

Abstract
BACKGROUND: A spontaneous breathing trial (SBT) is commonly used to determine extubation readiness in patients receiving mechanical ventilation. However, the physiological impact of such a trial in preterm infants has not been well described. This study aimed to investigate the effects of a 3-min SBT on the cardiorespiratory stability of these infants.
METHODS: A retrospective analysis of prospectively collected data was done for infants < 37 weeks gestational age who were extubated after a successful 3-min SBT. Heart rate,  , breathing frequency, exhaled tidal volume, and Silverman Andersen Respiratory Severity Score (SA-RSS) to assess work of breathing, before and at the end of the SBT, were recorded and compared using nonparametric paired Mann-Whitney tests. A secondary analysis was done between extubation success (ie, 72 h without the need for re-intubation) and failure groups. Differences were considered statistically significant if P < .05.
, breathing frequency, exhaled tidal volume, and Silverman Andersen Respiratory Severity Score (SA-RSS) to assess work of breathing, before and at the end of the SBT, were recorded and compared using nonparametric paired Mann-Whitney tests. A secondary analysis was done between extubation success (ie, 72 h without the need for re-intubation) and failure groups. Differences were considered statistically significant if P < .05.
RESULTS: A total of 90 SBTs were performed in 70 premature infants; 65 had a successful SBT, and 5 failed the SBT. Of the 65 infants who had a successful SBT and were extubated, 6 failed extubation (9.2%). Subjects had a median (interquartile range [IQR]) gestational age of 30 (27–33) weeks at birth, a birthweight of 1,240 (860–1,790) g, and weight at extubation of 1,790 (1,440–2,500) g. Cardiorespiratory stability was noted by a significant decrease in median (IQR) exhaled tidal volume (6.4 [4.9–8.4] mL/kg vs 5.2 (3.8–6.6] mL/kg, P < .001), a significant increase in mean ± SD breathing frequency (45.1 ± 11.4 vs 52.6 ± 14.4 breaths/min, P < .001), and a significant median (IQR) increase in work of breathing (SA-RSS of 1 [1–2] vs 2 [1–3], P < .001) at the end of the SBT. Respiratory instability was more remarkable in the success group.
CONCLUSIONS: In preterm infants receiving prolonged mechanical ventilation, the performance of a 3-min SBT was associated with increased respiratory instability while still leading to a 10% extubation failure rate. Therefore, the routine use of SBTs to assess extubation readiness in this population is not recommended until there are clear standards and definitions, as well as good accuracy to identify failures.
- spontaneous breathing trial
- mechanical ventilation
- ventilation weaning
- endotracheal extubation
- preterm infants
Introduction
Mechanical ventilation has been a remarkable advance in neonatal care responsible for a significant decrease in mortality, especially in preterm infants. However, prolonged mechanical ventilation exposure can be associated with short- and long-term complications such as bronchopulmonary dysplasia and neurodevelopmental impairment.1-3 While early extubation is frequently attempted, many neonates fail and require re-intubation and resumption of mechanical ventilation, which may further increase morbidities and mortality rates.4,5 In general, extubation is attempted when an infant is receiving mechanical ventilation at low ventilatory settings, is spontaneously breathing, and is hemodynamically stable. This decision is still mostly based on clinical experience and subjective judgment, leading to highly variable extubation practices and failure rates.6-8
To deal with the inaccurate nature of clinical judgment, a number of units have adopted the practice of performing a spontaneous breathing trial (SBT) to determine an infant’s readiness for extubation.6,9 An SBT is a challenge in which the infant receives minimal to no ventilatory support for a short duration while spontaneously breathing via the endotracheal tube. The infant is then extubated if they remain hemodynamically stable in accordance with predefined criteria.10,11 Although recognized as an evidence-based practice in adults and children, the safety and applicability of SBTs in neonates is less well-established.12-14 In a recent large cohort study, the use of a 5-min SBT in extremely preterm infants had low accuracy for predicting extubation failures and exposed nearly 60% of infants to some form of cardiorespiratory instability.9 Such information is not available for trials of a shorter duration in less immature preterm infants. Because our unit has adopted a weaning protocol incorporating an SBT to proceed with extubation, we performed this study to investigate the effects of a 3-min SBT on cardiorespiratory stability in preterm infants. As a secondary outcome, we performed an exploratory analysis to compare cardiorespiratory stability in infants who were successfully extubated or failed.
