementary materials at http://www.rcjournal.com) All the electrodes were connected with shielded cables to a Dipha-16 physiological amplifier (Inbiolab BV, Groningen, Netherlands). The electromyography signals were combined to obtain the electrical activity of the diaphragm (
recordings, 4 disposable electrodes (Covidien, Dublin, Ireland) were placed bilaterally below the lower frontal and dorsal ribs. An additional electrode (ie, ground) was placed on the sternum (see the supplementary materials at http://www.rcjournal.com) All the electrodes were connected with shielded cables to a Dipha-16 physiological amplifier (Inbiolab BV, Groningen, Netherlands). The electromyography signals were combined to obtain the electrical activity of the diaphragm ( ). Data were wirelessly transmitted to a laptop computer placed at the bedside of the patient. The
). Data were wirelessly transmitted to a laptop computer placed at the bedside of the patient. The  recordings, by using the
recordings, by using the  catheter (Maquet, Solna, Sweden), were registered trough wired connection between this laptop computer and the Servo-i ventilator.
catheter (Maquet, Solna, Sweden), were registered trough wired connection between this laptop computer and the Servo-i ventilator.

Automatic peak detection for A: surface electrical activity of the diaphragm [ ] and B: transesophageal electrical activity of the diaphragm [
] and B: transesophageal electrical activity of the diaphragm [ ].
].
Data Collection and Processing
The first 2 min of each measurement were exempted from analysis to limit signal disturbances. In each subject, the analysis was performed on the 10 min of recording directly after the exempted first 2 min. Peak diaphragm muscle activity of each breathing effort was detected automatically by using a minimum peak height threshold and a minimum peak distance threshold (Fig. 1). For both  and
and  , a respiratory peak was detected when the signal strength was at least 80% of the mean signal strength amplitude. Respiratory
, a respiratory peak was detected when the signal strength was at least 80% of the mean signal strength amplitude. Respiratory  peaks had to be within a range of 1,000 ms around the respiratory peak in the
peaks had to be within a range of 1,000 ms around the respiratory peak in the  signal to be detected as a matching breathing effort. When multiple
signal to be detected as a matching breathing effort. When multiple  peaks were detected within this range from de
peaks were detected within this range from de  peak, the closest the sEAdi peak closest to the tEAdi peak was defined as the respiratory
peak, the closest the sEAdi peak closest to the tEAdi peak was defined as the respiratory  respiratory peak. The
respiratory peak. The  signal was processed with an electrocardiogram gating technique as described in previous studies and was further processed with a boxcar averager.17,18 Processing of
signal was processed with an electrocardiogram gating technique as described in previous studies and was further processed with a boxcar averager.17,18 Processing of  was integrated into the Servo-i ventilator.19
was integrated into the Servo-i ventilator.19
Other documented data were age, sex, and body mass index of the patient; reason for ICU admission; Richmond Agitation Sedation Scale at the moment of assessment; number of days on invasive ventilation at the moment of assessment; Acute Physiology and Chronic Health Evaluation II score; and ventilator mode and parameters (including  , breathing frequency, oxygen saturation, PEEP, peak inspiratory pressure, and tidal volume).
, breathing frequency, oxygen saturation, PEEP, peak inspiratory pressure, and tidal volume).
Data Analysis
The number of matching breathing efforts detected by  and
and  was divided by the total number of breathing efforts detected by
was divided by the total number of breathing efforts detected by  . The temporal relation was investigated on selected stable recordings of 10 successive breathing efforts per subject. The stable recordings were visually selected from the recording. First, we determined the duration of peak-to-peak time intervals between successive breathing efforts (the time between peak amplitudes) in both
. The temporal relation was investigated on selected stable recordings of 10 successive breathing efforts per subject. The stable recordings were visually selected from the recording. First, we determined the duration of peak-to-peak time intervals between successive breathing efforts (the time between peak amplitudes) in both  and
and  (9 peak-to-peak intervals per patient). Thereafter, the temporal correlation and agreement between both methods were calculated.
(9 peak-to-peak intervals per patient). Thereafter, the temporal correlation and agreement between both methods were calculated.
Statistics
Non-parametric statistics were used with median (interquartile range [25th–75th percentile]) because of the small population size. The Spearman rank correlation coefficient (r) was calculated to determine the strength of the relation between  and
and  . Bland-Altman plots were used to determine the agreement between
. Bland-Altman plots were used to determine the agreement between  and
and  .20 Values with significance levels of ≤.05 were considered significant. Data analysis was performed with MATLAB R2016a (MathWorks, Natick, Massachusetts). The statistical analyses were performed by using SPSS version 24 (SPSS, Chicago, Illinois).
