

Abstract
BACKGROUND: Clinical alarms play an important role in monitoring physiological parameters, vital signs and medical device function in the hospital intensive care environment. Delays in staff response to alarms are well documented as health care providers become desensitized to increased rates of nuisance alarms. Patients can be at increased risk of harm due to alarm fatigue. Current literature suggests alarms from ventilators contribute significantly to nonactionable alarms. A greater understanding of which specific ventilator alarms are most common and the rates at which they occur is fundamental to improving alarm management.
METHODS: A retrospective review was performed on alarms that occurred on the Avea and Servo-i ventilators used in the pediatric ICU and pediatric cardiothoracic ICU at a major metropolitan children’s hospital. High- and medium-priority alarms, as classified by the manufacturer, were studied between June 1, 2017, and November 31, 2017. Descriptive data analysis and a 2-proportion z-test were performed to identify proportionality, cause, and prevalence rates in the pediatric ICU and the cardiothoracic ICU.
RESULTS: Eleven distinct ventilator alarms were identified during 2,091 d of mechanical ventilation. The Inspiratory Flow Overrange alarm (42.4%) on the Servo-i, Low VTE (20.4%; expiratory tidal volume) and Circuit Integrity alarm (20.0%) on the Avea were the most prevalent causes according to ventilator type. Medium-priority alarms comprised 68.7% of all Servo-i alarms, and high-priority alarms comprised 84% of all Avea alarms. The 2-sample test of proportions was significant for differences between both areas (P < .001). The overall alarm prevalence rate was 22.5 ventilator alarms per ventilator-day per patient.
CONCLUSIONS: The cause and proportion of alarms varied by ventilator and care unit. High-priority alarms were most common with the Avea and medium-priority alarms for the Servo-i. The overall combined ventilator alarm prevalence rate was 22.5 alarms per ventilator-day per patient.
- ventilator alarms
- frequency
- prevalence
- proportionality
- cause
- rate
- alarm fatigue
- critical alarm
- alarm priority
- pediatric intensive care unit
Introduction
Clinical alarms and physiologic monitors are pervasive and are an established part of critical care in the hospital setting. The goal of physiologic monitors and clinical alarms is to provide early warnings to redirect attention to a potential impending critical event, thereby allowing early intervention and prevention of a critical event.1 Physiologic monitors provide audible and visual alerts as parameters move outside of set alarm thresholds.
Many medical devices also possess their own monitoring alarm systems. For example, ventilators, intravenous infusion pumps, feeding pumps, hospital beds, and other medical devices have their own unique alarms adding to the milieu of sounds that are seen, heard, and experienced in the hospital setting. Some medical devices are highly complex. A few ventilators offer > 100 different types of alarms.2 In addition, there are large proportions of nonactionable clinical alarms that do not require clinical intervention and contribute to what has been described as alarm fatigue.3-6 The ubiquitous prevalence of alarms can cause caregivers to become desensitized, exhibited through delayed or ignored responses to ventilator alarms in the ICU.7-9
Ventilator alarms may contribute to alarm fatigue by adding to the total number of nonactionable alarms. Ventilator alarms comprise 16–45% of all clinical alarms generated in the operating room setting.3,10 A large proportion of ventilator-specific alarms (as high as 73% in the adult ICU) are nonactionable.11 The high proportion of nonactionable ventilator alarms is closely connected to the current issues surrounding alarm fatigue and patient safety.
The concern with alarm safety is at the forefront of regulatory agencies, professional organizations, and patient safety organizations. The Emergency Care Research Institute (ECRI) highlighted the danger of excessive nonactionable alarms by reporting alarm fatigue as their number one safety concern for 2 successive years in 2012 and 2013. Further, ECRI reported health technology hazards related to alarm alert and notification overload as one of their top 10 concerns for 2020.12 For more than a decade, the Joint Commission and FDA, a government regulatory agency that establishes regulations and standards and provides oversight for medical devices, have drawn attention to alarm safety as a concern through their official communications, safety initiatives, and recommendations. In 2003, the Joint Commission highlighted alarm safety as a National Patient Safety Goal and raised the concern even higher through the 2013 Joint Commission Sentinel Report.13 Ninety-eight alarm-related events were reported to have occurred nationally between 2009 and 2012; 80 of these cases ended in death.13 In 2010, the FDA received 2,500 ventilator-related adverse event reports, and approximately 33% were found to be due to alarm-related issues.14 No recent studies were available on ventilator-related injuries.
