

Abstract
BACKGROUND: This systematic literature review summarizes the impact of smoking on maximal oxygen uptake (maximum  ).
).
METHODS: Full-text articles were retrieved if the abstract met the assigned criteria. A total of 9 articles were included in the final review based on the inclusion and exclusion criteria. These included articles assessed the effects of tobacco smoking on maximum  values.
values.
RESULTS: Half of the articles reported a significant difference in maximum  scores between smokers and nonsmokers, with smokers having a lower maximum
scores between smokers and nonsmokers, with smokers having a lower maximum  . The other half of the articles did not identify significant differences between smokers and nonsmokers. One study found a significant difference in maximum
. The other half of the articles did not identify significant differences between smokers and nonsmokers. One study found a significant difference in maximum  in only one age group (ie, 20–29 y), but not any of the other age groups.
in only one age group (ie, 20–29 y), but not any of the other age groups.
CONCLUSIONS: More research is needed on the effects of smoking on maximum  to better understand any relationships or causations.
to better understand any relationships or causations.
- maximum ˙VO2
- maximal oxygen uptake
- aerobic capacity
- maximum ˙VO2 test
- cigarette smoking
- smoking
- smokers
- cigarettes
- tobacco cigarettes
Introduction
Traditional tobacco cigarettes are known to have detrimental health effects, yet the addictiveness of tobacco leads to continued use. In general, smoking continues to be a major public health issue and a preventable form of death and disability. It is estimated that 1.1 billion individuals worldwide smoke traditional cigarettes.1 One in 5 Americans die each year due to a tobacco-related illness.2 Cigarette smoking negatively impacts almost every organ system in the body. Diseases resulting from tobacco smoking include, but are not limited to, COPD, heart disease, premature birth, decreased fertility, type 2 diabetes, lower bone density, cataracts, and premature aging of the skin.2 Initial physiological changes related to tobacco smoke are found in the respiratory tract, our innate immune system and primary defense against respirable pathogens.3
Smoking increases risks for respiratory infections, worsens asthma, and can lead to COPD and cancers.2,4 Smoking accounts for 80–90% of all lung cancer deaths.5 Cigarettes contain approximately 69 chemicals that are known to be toxic and carcinogenic.6 When cigarettes are burned, the smoke produces > 7,000 chemicals.6 These toxic chemical compounds increase a smoker's risk of respiratory compromise and related diseases. The impact smoking has on the lungs brings into question how smoking affects physical activity and exercise in those individuals who smoke and exercise.
Evaluation of lung function is common in smokers and can be determined with spirometry. FEV1 as compared to FVC is a common measure to assess obstructive lung disease, commonly seen in smokers. Decreased FEV1/FVC values have been observed in young smokers, indicating early negative respiratory health changes.4,7 Several negative physiological effects occur in the lungs due to tobacco smoking. Airways in the lungs become narrow due to swelling and increased mucus production. Buildup of poisonous substances decreases the lungs clearance system. The alveoli in the lungs are permanently damaged, which inhibits gas exchange. Inhaled carbon monoxide from tobacco cigarettes binds to red blood cells and displaces oxygen, thus reducing the delivery of oxygen to the lungs, muscles, and other tissues. A decrease in oxygen will negatively impact endurance performance and lower the maximum  score.
score.
Many adults, regardless of athletic ability, exercise as a form of stress relief and relaxation.8 However, understanding the changes in lung function among smokers who are striving to become healthier by exercising is important. Smoking negatively affects these individuals respiratory function.9,10 It is known that individuals who smoke and engage in physical activity do not perform as well as nonsmokers.11 By comparing smokers and nonsmokers, the maximum  scores would show whether smoking has negatively impacted performance during exercise due to decreased lung function. The aim of this study was to systematically review the literature for studies that have assessed traditional cigarette smoking impact on maximum
scores would show whether smoking has negatively impacted performance during exercise due to decreased lung function. The aim of this study was to systematically review the literature for studies that have assessed traditional cigarette smoking impact on maximum  , a measure of the maximum amount of oxygen a person can utilize during exercise. Current research has not systematically reviewed the effects of smoking on maximum
, a measure of the maximum amount of oxygen a person can utilize during exercise. Current research has not systematically reviewed the effects of smoking on maximum  scores. In essence, maximum
scores. In essence, maximum  serves as a measure of cardiorespiratory efficiency.
serves as a measure of cardiorespiratory efficiency.