QUICK LOOK
Current Knowledge
In adult and pediatric patients, a spontaneous breathing trial (SBT) is a respiratory challenge that can provide useful information regarding the patient's ability to breathe spontaneously after disconnection from the ventilator. However, little research has been carried out to evaluate the physiological impact of such a challenge in the neonatal population, especially preterm infants.
What this article contributes to our knowledge
The performance of a 3-min SBT in preterm infants was associated with decreased exhaled tidal volume/kg, increased breathing frequency, and increased work of breathing without eliminating extubation failures. Therefore, until there are clear standards and definitions, and good accuracy to identify failures, we do not recommend the routine use of SBTs to assess extubation readiness in preterm infants.
Methods
Population and Setting
In July 2017, the neonatal ICU at the Waldemar Monastier Children's Hospital (Campo Largo, Paraná, Brazil) implemented a protocol whereby all infants receiving mechanical ventilation undergo an SBT when deemed ready for extubation by the medical team. Thus, in this study the inclusion criteria were all premature infants < 37 weeks of gestational age extubated after a successful SBT between July 2017 and April 2019. Infants who did not undergo an SBT were excluded from this study; these included infants with neurological or cardiac impairment, airway malformation, or suspected/confirmed genetic syndromes. Data were prospectively collected, and a retrospective analysis was performed. The study was approved by the Human Research Ethics Committee of the Hospital de Clínicas, Federal University of Paraná (18296113.0000.0096).
Weaning Protocol and SBT Procedure
All premature infants were mechanically ventilated with the Inter Neo, Inter 7, or Inter 5 ventilator (Intermed, São Paulo, Brazil) using a permissive hypercapnia strategy ( of 45–55 mm Hg for the first 3 d and 55–65 mm Hg afterwards, if pH > 7.20) and an
of 45–55 mm Hg for the first 3 d and 55–65 mm Hg afterwards, if pH > 7.20) and an  target of 91–95%. The protocol suggested infants were to be considered ready for extubation in the presence of all of the following criteria: (1)
target of 91–95%. The protocol suggested infants were to be considered ready for extubation in the presence of all of the following criteria: (1)  < 65 mm Hg, (2)
< 65 mm Hg, (2)  > 85% with
> 85% with  < 0.30, (3) heart rate > 100 beats/min, (4) low ventilatory settings (ie, peak inspiratory pressure < 20 cm H2O; PEEP < 7 cm H2O, and ventilator rate < 30 inflations/min), and (5) hemodynamically stable (ie, normal blood pressure for the gestational age without use of inotropes).
< 0.30, (3) heart rate > 100 beats/min, (4) low ventilatory settings (ie, peak inspiratory pressure < 20 cm H2O; PEEP < 7 cm H2O, and ventilator rate < 30 inflations/min), and (5) hemodynamically stable (ie, normal blood pressure for the gestational age without use of inotropes).