As health care organizations strive for zero patient harm, one clinical alarm- or medical error-related death is too many.15 A single ventilator alarm incident can result in patient demise and be a tragedy for the patient, family, staff, and organization. Ventilator alarms can add a significant burden to the concerns surrounding alarm fatigue. Understanding ventilator alarm characteristics such as alarm rates, proportionality, and variations due to ventilator design are some of the fundamental details needed to enhance alarm safety. The purpose of this study was to determine the frequency, prevalence rates, and cause of high- and medium-priority ventilator alarms. This new knowledge can help policymakers be more strategic in developing alarm practice standards that are directed at the most common types of alarms. Lastly, manufacturers can utilize these findings in the design of more effective and consistent alarm systems to help reduce the overall alarm burden caused by ventilator alarms.
QUICK LOOK
Current knowledge
Ventilator alarms make up a large segment of all clinical alarms in the pediatric ICU and have added to the overall burden of alarm fatigue. However, alarm characteristics such as prevalence rates, proportions, and causes are not well understood. Very little has been published on alarm management practices and guidelines. Understanding ventilator alarm characteristics could be an important first step in an evidence-based approach to develop policies for alarm management.
What this paper contributes to our knowledge
Ventilator alarms occurred in pediatric ICUs at a prevalence rate of 22.5 ventilator alarms per day of mechanical ventilation. The most common ventilator alarms were related to high inspiratory flow, high respiratory frequency and high airway pressures. Ventilator alarm proportions were significantly different between the brands of ventilators.
Methods
A retrospective study was performed on ventilator alarm occurrences for 2 common types of ventilators used in the pediatric ICU (PICU) and pediatric cardiothoracic intensive care unit (CTICU) between June 1, 2017, and November 31, 2017 (110 d) at Children’s Hospital Los Angeles, a major metropolitan children’s hospital in Los Angeles, California. Study approval was obtained from the institutional review boards at Children’s Hospital Los Angeles and Loma Linda University. Collected data included ventilator alarm information for the Avea ventilator (Carefusion, San Diego, California) and the Servo-i ventilator (Maquet, Rastatt, Germany) gathered through the proprietary Philips monitor alarm audit tool (Philips IntelliVue PIIC iX system, Amsterdam, Netherlands).
The ventilator alarm log report included Apnea, Circuit Integrity, High Airway Respiratory Rate (awRR), High peak inspiratory pressure (Paw), High Minute Ventilation ( ), High Tidal Volume (VT), Low Peak Pressure (Ppeak), Low PEEP, Low Exhaled VT (VTE), Low/High
), High Tidal Volume (VT), Low Peak Pressure (Ppeak), Low PEEP, Low Exhaled VT (VTE), Low/High  , and Inspiratory Flow Overrange. Circuit Integrity and Inspiratory Flow Overrange alarms were proprietary alarms unique to the Avea ventilator and the Servo-i, respectively, and both alarms were determined by manufacturer software algorithms. The Circuit Integrity alarm on the Avea was activated when the ventilator sensed a circuit occlusion condition on the inspiratory or expiratory limb. The Inspiratory Flow Overrange alarm on the Servo-i occurred when a combination of parameter settings created a condition outside of the allowable inspiratory flow range. For example, in the infant mode, if the subject required inspiratory flows exceeding 33 L/min, the Inspiratory Flow Overrange alarm was activated.
, and Inspiratory Flow Overrange. Circuit Integrity and Inspiratory Flow Overrange alarms were proprietary alarms unique to the Avea ventilator and the Servo-i, respectively, and both alarms were determined by manufacturer software algorithms. The Circuit Integrity alarm on the Avea was activated when the ventilator sensed a circuit occlusion condition on the inspiratory or expiratory limb. The Inspiratory Flow Overrange alarm on the Servo-i occurred when a combination of parameter settings created a condition outside of the allowable inspiratory flow range. For example, in the infant mode, if the subject required inspiratory flows exceeding 33 L/min, the Inspiratory Flow Overrange alarm was activated.
The standard clinical policy and procedure for setting ventilator alarms was followed for this study, and no modifications were made during this study period. Institutional ventilator alarm policy consisted of high pressure limit set at 10–15 cm H2O above peak inspiratory pressure; low pressure limit at 5 cm H2O below peak inspiratory pressure; low  at not less than one half of the patient’s measured
at not less than one half of the patient’s measured  ; and
; and  ± 10% of baseline (Table 1). The bedside clinician’s clinical judgment was used to determine appropriate alarm parameter settings for alarms not covered in policy.