Methods
A systematic review of the literature was conducted in April 2020 by 2 researchers. The researchers categorized and located studies related to the effects of cigarette smoking on maximum  and cardiorespiratory efficiency. Databases included in the search were PubMed, Academic Search Complete, Google Scholar, NCBI, Science Direct, and ProQuest. The exercise search terms were [maximum
and cardiorespiratory efficiency. Databases included in the search were PubMed, Academic Search Complete, Google Scholar, NCBI, Science Direct, and ProQuest. The exercise search terms were [maximum  ], [maximum oxygen uptake], [aerobic capacity], and [maximum
], [maximum oxygen uptake], [aerobic capacity], and [maximum  test] combined with “or.” Population terms included [cigarette smoking], [smoking], [smokers], [cigarettes], and [tobacco cigarettes] combined with “or.” Intervention and population terms were also combined with “and” and searched in “All Fields” with the limits of the English language.
test] combined with “or.” Population terms included [cigarette smoking], [smoking], [smokers], [cigarettes], and [tobacco cigarettes] combined with “or.” Intervention and population terms were also combined with “and” and searched in “All Fields” with the limits of the English language.
Inclusion criteria included smoking/nonsmoking comparison studies that conducted a maximum  test to measure cigarette smoking effects on subjects' maximum
test to measure cigarette smoking effects on subjects' maximum  and cardiorespiratory efficiency. The study design of the research articles could be observational studies, randomized controlled trials, or experimental studies. Only full-text articles published in peer-reviewed journals were included. Only studies in English or translated into English were included. No exclusions were made for gender or ethnicity. No exclusions were made for subjects' physical activity level. Exclusion criteria included studies in which subjects reported preexisting or underlying health conditions and studies involving e-cigarette and marijuana.