SBTs were performed by the physiotherapist (ie, the equivalent of a respiratory therapist in North America) on duty once infants met the readiness criteria. Prior to the SBT, the physiotherapist confirmed the correct positioning and fixation of the endotracheal tube and performed suctioning. The SBT was performed with the neonate in a supine position and consisted of a 3-min period in which the infant received CPAP via the endotracheal tube at the same level of PEEP used during mechanical ventilation and without pressure support. The protocol mandated annotation of the following cardiorespiratory parameters by the physiotherapist before and immediately after the end of the trial: heart rate,  , breathing frequency, exhaled tidal volume, exhaled tidal volume per kilogram, and Silverman-Andersen Respiratory Severity Score (SA-RSS).15 Heart rate,
, breathing frequency, exhaled tidal volume, exhaled tidal volume per kilogram, and Silverman-Andersen Respiratory Severity Score (SA-RSS).15 Heart rate,  , and breathing frequency were obtained from the bedside monitors (Mindray iMEC12, Umec12, PM700 or PM900, Mindray Medical International, China); exhaled tidal volumes were obtained from the ventilators; and SA-RSS was calculated by evaluating 5 parameters with a numerical score of 0–2 for each parameter: (1) thoracoabdominal synchrony, (2) lower chest retractions, (3) xiphoid retractions, (4) nasal flaring, and (5) expiratory grunting. SA-RSS scores ≤ 3 were defined as low, scores of 3–5 as moderate, and scores > 5 as severe. SBT failure was defined as the presence of any of the following criteria: (1) 20% decrease or increase in baseline heart rate; (2) drop in
, and breathing frequency were obtained from the bedside monitors (Mindray iMEC12, Umec12, PM700 or PM900, Mindray Medical International, China); exhaled tidal volumes were obtained from the ventilators; and SA-RSS was calculated by evaluating 5 parameters with a numerical score of 0–2 for each parameter: (1) thoracoabdominal synchrony, (2) lower chest retractions, (3) xiphoid retractions, (4) nasal flaring, and (5) expiratory grunting. SA-RSS scores ≤ 3 were defined as low, scores of 3–5 as moderate, and scores > 5 as severe. SBT failure was defined as the presence of any of the following criteria: (1) 20% decrease or increase in baseline heart rate; (2) drop in  to < 85% for any duration; (3) SA-RSS > 5. If any of these occurred, the trial was stopped and the failure criteria were recorded. If none of these occurred, the SBT was deemed successful and the infant was extubated as per protocol.
to < 85% for any duration; (3) SA-RSS > 5. If any of these occurred, the trial was stopped and the failure criteria were recorded. If none of these occurred, the SBT was deemed successful and the infant was extubated as per protocol.
As a result of implementing a weaning protocol in our unit, all infants were extubated at the recommended levels of respiratory support, except for one infant in whom the SBT was performed at a PEEP of 7 cm H2O (ie, in the failure group). We observed that all extubation decisions were made in full compliance with the results of the SBT, meaning that only infants who passed the SBT were extubated. Such adherence to the protocol led to a reduction in practice variability and harmonized the approach to extubation in our unit.
Clinical Data
The following information concerning subject demographics and ventilatory parameters prior to each successful SBT was extracted from medical records: birthweight, gestational age, gestational age at extubation, use of surfactant, Apgar at 1 min and at 5 min, duration and modes of mechanical ventilation, peak inspiratory pressure, pressure support level, PEEP,  , total breathing frequency prior to SBT, and type of noninvasive support used after extubation. Moreover, for each successful SBT, the outcome of the extubation (ie, success or failure) was determined. Extubation success was defined as 72 h without the need for re-intubation and mechanical ventilation.
, total breathing frequency prior to SBT, and type of noninvasive support used after extubation. Moreover, for each successful SBT, the outcome of the extubation (ie, success or failure) was determined. Extubation success was defined as 72 h without the need for re-intubation and mechanical ventilation.
The primary objective of this study was to evaluate the impact of a 3-min SBT prior to extubation on cardiorespiratory stability of preterm infants. Cardiorespiratory stability was assessed by using the heart rate,  , exhaled tidal volume, breathing frequency, and SA-RSS immediately before and after passing the SBT. These data were extracted from the physiotherapist notes. As an exploratory analysis, cardiorespiratory stability was compared between infants who were successfully extubated or failed extubation.
, exhaled tidal volume, breathing frequency, and SA-RSS immediately before and after passing the SBT. These data were extracted from the physiotherapist notes. As an exploratory analysis, cardiorespiratory stability was compared between infants who were successfully extubated or failed extubation.
Statistical Analysis
The results were presented from descriptive statistical analysis (mean ± SD; absolute frequency and percentages; median with interquartile range and range). For the primary outcome, due to non-normality of the data (as assessed using the Shapiro-Wilk test), cardiorespiratory parameters were compared before and after the passed SBT using nonparametric paired Mann-Whitney tests. As a secondary outcome, cardiorespiratory parameters were compared separately for infants with successful extubation and those who failed extubation to determine any differential response to the SBT between the groups. Differences were considered statistically significant if P < .05. Statistical analysis was performed using Stata 16 (StataCorp, College Station, Texas).