± 10% of baseline (Table 1). The bedside clinician’s clinical judgment was used to determine appropriate alarm parameter settings for alarms not covered in policy.
Ventilator Alarm Parameter Settings
During the study, the Servo-i ventilator was the favored ventilator in the CTICU due to staff comfort and familiarity. The Avea was preferred for the PICU because of its ability to measure transpulmonary pressure. The Servo-i ventilator was also used in the PICU. Patients admitted to the PICU on ventilators other than the Avea or Servo-i ventilators were excluded from the study due to technical limitations on data collection (ie, the Sensormedics 3100a, Sensormedics 3100b, and home ventilators did not have the capability to interface with the Philips middleware and data collection system).
Data analysis was performed using Matlab (version 9.4, MathWorks, Natick, Massachusetts) and Microsoft Excel (Microsoft, Redmond, Washington) to quantify ventilator alarm frequency, prevalence rate, proportionality, and type of alarms activated according to clinical settings and alarm priority. The alarm priority designation of low-, medium-, and high-priority alarms was determined according to the manufacturers’ interpretation of existing guidance, requirements, and recommendations from the FDA. Professional organizations such as the American Association for Respiratory Care (AARC) provided expert opinion through a ventilator consensus statement.16 Collected alarm data were also analyzed in subgroups based on the 2 different types of ventilators. A 2-sample z-test of proportions between the PICU and the CTICU was performed to identify differences in alarm prevalence rates for common ventilator alarms.
Results