.20 Values with significance levels of ≤.05 were considered significant. Data analysis was performed with MATLAB R2016a (MathWorks, Natick, Massachusetts). The statistical analyses were performed by using SPSS version 24 (SPSS, Chicago, Illinois).
Results
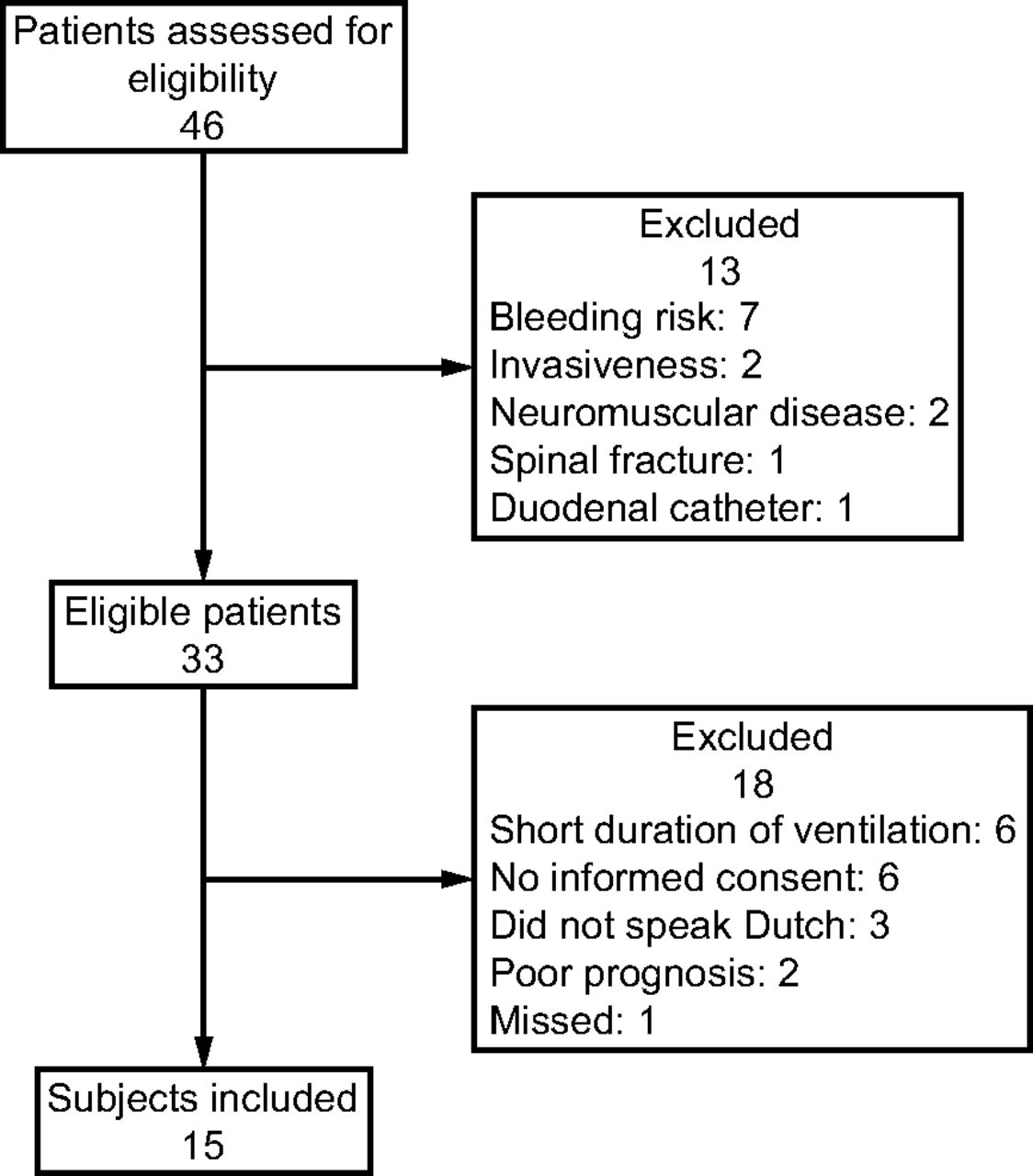
Between December 2014 and April 2015, we screened all patients in the ICU who were ventilated with a Servo-i. Results of the screening and inclusion process are shown in Figure 2. Fifteen subjects were included (see Table 1 for baseline characteristics), all the subjects tolerated the measurements well. Ventilator settings and respiratory parameters during the measurements are shown in Table 2.