and cardiorespiratory efficiency. The study design of the research articles could be observational studies, randomized controlled trials, or experimental studies. Only full-text articles published in peer-reviewed journals were included. Only studies in English or translated into English were included. No exclusions were made for gender or ethnicity. No exclusions were made for subjects' physical activity level. Exclusion criteria included studies in which subjects reported preexisting or underlying health conditions and studies involving e-cigarette and marijuana.
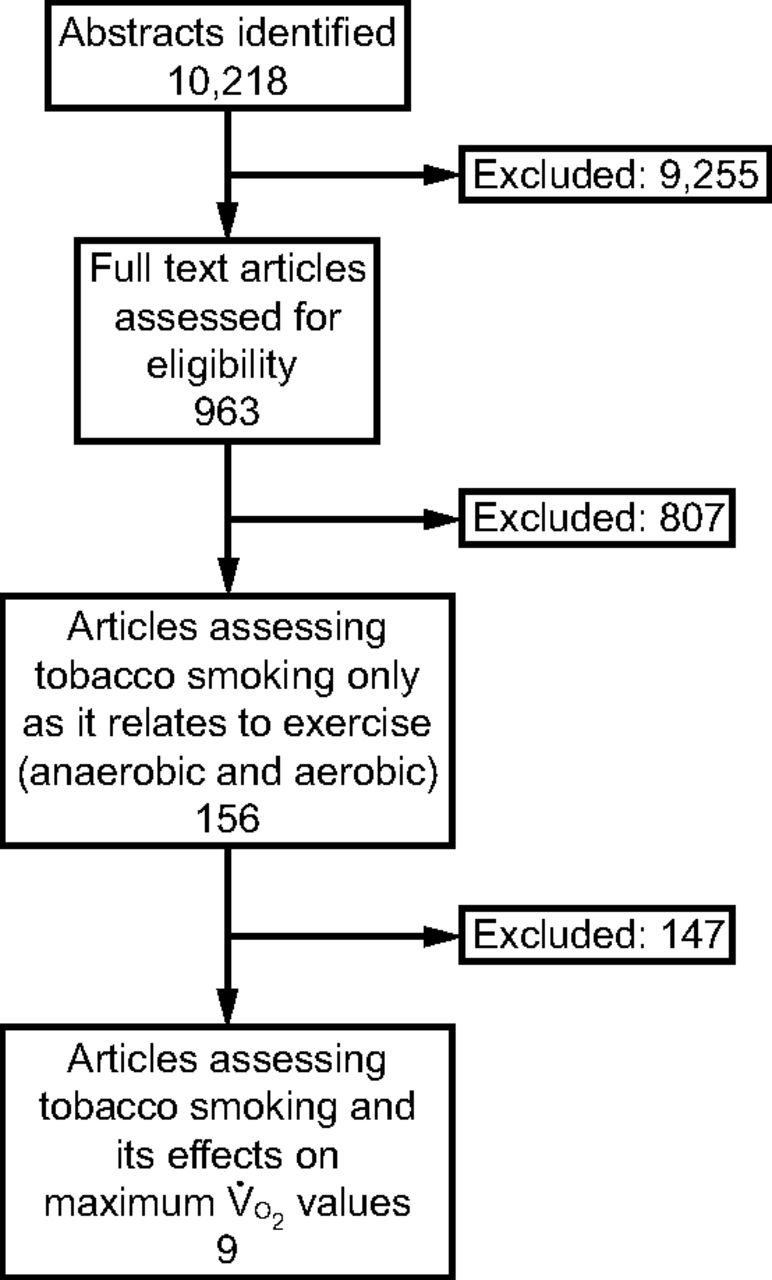
The initial search generated a total of 10,218 eligible studies. After a review of the titles and abstracts, only 963 studies were relevant for this review. Studies were excluded if they did not include humans, were systematic reviews or meta-analyses, had an inappropriate study design, or did not look at the specific desired population. After independently reviewing the 963 results, articles looking at other forms of smoking besides traditional cigarettes were excluded, as well as any articles not relating to exercise. This further narrowed the results to 156 studies. Out of these 156 studies, those that included anaerobic exercise were eliminated, as were any studies that did not conduct a full maximum  test with subsequent results. A total of 9 studies evaluating maximum
test with subsequent results. A total of 9 studies evaluating maximum  in cigarette smokers met the criteria to be included. Figure 1 displays the results of the search process; Table 1 shows a summary of the study characteristics and outcomes.
in cigarette smokers met the criteria to be included. Figure 1 displays the results of the search process; Table 1 shows a summary of the study characteristics and outcomes.

Flow chart.