The PICU and CTICU alarm log identified 11 unfiltered types of ventilator alarms. These 11 distinct alarms were classified as medium-priority or high-priority ventilator alarms specific to the Avea and Servo-i during 2,091 d of mechanical ventilation (Table 2). A ventilator day was defined as any portion of a 24-h period requiring mechanical ventilation. A total of 47,099 ventilator alarm conditions were included in this analysis.
Manufacturer Alarm Priority Classification for the Avea and Servo-i Ventilators
Prevalence Rate of Ventilator Alarms
The combined PICU and CTICU incidence rate of ventilator alarms was 22.5 ventilator alarms per day of mechanical ventilation per patient measured over 2,091 d (Table 3). The PICU had 24.9 ventilator alarms per day of mechanical ventilation and the CTICU had a rate of 20.0 ventilator alarms per day of mechanical ventilation (Table 3). The ventilator alarm prevalence rate for the PICU was greater than that for the CTICU.
Frequency of Alarm Types in the Pediatric ICU and Cardiothoracic ICU
Proportionality of Ventilator Alarms
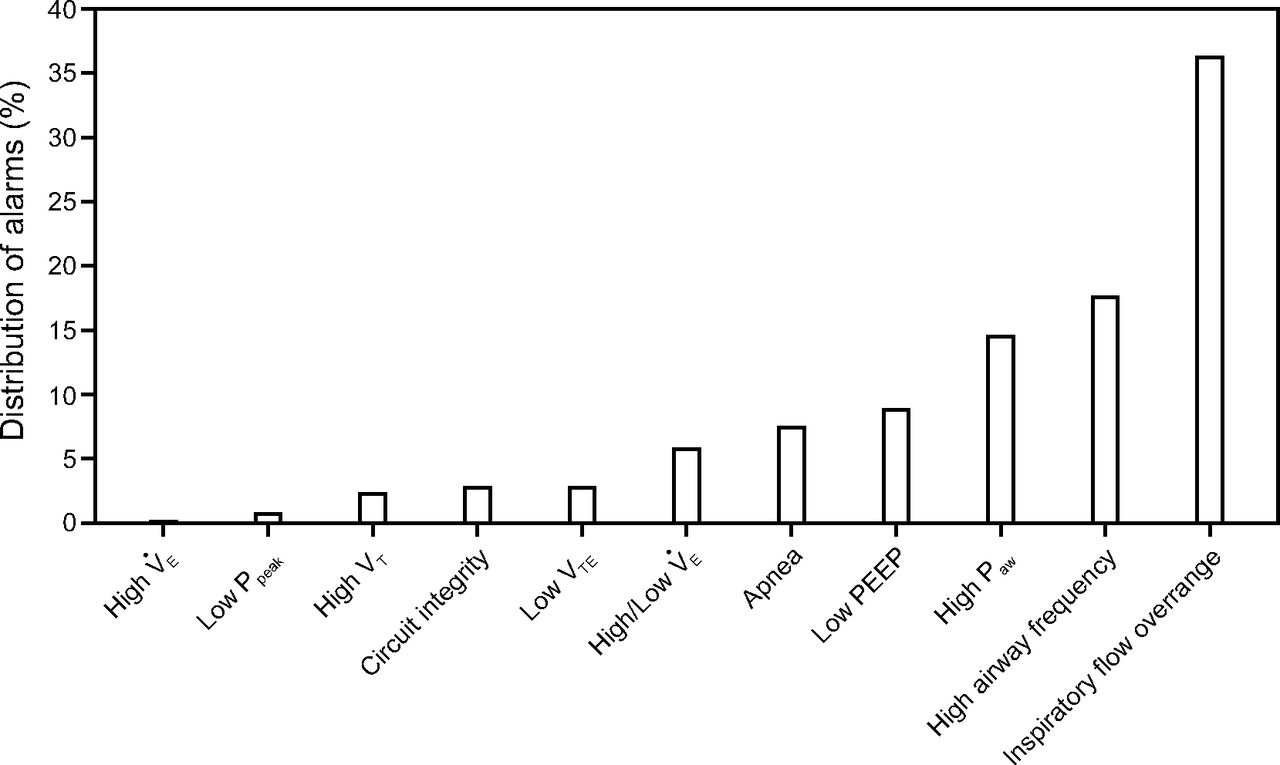
Overall, the Inspiratory Flow Overrange (36.6%) on the Servo-i, High awRR (17.8%), and High Paw (14.7%) alarms were the 3 most common ventilator alarms (Fig. 1, Table 3). The Inspiratory Flow Overrange alarm is determined by the ventilator algorithm on the Servo-i. The 2 most common alarms, Inspiratory Flow Overrange and High awRR, were classified as medium-priority alarms and comprised 54% of all alarms. In general, medium-priority alarms comprised 61.5% of all ventilator alarms, and high-priority alarms consisted of 38.5% of all ventilator alarms. The most common high-priority alarms were the High Paw and Apnea alarms on the Servo-i.
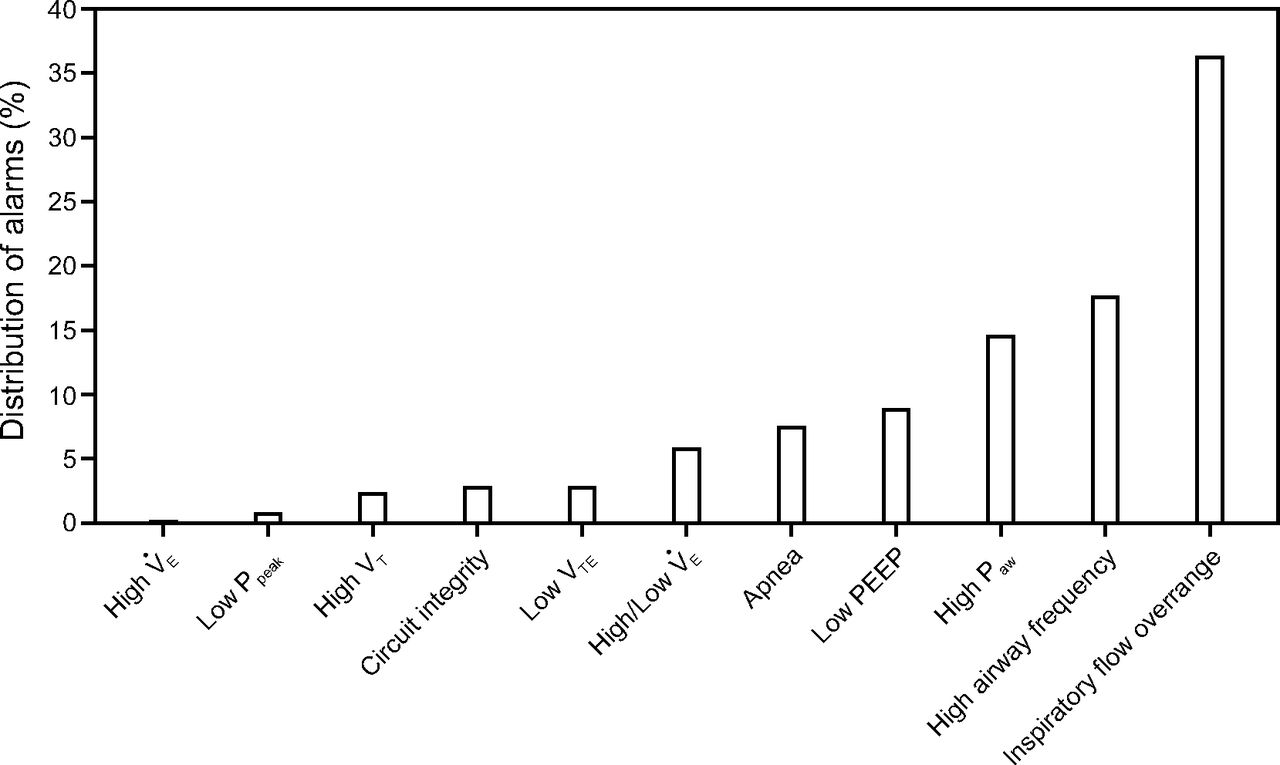
Distribution of types of ventilator alarms in the pediatric ICU and cardiothoracic ICU.  = minute ventilation; Ppeak = peak pressure; VT = tidal volume; VTE = end-tidal volume; Paw = high peak inspiratory pressure.