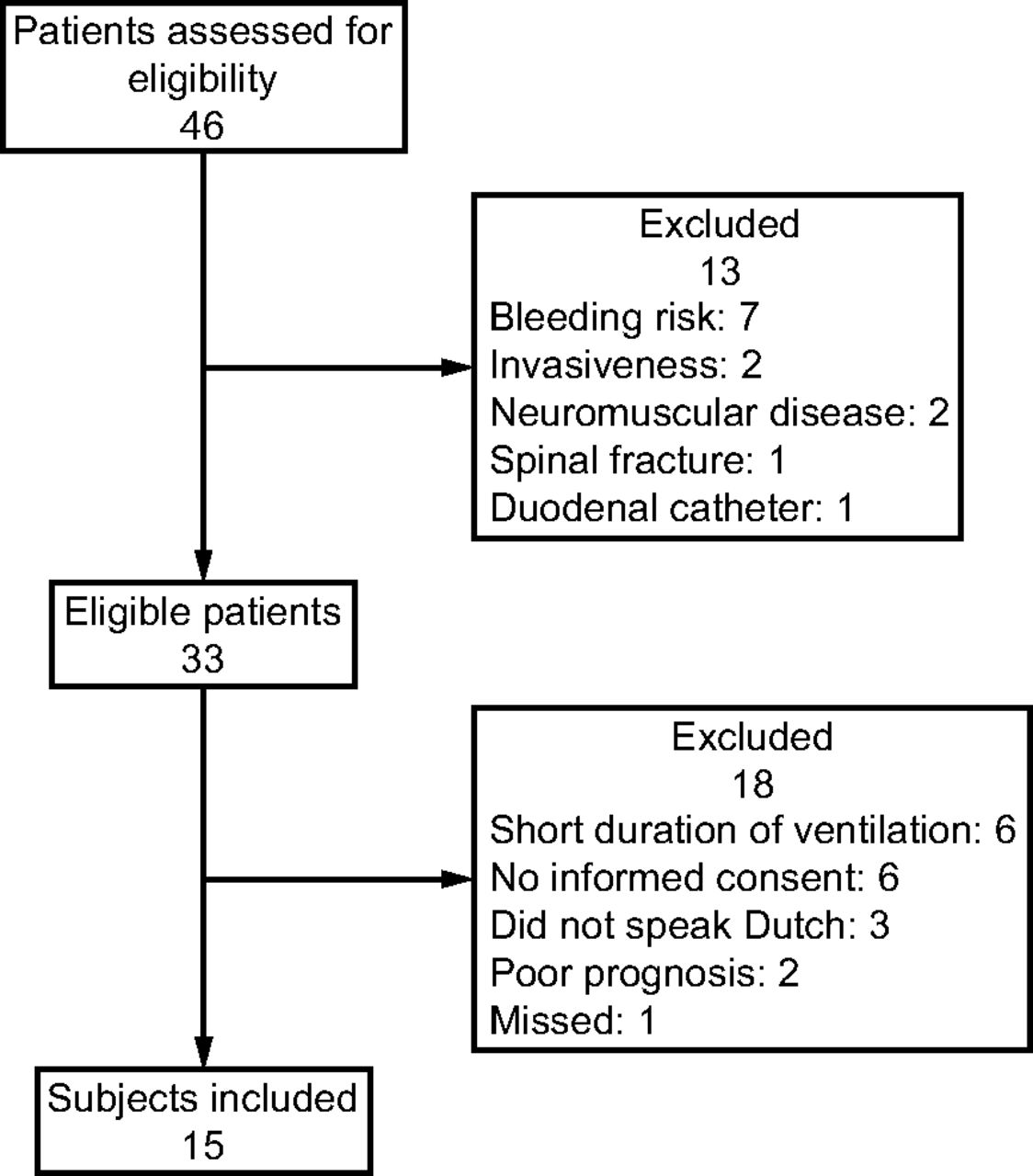
Flow chart.
Baseline Characteristics
Ventilator Settings and Respiratory Parameters
Breathing Effort Detection
A total of 3,675 breathing efforts were accurately obtained by using  , of which 3,162 (86.0%) were matched by
, of which 3,162 (86.0%) were matched by  detection. There was a great variety in the number of matching breathing efforts on a per-subject level, which ranged from 66.1 to 98.5% (see the supplementary materials at http://www.rcjournal.com for detailed per-subject results).
detection. There was a great variety in the number of matching breathing efforts on a per-subject level, which ranged from 66.1 to 98.5% (see the supplementary materials at http://www.rcjournal.com for detailed per-subject results).