Results
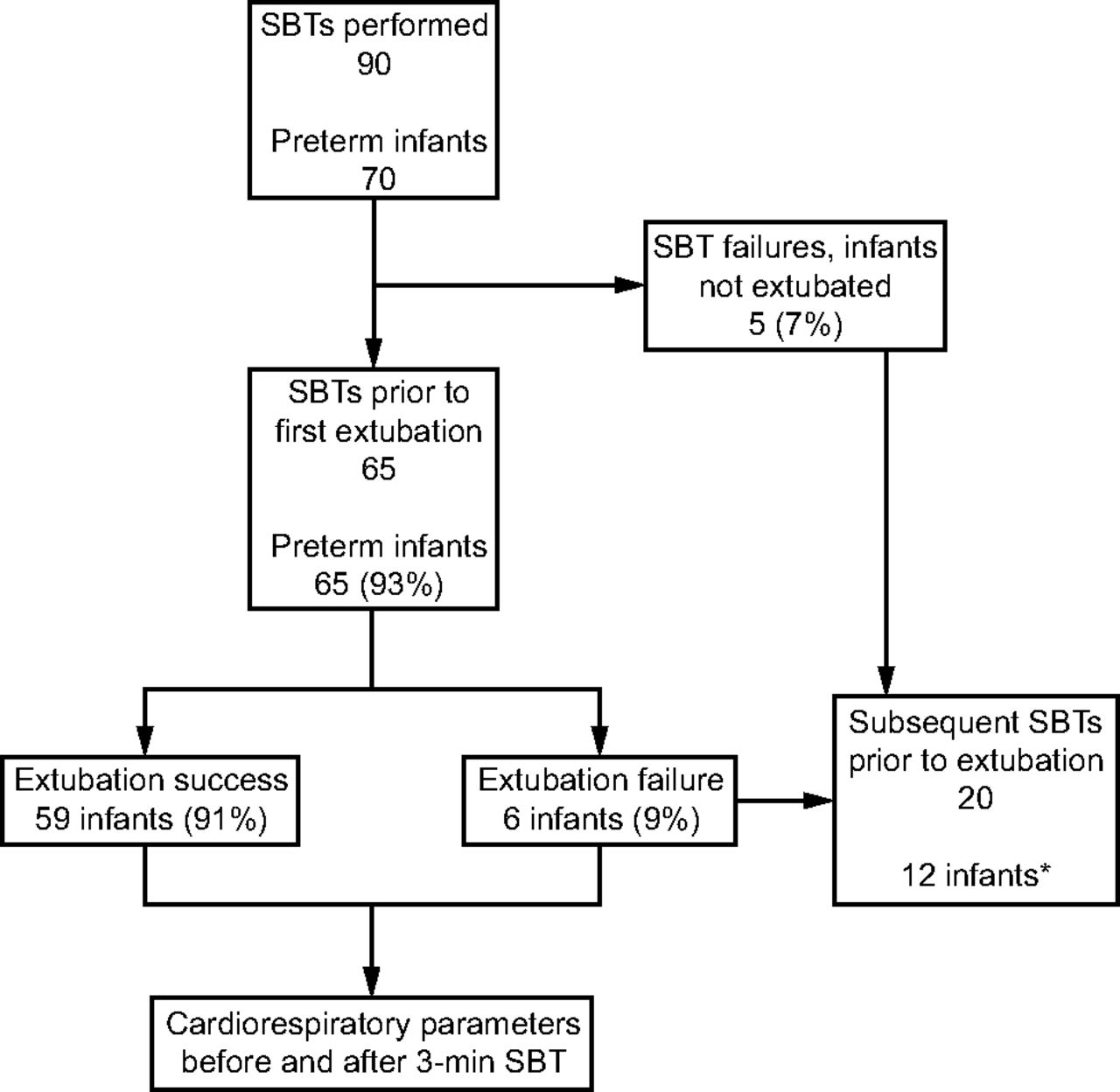
During the study period, a total of 90 SBTs in 70 premature infants were performed; 65 had a successful SBT, and 5 failed the SBT. Only the preterm infants who passed the SBT were analyzed. Of the 65 subjects who had a successful SBT and were extubated, 6 (9.2%) failed their first extubation attempt. Details of patient flow during the study period are provided in Figure 1.