= minute ventilation; Ppeak = peak pressure; VT = tidal volume; VTE = end-tidal volume; Paw = high peak inspiratory pressure.
The High  (0.1%), Low Ppeak (0.7%), and High VT (2.3%) alarms were the least common ventilator alarms for both PICU and CTICU combined areas. The proportion of other alarms were Circuit Integrity (2.8%) and Low VTE (2.8%) alarms, specific to the Avea ventilator only, and the Low/High
(0.1%), Low Ppeak (0.7%), and High VT (2.3%) alarms were the least common ventilator alarms for both PICU and CTICU combined areas. The proportion of other alarms were Circuit Integrity (2.8%) and Low VTE (2.8%) alarms, specific to the Avea ventilator only, and the Low/High  (5.8%), Apnea (7.5%), and Low PEEP (8.9%) alarms for both ventilators.
(5.8%), Apnea (7.5%), and Low PEEP (8.9%) alarms for both ventilators.
Ventilator-Specific Results
The Servo-i had a larger number of medium-priority alarms (68.7%) (Table 3). The Inspiratory Flow Overrange was the most common type of alarm for the Servo-i (42.4%), followed by the High awRR (18.2%) and High Paw (17.0%) alarms. The Avea had a greater number of high-priority alarms (84.0%) (Table 4). Circuit Integrity (20.0%) and Low VT (20.4%) were the most common alarms for the Avea. The Circuit Integrity alarm in the Avea is predetermined by algorithms programmed by the manufacturer.
Alarm Frequency and Priority by Ventilator
The proportion of high- and medium-priority alarms, based on the type of ventilator, varied between the Avea and Servo-i ventilators (Table 4). The proportion of high- and medium-priority alarms with the Avea were 84% and 16%, respectively. Subsequently, the proportion for high- and medium-priority alarms for the Servo-i were 31.2% and 68.7%, respectively. Eight different types of alarms were reported for the Avea, and 6 distinct types of ventilator alarms were reported for the Servo-I; 4 types of alarms were common in both ventilators: Apnea, High  , Low PEEP, and High awRR.
, Low PEEP, and High awRR.
2-Proportion z-Test
A 2-proportion z-test was performed for the 6 types of ventilator alarms present on both the Servo-i and Avea ventilators. The prevalence of alarms was compared between the PICU and CTICU. The alarms observed were Apnea, High Paw, High awRR, Low PEEP, Low/High  , and Inspiratory Flow Overrange (Table 5). The 2-proportion z-test was statistically significant for differences in ventilator alarm proportions with both ventilators combined (Avea and Servo-i) and all 6 types of alarms compared. However, when testing for the Servo-i only, the Low PEEP alarm was not statistically significant. The other 5 alarms showed a statistically significant difference in proportions between both areas with the Servo-i only (P < .001) (Table 5). The only notable similarity between the 2 alarm frequencies in the PICU and CTICU was the Low PEEP when controlling for Servo-i only ventilators.
, and Inspiratory Flow Overrange (Table 5). The 2-proportion z-test was statistically significant for differences in ventilator alarm proportions with both ventilators combined (Avea and Servo-i) and all 6 types of alarms compared. However, when testing for the Servo-i only, the Low PEEP alarm was not statistically significant. The other 5 alarms showed a statistically significant difference in proportions between both areas with the Servo-i only (P < .001) (Table 5). The only notable similarity between the 2 alarm frequencies in the PICU and CTICU was the Low PEEP when controlling for Servo-i only ventilators.