Study Characteristics and Outcomes
Results
A total of 3,326 people participated in the 9 studies included in this systematic review. Of those subjects, 63.9% were classified as smokers while 36.1% were classified as nonsmokers. Two of the 9 studies did not specify the number of smokers and nonsmokers tested.14,18 Two studies divided smoking subjects into moderate and heavy smoker groups.12,13 One study divided the smoking subjects into light, moderate, and heavy smoking groups.14
The study conducted at the NASA Johnson Space Center in Houston, Texas, had the largest subject pool (N = 2,749).14 The average number of subjects in the remaining studies was 72. The age of subjects ranged from 18 y to 59 y. Two studies did not specify subject age.15,16 Regarding gender, 5 of the 9 studies used only male subjects, averaging 40 males per study.13,15–18 The study conducted at NASA Johnson Space Center included both male and female subjects, with 86.4% of the subjects being male.14 The remaining 3 studies did not specify subject gender.8,13,14
Each study contained a control group of nonsmokers. All subjects participated voluntarily. Each study's criteria for a nonsmoker was a self-report of never smoking. None of the control subjects had any reported health issues. One study matched smokers and nonsmokers.19 Seven studies stated the number of subjects in the control group.8,9,11–15 The smallest number of subjects in a control group was 9, while the largest number of subjects in a control group was 92.15,20 Two studies did not state the specific number of subjects in the control group.14,16
Four of the 9 studies reported a statistically significant difference in maximum  between smokers and nonsmokers.12–14,16 Two studies stated that there was an overall decline in maximum
between smokers and nonsmokers.12–14,16 Two studies stated that there was an overall decline in maximum  from nonsmokers to heavy smokers.13,14 In the study by Suminski et al,14 the reduction in maximum
from nonsmokers to heavy smokers.13,14 In the study by Suminski et al,14 the reduction in maximum  between nonsmokers and heavy smokers was 6.2 mL/kg/min. There was also a statistically significant difference between active smokers and nonsmokers in the study by de Borba et al.12 Namrata et al18 reported a significant difference between light smokers and nonsmokers.
between nonsmokers and heavy smokers was 6.2 mL/kg/min. There was also a statistically significant difference between active smokers and nonsmokers in the study by de Borba et al.12 Namrata et al18 reported a significant difference between light smokers and nonsmokers.
All studies assessed statistical significance as occurring at P ≤ .05 or less. Four studies did not report a significant difference in maximum  between smokers and nonsmokers. Song et al17 did not report a significant difference. The maximum
between smokers and nonsmokers. Song et al17 did not report a significant difference. The maximum  of smokers was 53.38 mL/kg/min, while the nonsmokers had a maximum
of smokers was 53.38 mL/kg/min, while the nonsmokers had a maximum  of 54.42 mL/kg/min. There was also no statistically significant difference between the controls and smokers in the study by Pakkala et al.19 Nonsmokers averaged a lower maximum
of 54.42 mL/kg/min. There was also no statistically significant difference between the controls and smokers in the study by Pakkala et al.19 Nonsmokers averaged a lower maximum  of 41.01 mL/kg/min than smokers which averaged 42.25 mL/kg/min. Gur et al16 reported no significant difference between smokers and nonsmokers, with a very small difference of 0.5 mL/kg/min in the average maximum
of 41.01 mL/kg/min than smokers which averaged 42.25 mL/kg/min. Gur et al16 reported no significant difference between smokers and nonsmokers, with a very small difference of 0.5 mL/kg/min in the average maximum  . Smokers averaged a maximum
. Smokers averaged a maximum  of 38.1 mL/kg/min, whereas nonsmokers averaged 38.6 mL/kg/min. Kobayashi et al15 reported that nonsmokers had higher fitness levels with lower heart rates and percent body fat and higher maximum
of 38.1 mL/kg/min, whereas nonsmokers averaged 38.6 mL/kg/min. Kobayashi et al15 reported that nonsmokers had higher fitness levels with lower heart rates and percent body fat and higher maximum  values, although this difference was not statistically significant between groups.
values, although this difference was not statistically significant between groups.
Four of the studies reported a statistically significant difference between smokers and nonsmokers of all ages,12–14,18 whereas 4 studies noted no difference between smokers and nonsmokers.15–17,19 Chatterjee et al,20 in the only study to stratify subjects by age, reported a statistically significant difference in maximum  between nonsmokers and smokers, but only in subjects 20–29 y old. In the 30–39, 40–49, and 50–59 y age groups, nonsmokers had higher maximum
between nonsmokers and smokers, but only in subjects 20–29 y old. In the 30–39, 40–49, and 50–59 y age groups, nonsmokers had higher maximum  scores, but the differences were not statistically significant between smokers and nonsmokers. For individuals > 30 y old, the maximum
scores, but the differences were not statistically significant between smokers and nonsmokers. For individuals > 30 y old, the maximum  for nonsmokers was lower than for smokers, but the difference was not statistically significant.
for nonsmokers was lower than for smokers, but the difference was not statistically significant.