Flow chart. SBT = spontaneous breathing trial. *1 infant was subsequently re-intubated and another SBT was performed.
Subject characteristics are described in Table 1. Premature infants had a median (interquartile range) gestational age of 30 (27–33) weeks at birth, birthweight of 1,240 (860–1,790) g, and weight at extubation of 1,790 (1,440–2,500) g. Before the SBT, most subjects (95%) were receiving synchronized intermittent mandatory ventilation. Peak inspiratory pressure and PEEP levels were significantly higher in infants who failed extubation. After extubation, CPAP was the most commonly used mode of noninvasive respiratory support: 83% in the successful group and 95% in the failure group.
Subject Demographics and Ventilatory Parameters Prior to SBT and Extubation Outcomes
The impact of the SBT on cardiorespiratory stability was noted by changes in respiratory parameters. After a 3-min successful trial, there was a significant decrease in exhaled tidal volume per kilogram and an increase in breathing frequency and work of breathing (WOB) as assessed with SA-RSS (Table 2). An exploratory analysis was performed for the groups of infants who were successfully extubated or failed. Respiratory instability was noted in both groups. However, likely due to the larger sample size, these effects were more remarkable in the group of infants successfully extubated (Table 3).
Cardiorespiratory Parameters Before and After a 3-min SBT
Cardiorespiratory Parameters Before and After a 3-min SBT and Extubation Outcomes
Discussion
In this study, we evaluated the physiological impact of performing a 3-min SBT for the assessment of extubation readiness in preterm infants. Most infants were successfully extubated, but they also exhibited a significant decrease in exhaled tidal volume per kilogram and increases in breathing frequency and WOB at the end of the trial. These data shed some light on the clinical safety and usefulness of an SBT as it pertains to preterm infants.
Neonatologists around the world have increasingly adopted the practice of performing SBTs in preterm infants, despite the limited evidence guiding its use in this population.6,12,13,16 Clinicians endorsing SBTs have typically justified practice based on a standardized assessment of extubation readiness (ie, to reduce clinical practice variations), identification of an infant’s potential for extubation as early as possible (ie, to reduce unnecessary exposure to mechanical ventilation), and the ability to accurately identify infants who will fail extubation and thus prevent them from being extubated. To achieve the latter goal, the SBT is intentionally designed to impose a certain level of physiological stress on the patient to differentiate between infants capable of tolerating extubation and those who will not tolerate extubation.
Moreover, the criteria used to determine SBT success or failure were easy to follow and provided a more objective determination of the infant’s readiness for extubation. Indeed, there is ample evidence from the adult, pediatric, and (to a lesser extent) neonatal literature that protocolized weaning from the ventilator improves clinical outcomes, reduces costs, enhances educational opportunities for trainees, and strengthens therapeutic alliance with the families through the provision of streamlined care.11,17-20 A recent study reported that the implementation of a 2-step extubation readiness test, which included a 3-min SBT, in a cohort of moderate to late preterm and term infants harmonized extubation practices while also reducing extubation failure rates; however, it was unclear whether it was the specific use of an SBT or the implementation of a respiratory therapist–driven protocol that conferred the greatest benefits.16
The use of our SBT protocol had some effect on weaning success as only 5 of the 70 preterm infants failed their first SBT attempt. However, at the time of the first SBT, infants had been ventilated for a long period (median 14 d), were considerably mature, and had an average weight of nearly 2 kg. This suggests that the SBT was performed when the chance of a success was already very high. In other words, once an infant was considered ready, the SBT provided very little additional information in terms of determining the infant’s potential for extubation. This finding is in keeping with 2 prior studies that also reported no beneficial effects of SBT use on weaning durations.13,16 Thus, it is possible that the SBT may have been more useful if it had been performed earlier.