2-Proportion z-Test for Ventilator Alarms Between Pediatric ICU and Cardithoracic ICU
Discussion
The studies by Schondelmeyer et al,18 Schmid et al,19 and Bridi et al20 maintained the idea that clinical alarms as a group occur at a high rate. Many studies also demonstrated a high incidence of nonactionable alarms.7,8,14,21 Researchers have studied the overall frequency of clinical alarms and the proportion of nonactionable alarms, but the specific causes and types were not well understood.7,8,18-20,22 In addition, the proportion of clinical alarms due to ventilator alarms ranged from 16% to 45% and is a significant segment of all clinical alarms (Table 6).3,7,10,11
Proportion of Alarms Caused by Ventilators in the Hospital Setting
Ventilator Alarm Prevalence Rates
The overall ventilator alarm prevalence rate measured in our study was 22.5 alarms per day of mechanical ventilation per patient. Our result was slightly higher than an earlier study in the PICU setting by Lawless, who reported 17.5 alarms per day of mechanical ventilation.7 The study by Lawless et al7 was one of the few studies of ventilator alarm rates in the PICU setting. More recently published studies in the PICU population were unavailable for comparison of ventilator alarm prevalence rates (Table 7 for comparison on ventilator alarm prevalence rates).
Rates of Ventilator Alarms in Adult, Pediatric, and Neonatal Populations
Earlier studies in the adult ICU population by Chambrin et al11 and Trojanowski et al25 also reported lower ventilator alarm prevalence rates of 14.8 and 16.2 ventilator alarms per ventilator day, respectively. However, a more recent adult ICU study by Cvach et al27 reported prevalence rates of 168 ventilator alarms per day of mechanical ventilation. Another recent study by Belteki et al28 in a neonatal ICU setting reported a significantly higher prevalence rate of 240 ventilator alarms per day of mechanical ventilation. The study by Belteki et al28 was performed with the Dräger Babylog VN500 ventilator, whereas the study by Cvach et al27 used the Hamilton G5 and PB840 ventilators.
The 10-fold increase in ventilator alarm prevalence rates reported in more recent studies may be related to differences in critical care ventilators, patient populations, or patient care settings. Newer ventilators are generally equipped with additional modes, complex algorithms, and capability to monitor additional parameters. Our own study identified a statistically significant (P < .001) difference in alarm proportions in different types of alarms when comparing the Servo-i and Avea ventilators between the PICU and CTICU (Table 5). For example, apnea alarms occurred at twice the rate in the PICU compared to the CTICU. This may have been due to the different underlying diseases in each ICU. Clearly, alarm prevalence rates varied between the different types of ventilators and care settings.
Medium- and High-Priority Alarms
The AARC consensus report classified common ventilator alarm conditions into Level 1 and Level 2 priority alarms using the AARC alarm priority criteria.16 Level 1 priority alarms are considered immediately life-threatening, such as apnea. Level 2 priority alarms are defined as potentially life-threatening events; immediate intervention recommended for both types of priority alarms.16 Ventilator manufacturers’ interpretation of the expert panel recommendations classified the ventilator alarms as high-priority or medium-priority alarms for the Servo-i and Avea ventilators.
Our results indicate that the Avea ventilator had a greater proportion of high priority alarms (84%), whereas the Servo-i exhibited more medium-priority alarms (69%). In contrast, the study by Cvach et al27 reported that 90% of alarms from the Hamilton G5 were high-priority alarms, compared with 9% from the PB840 ventilators. It is clear that manufacturers’ interpretations of alarm priority vary. In our comparison of the Avea and Servo-i manufacturer alarm priority (Table 2), a disagreement was found on alarm classifications for PEEP and High  . There was agreement, however, with Apnea, High Paw, Respiratory Rate, and Low
. There was agreement, however, with Apnea, High Paw, Respiratory Rate, and Low  alarms. The disagreement in alarm priority classification between manufacturers accounted for some of the differences in alarm priority proportions between these 2 ventilators. Alarm priority ratings require further standardization to improve agreement and consistency between manufacturers.
alarms. The disagreement in alarm priority classification between manufacturers accounted for some of the differences in alarm priority proportions between these 2 ventilators. Alarm priority ratings require further standardization to improve agreement and consistency between manufacturers.