Temporal Relation Between and


The temporal relation could not be determined in 4 patients due to impaired signal quality of the  . Breathing effort time intervals for the selected stable recordings showed a statistically significant correlation (r = 0.95, P < .001) between
. Breathing effort time intervals for the selected stable recordings showed a statistically significant correlation (r = 0.95, P < .001) between  and
and  . The mean difference in the time intervals between
. The mean difference in the time intervals between  and
and  was 10.1 ms, with limits of agreement from –410 to 430 ms (Fig. 3).
was 10.1 ms, with limits of agreement from –410 to 430 ms (Fig. 3).

A: A scatterplot of peak-to-peak time intervals, showing the correlation between surface electrical activity of the diaphragm ( ) and transesophageal electrical activity of the diaphragm (
) and transesophageal electrical activity of the diaphragm ( ). B: Bland-Altman plot, showing the temporal agreement between
). B: Bland-Altman plot, showing the temporal agreement between  and
and  . The dashed lines indicate the limits of agreement.
. The dashed lines indicate the limits of agreement.
Discussion
This pilot study compared  with
with  in subjects who were invasively ventilated. Only 86.0% of all
in subjects who were invasively ventilated. Only 86.0% of all  that detected breathing efforts were matched by
that detected breathing efforts were matched by  recordings. In stable parts of the recordings, however,
recordings. In stable parts of the recordings, however,  and
and  had excellent temporal correlation. Further visual analysis revealed that the inability to determine breathing efforts with
had excellent temporal correlation. Further visual analysis revealed that the inability to determine breathing efforts with  was mainly caused by impaired signal quality. Recently, surface and esophageal electromyography were compared in healthy subjects after phrenic stimulation. As with our study, esophageal signal amplitudes were higher than amplitudes of surface electromyography.21
was mainly caused by impaired signal quality. Recently, surface and esophageal electromyography were compared in healthy subjects after phrenic stimulation. As with our study, esophageal signal amplitudes were higher than amplitudes of surface electromyography.21
High body mass indices and thus increased electrode-to-diaphragm distance could have influenced the  signal strengths. Although interindividual variability in signal strengths was high, the ratio of
signal strengths. Although interindividual variability in signal strengths was high, the ratio of  to
to  remained relatively stable between the successive breathing efforts per subject. Differences in signal strengths between patients might indicate an effect of differences in anatomy and measurement conditions. Because electrodes were placed after palpation, we could not rule out the possibility of variety in the electrode-to-diaphragm distance among subjects. The
remained relatively stable between the successive breathing efforts per subject. Differences in signal strengths between patients might indicate an effect of differences in anatomy and measurement conditions. Because electrodes were placed after palpation, we could not rule out the possibility of variety in the electrode-to-diaphragm distance among subjects. The  was thereby more susceptible for signal disturbances and noise than
was thereby more susceptible for signal disturbances and noise than  . Activity of the abdominal muscles near the diaphragm could have interfered with the diaphragmatic activity. This phenomenon, also known as cross-talk, might be a disadvantage of surface electromyography.22
. Activity of the abdominal muscles near the diaphragm could have interfered with the diaphragmatic activity. This phenomenon, also known as cross-talk, might be a disadvantage of surface electromyography.22
In our study, coughing or subject movements could have interfered with  measurements. However, visual analysis of stable recordings showed similar
measurements. However, visual analysis of stable recordings showed similar  and
and  tidal breathing curves (Fig. 1). This suggested that minimal interference of adjacent muscle activity was present in these parts of the recording. Unfortunately, our study was too small to determine possible external causes of impaired
tidal breathing curves (Fig. 1). This suggested that minimal interference of adjacent muscle activity was present in these parts of the recording. Unfortunately, our study was too small to determine possible external causes of impaired  signal quality. Although not interfering with the
signal quality. Although not interfering with the  recording, the sternocleidomastoid and parasternal muscles also contribute to inspiration. However, the diaphragm is the main inspiratory muscle and, therefore, is a reliable signal for triggering invasive ventilation. Thus we chose to compare only
recording, the sternocleidomastoid and parasternal muscles also contribute to inspiration. However, the diaphragm is the main inspiratory muscle and, therefore, is a reliable signal for triggering invasive ventilation. Thus we chose to compare only  with
with  .