Despite passing an SBT, almost 10% of preterm infants failed their first extubation attempt. Although no data were available from our unit regarding extubation failure rates prior to SBT implementation, this remains a relatively high percentage of failure given the characteristics of our population, which is primarily composed of more mature infants extubated at a high weight.7,8 These findings are in keeping with a systematic review and meta-analysis that established the low specificity of the SBT.9 Likewise, these results parallel those obtained in another study in which implementation of an SBT protocol did reduce the extubation failure rates among a cohort of very low birthweight infants.13 Therefore, our results confirm that a 3-min SBT adds little benefit for the identification of extubation failures. A possible explanation for the relatively high extubation failure rate seen in our cohort is that the duration, PEEP level, and definition of SBT success or failure may have been ill-suited for the detection of failures specific to our population. For instance, the duration of 3 min may have been insufficient to capture extubation failures related to unsustained respiratory drive. Moreover, given that SBTs were conducted using an average PEEP level of nearly 6 cm H2O, this amount of support may have been too high to accurately capture the true extubation failures.21 Finally, it is plausible that a different definition of SBT success or failure may have had a better ability to distinguish those infants with successful or failed extubation. However, in the recent diagnostic study by Shalish et al,9 after evaluating > 40,000 different definitions of SBT success and failure, none were able to improve the accuracy of detection of extubation failures among extremely preterm infants.
After evaluating for changes in cardiorespiratory parameters before and after the SBT, we noted a statistically significant increase in exhaled tidal volume per kilogram, breathing frequency, and WOB at the end of the 3-min SBT. Indeed, the presence of an endotracheal tube, without the mechanical inflations from the ventilator, is associated with an increase in dead space and airway resistance.22 This is the reason why SBTs of shorter duration have been proposed for preterm infants. In our study, despite using a short SBT duration that nearly all infants successfully passed, almost 10% still required re-intubation and experienced a significant increase in breathing frequency and WOB during the trial. Similar results were observed in a recent large cohort study of > 250 extremely preterm infants, in which a 5-min endotracheal CPAP trial exposed nearly 60% of infants to some form of clinical instability without any added benefit in identifying extubation failures.9
In this study, we attempted a subgroup analysis to determine whether the 6 infants who failed extubation had a different cardiorespiratory response compared to those infants with a successful extubation. The infants who failed extubation did not mount a statistically significant increase in breathing frequency or WOB following the SBT. Thus, it is possible that the inability to increase breathing frequency and WOB during a trial might be an indicator of worse respiratory function and a predictor of readiness in this population, as demonstrated in adults.23 However, given the very small number of failures, the data provided here do not support a detectable difference that could be used clinically and remains a hypothesis-generating theory that should be further explored in larger studies.
Our study has limitations. As in any retrospective analysis, there were some missing data, and data on endotracheal tube size and length were not collected. Because we did not collect data from a historical cohort of infants who were extubated prior to implementation of the protocol, it was not possible to quantify the exact impact of this protocol on clinical outcomes. However, the SBT was performed using standard methodology in all infants, and cardiorespiratory measurements were collected and compared for each patient, before and after the SBT. Cardiorespiratory parameters were extracted from the monitors at 2 time points, and continuous monitoring of those parameters would have allowed for a more detailed analysis over time as well as the use of other analytical methods. Thus, we provide important information concerning the impact of a short SBT on cardiorespiratory stability in preterm infants receiving prolonged mechanical ventilation and extubated from low ventilatory settings.
Conclusions
In preterm infants receiving prolonged mechanical ventilation, the performance of a 3-min SBT as part of a weaning protocol was associated with decreased exhaled tidal volume per kilogram and increased breathing frequency and WOB while still allowing a 10% extubation failure rate. Therefore, we do not recommend the routine use of SBTs to assess extubation readiness in preterm infants until there are clear standards and definitions, and good accuracy to identify failures.
ACKNOWLEDGMENTS
The authors thank Dr W Shalish and G Sant’Anna from McGill University, Montreal, Canada, for the critical review of the manuscript. We also acknowledge the team of the neonatal ICU at the Waldemar Monastier Children's Hospital.
Footnotes
- Correspondence: Adriane M Nakato PT PhD, Rua Imaculada Conceição 1155, Prado Velho, Curitiba, Paraná, Brazil, CEP 80215–901. E-mail: adrianemuller{at}hotmail.com
This work was supported in part by Conselho Nacional de Desenvolvimento Científico e Tecnológico and Fundação Araucária/Coordenação de Aperfeiçoamento de Pessoal de Nível Superior. The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}