Manufacturer Preset Algorithms
Our study identified 2 proprietary manufacturer alarms, the Inspiratory Flow Overrange alarm (42%) on the Servo-i and the Circuit Integrity alarm (20%) on the Avea, as 2 of the most common alarms based on the type of ventilator. These alarms were preset according to manufacturer algorithms. The high proportions of these alarms suggests that preset algorithms may not be ideal for all pediatric conditions. Flow and volume demands can vary widely in the pediatric population based on patient size and disease state. The condition of uncuffed endotracheal tubes, airway leaks, smaller tidal volumes, use of external flow sensors, and interactions with humidity and circuit rainout add to the challenges in ventilator alarm management in the pediatric patient. Alarm algorithms designed by ventilator manufacturers vary between the adult, pediatric, and neonatal modes and between types of ventilator. The high proportion of Inspiratory Flow Overrange and Circuit Integrity alarms suggests that additional capabilities for alarm customization are needed to optimize alarm parameters and reduce the overall alarm prevalence.
Most Prevalent Ventilator Alarms
In our study, the Inspiratory Flow Overrange (42%), high awRR (18%), and High Paw (17%) alarms were the most prevalent type of alarms. These findings were consistent with some of the findings reported by Tan et al26 and by Cvach et al.27 Tan et al26 reported high Paw, high breathing frequency, high VT, high  , and low Paw to be some of the most common alarms in adult ICUs. Cvach et al27 also studied the frequency of ventilator alarms extensively in an adult intensive care setting and reported the proportion of ventilator alarms to be greatest with the high peak inspiratory pressure (34%), high breathing frequency (18%), and low VT (13%).
, and low Paw to be some of the most common alarms in adult ICUs. Cvach et al27 also studied the frequency of ventilator alarms extensively in an adult intensive care setting and reported the proportion of ventilator alarms to be greatest with the high peak inspiratory pressure (34%), high breathing frequency (18%), and low VT (13%).
No pediatric studies were found for comparison of ventilator alarm proportions; however, in a neonatal ICU study, Belteki et al28 reported variations in breathing frequency and  as the primary determinants for ventilator alarm activation. The studies by Tan et al26 and Cvach et al27 indicated that high Paw and high breathing frequency alarms were some of the most common causes for ventilator alarms in the adult population. These findings were consistent with our results for High awRR and High Paw alarms, which were identified as 2 of the 3 most common causes for ventilator alarms. The Inspiratory Flow Overrange alarm, specific to the Servo-i, was difficult to compare to other studies as no other Servo-i alarm data were reported.
as the primary determinants for ventilator alarm activation. The studies by Tan et al26 and Cvach et al27 indicated that high Paw and high breathing frequency alarms were some of the most common causes for ventilator alarms in the adult population. These findings were consistent with our results for High awRR and High Paw alarms, which were identified as 2 of the 3 most common causes for ventilator alarms. The Inspiratory Flow Overrange alarm, specific to the Servo-i, was difficult to compare to other studies as no other Servo-i alarm data were reported.
Strategic Reduction of Ventilator Alarms
A systematic analysis of ventilator alarm data is an important first step in a logical and strategic approach to ventilator alarm reduction. This comprehensive method quantifies and helps prioritize the most prevalent types of alarms specific for each ventilator. A secondary step is to evaluate the institutional policy and consider whether guidelines for ventilator alarm management provide adequate guidance for all common alarms. A standard policy is necessary for consistent practice and could have a meaningful impact in reducing alarm prevalence. However, in a systematic review of issues related to ventilator alarms and alarm fatigue, Scott et al17 found no published standard guideline for clinicians and institutions to follow when setting ventilator alarm parameters.
Very little data are available to guide best practices for setting ventilator alarm limits. Furthermore, the lack of information on alarm management practices and outcomes makes comparisons with other institutions difficult. This necessitates internal benchmarking of baseline alarm prevalence rates followed by methodical policy changes to reduce alarms and efforts to compare resulting changes to previous alarm prevalence rates. This systematic method for benchmarking and analysis of alarm prevalence rates will bring the profession closer to a logical, evidence-based approach to setting ventilator alarms (Table 8).29,30
Ventilator Alarms Description
The high prevalence measured with some alarms suggested room to customize alarm parameters selectively based on the type of alarm priority and redundancy. Trojanowski et al25 reported that adding an alarm delay of 5 s could reduce the overall ventilator alarm prevalence by 64%. In our study, the top 5 alarms accounted for > 85% of all alarms generated; therefore, a focused approach with the top 5 alarms may have a significant impact. Lastly, educating end users to alarm algorithms inherent to each alarm is essential. The most common alarm found in our study, the Inspiratory Flow Overrange alarm, was not directly set by the practitioner. A greater understanding of the underlying relationships, such as manufacturer-designed flow limitations programmed for each mode of ventilation, is essential to reducing the conditions activating this alarm.