.
The  and
and  signals were processed differently. The
signals were processed differently. The  signal was processed with the double-subtraction technique and was smoothed with an exponential filter, whereas the
signal was processed with the double-subtraction technique and was smoothed with an exponential filter, whereas the  signal was processed with a root mean square signal.19,23 Therefore, peak amplitudes of
signal was processed with a root mean square signal.19,23 Therefore, peak amplitudes of  and
and  have a quadratic difference. Studies so far have used different thresholds for analysis of
have a quadratic difference. Studies so far have used different thresholds for analysis of  breathing effort detection.9,24 Because signal strengths were higher in
breathing effort detection.9,24 Because signal strengths were higher in  , we chose a uniform threshold based on the percentage of maximum peak signals to compare
, we chose a uniform threshold based on the percentage of maximum peak signals to compare  with
with  .
.
So far,  has been studied in subjects with COPD without invasive ventilation, neonates on noninvasive respiratory support, and in healthy subjects without invasive ventilation in which
has been studied in subjects with COPD without invasive ventilation, neonates on noninvasive respiratory support, and in healthy subjects without invasive ventilation in which  was compared with
was compared with  .16,18,21,25,26 As a proof of concept, we were interested in the best possible performance of
.16,18,21,25,26 As a proof of concept, we were interested in the best possible performance of  compared with
compared with  during invasive ventilation. Therefore, 10 successive breathing efforts per subject were visually selected on parts of the recordings without signal disturbances. In these parts, we found excellent temporal correlation and good agreement between the matching
during invasive ventilation. Therefore, 10 successive breathing efforts per subject were visually selected on parts of the recordings without signal disturbances. In these parts, we found excellent temporal correlation and good agreement between the matching  and
and  breathing efforts.
breathing efforts.
Recently, Beloncle et al27 showed, in a small study, that  -based monitoring of subjects during supportive invasive ventilation can improve patient-ventilator interaction. Synchrony between patient and the ventilator during invasive ventilation is pivotal to minimize adverse events,
-based monitoring of subjects during supportive invasive ventilation can improve patient-ventilator interaction. Synchrony between patient and the ventilator during invasive ventilation is pivotal to minimize adverse events,  provides additional information about patients' efforts during invasive ventilation and thus might function as a noninvasive bedside monitoring tool in the future.28,29 However, because of the many signal instabilities in our recordings, this method is not yet reliable and more research has to be conducted to address external causes of signal noise.
provides additional information about patients' efforts during invasive ventilation and thus might function as a noninvasive bedside monitoring tool in the future.28,29 However, because of the many signal instabilities in our recordings, this method is not yet reliable and more research has to be conducted to address external causes of signal noise.
Limitations
This study had some limitations. Most importantly, the small number of subjects precluded us from designating factors that significantly impaired the performance of  We, therefore, were unable to perform a subgroup analysis. Furthermore, we recorded
We, therefore, were unable to perform a subgroup analysis. Furthermore, we recorded  and
and  over a short period of time and only once in each patient. Therefore, the reproducibility of
over a short period of time and only once in each patient. Therefore, the reproducibility of  compared with
compared with  was not assessed. More so, our algorithm for automatic breathing effort detection was not capable of discriminating the stable from the instable recordings.
was not assessed. More so, our algorithm for automatic breathing effort detection was not capable of discriminating the stable from the instable recordings.
Conclusions
We found that  was not reliable for breathing effort detection in adult subjects invasively ventilated because of signal instabilities. However, in stable situations,
was not reliable for breathing effort detection in adult subjects invasively ventilated because of signal instabilities. However, in stable situations,  and
and  had excellent temporal correlation and good agreement. Although optimization of
had excellent temporal correlation and good agreement. Although optimization of  is necessary, these findings indicated that
is necessary, these findings indicated that  has potential as a monitoring tool during invasive ventilation.
has potential as a monitoring tool during invasive ventilation.
Footnotes
- Correspondence: Joost LC Lokin MD, Department of Intensive Care, Amsterdam UMC, location AMC, Postbus 22660 1100 DD Amsterdam Zuidoost, the Netherlands. E-mail: j.l.lokin{at}amsterdamumc.nl
The study was performed at the Department of Intensive Care, Amsterdam UMC, Amsterdam University Medical Center, location AMC, Amsterdam, the Netherlands.
The authors have disclosed no conflicts of interest.
Trialregister.nl study registration NTR4766, 01/09/2014.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}