Limitations
Currently, there is no standardized metric or method for reporting ventilator alarm rates. The reported rates in our study (Table 3) were converted to the number of ventilator alarms per ventilator day per patient to facilitate comparisons in prevalence rates. Some studies excluded their number of ventilator days or other types of ventilator alarms in which only high-priority alarms were reported.2,23 This made it difficult to standardize the ventilator alarm prevalence rate for comparison with other research findings. In addition, the ventilator manufacturer and model were often not reported, which made ventilator-specific comparisons difficult to perform.
An additional challenge in ventilator alarm comparisons was the use of ventilator alarm terminology specific to the manufacturer’s preference. The varied names for similar alarm conditions made comparisons more difficult. Attempts were made maintain the manufacturer’s preferred terms for consistency. The unique ventilator alarms of the Avea device (ie, Circuit Integrity alarm) and the Servo-i ventilator (ie, Inspiratory Flow Overrange alarm) added another level of difficulty to our comparisons.
A clear methodology for comparison and benchmarking of ventilator alarm rates requires that all of the different types of alarms are captured and considered in the context of the total duration of mechanical ventilation for the time period being compared. The method applied in this study captured the diverse type of alarms prevalent in the PICU and CTICU in addition to the total days of mechanical ventilation. However, we could not gather alarm data from specialized ventilators such as the Sensormedics 3100a and 3100b, as well as home mechanical ventilators, due to software and hardware connectivity issues.
The collection of a large sample size is difficult due to limitations in the information technology and connectivity infrastructure. The automated process for electronically collecting ventilator alarm characteristics allows for the detailed examination of large data, which provides a comprehensive portrayal of ventilator alarm patterns in the clinical setting.
Generalization with this study is limited. First, the data studied were limited to the type of medical devices and monitors available at Children’s Hospital Los Angeles. Second, this study looked at only 2 types of ventilators. There are many other types of pediatric ventilators used throughout other ICUs. An observational study specific to each type of ventilator is needed to fully account for the variations in ventilator algorithms. Third, the detailed ventilator days attributed to each type of ventilator model were not collected for this study. This limits the ability to compare alarm prevalence rates specific to each type of ventilator. Additionally, ventilator alarm data collection was limited by the middleware system. Some alarms such as the high and low  on the Servo-i were bundled together due to system programming design. Lastly, the prevalence of ventilator alarms needs to be considered in the context of institutional alarm management practices.
on the Servo-i were bundled together due to system programming design. Lastly, the prevalence of ventilator alarms needs to be considered in the context of institutional alarm management practices.
Conclusions
The lack of ventilator alarms research in the pediatric population makes it compelling to do research for this vulnerable population. Studying the type and prevalence of ventilator alarms within the context of alarm management policies and guidelines in the clinical setting will help direct the professional community toward an evidence-based approach to alarm management.
Ventilators are designed to have their own unique alarm pattern and algorithms that impact alarm frequency and proportionality. Ventilator alarms occurred in the PICU and CTICU in a large metropolitan children’s hospital at an average combined prevalence rate of 22.52 ventilator alarms per day of mechanical ventilation per patient. Overall, the most common ventilator alarms were the Inspiratory Flow Overrange (37%), High awRR (18%), and High Paw (15%). Alarm characteristics vary with different ventilators. Ventilator alarm proportions also varied significantly between the PICU and the CTICU. Ventilator alarm proportions were significantly different between the Avea and Servo-i ventilators. Lastly, classification of high- and medium-priority alarms varies between ventilator manufacturers.
More studies are needed to observe the behavior of each type of ventilator within different patient populations, disease states, alarm parameter guidelines, and hospital settings. Lastly, connecting the alarms to physiological responses, patient interventions and outcomes can help the medical community identify the most important alarms, and which might play a secondary role. Ventilator manufacturers can design more effective and meaningful alarm systems with this new information.
Footnotes
- Correspondence: Leo Langga RRT RRT-NPS MBA DrPH. E-mail: leolangga{at}gmail.com
See the Related Editorial on Page 699
Dr Langga presented a version of this paper at AARC Congress 2019, held November 9–12, 2019, in New Orleans, Louisiana.
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}