Three studies used bicycle ergometers to perform their maximum  protocol.13,16,20 Each bicycle protocol required subjects to ride until exhaustion. Two protocols increased workload every 3 min, while the third protocol led to total exhaustion within 4 min for every subject. The remaining 6 studies used a treadmill to perform the maximum
protocol.13,16,20 Each bicycle protocol required subjects to ride until exhaustion. Two protocols increased workload every 3 min, while the third protocol led to total exhaustion within 4 min for every subject. The remaining 6 studies used a treadmill to perform the maximum  test.12,14,15,17–19
test.12,14,15,17–19
Of these 6 treadmill protocol studies, 2 specified that the Bruce protocol was used.12,17 One study performed a Balke treadmill test, while another used the Astrand nomogram method.19 Two studies used their own treadmill protocols.15,17 Each study that performed a maximum  test on a treadmill determined that the maximum
test on a treadmill determined that the maximum  was the highest
was the highest  value in the last minute prior to subject exertion and test termination. Each subject had to obtain a respiratory exchange ratio value of ≥ 1.1 to determine the maximum
value in the last minute prior to subject exertion and test termination. Each subject had to obtain a respiratory exchange ratio value of ≥ 1.1 to determine the maximum  . Every study utilized in this systematic review described the specific maximum
. Every study utilized in this systematic review described the specific maximum  protocol that they used.
protocol that they used.
Discussion
This study sought to systematically review the literature for studies that assessed maximum  in individuals who self-reported that they were smokers. The act of cigarette smoking most significantly affects the respiratory system.7,9 This is due to nicotine impairing ventilatory function and constricting ventilatory pathways and blood vessels.17 Airway obstruction as well as inflammatory changes in the lungs affect their function, which is often an indicator of all-cause morbidity and mortalilty.7 The maximum
in individuals who self-reported that they were smokers. The act of cigarette smoking most significantly affects the respiratory system.7,9 This is due to nicotine impairing ventilatory function and constricting ventilatory pathways and blood vessels.17 Airway obstruction as well as inflammatory changes in the lungs affect their function, which is often an indicator of all-cause morbidity and mortalilty.7 The maximum  test is an assessment of lung function that measures functional capacity of the oxygen transportation in the body.13 Exercise tolerance testing helps clinicians establish relationships between cardiorespiratory fitness, cardiovascular disease, and all-cause mortality.
test is an assessment of lung function that measures functional capacity of the oxygen transportation in the body.13 Exercise tolerance testing helps clinicians establish relationships between cardiorespiratory fitness, cardiovascular disease, and all-cause mortality.
This form of physical activity may be difficult for smokers impairment of respiratory function due to cigarette smoking.9 Physical activity positively changes adipose tissue profiles, which reduces obesity and enhances ventilatory muscle function.7 Previous studies have indicated that muscle tissue differences may occur between smokers and nonsmokers. Another difference between groups may be a decrease in the oxygen transporting capacity to the mitochondria in the muscle due to the action of carbon monoxide.13
In the future, more studies should focus on the number of cigarettes smoked each day, the length of smoking history, age, and gender on the impact of maximum  . By analyzing more specific variables related to smoking and the subject demographics, the results may be unanimously conclusive.
. By analyzing more specific variables related to smoking and the subject demographics, the results may be unanimously conclusive.
One limitation of this study is that both acute and chronic smoking was assessed. Due to the limited number of published studies on maximum  and smoking, all lengths of smoking history were included in this review. Another limitation of this review is that not all studies stratified subjects by age and gender. Age can have an impact on length of smoking history, which may affect the amount of lung damage done.
and smoking, all lengths of smoking history were included in this review. Another limitation of this review is that not all studies stratified subjects by age and gender. Age can have an impact on length of smoking history, which may affect the amount of lung damage done.
Conclusions
The variable results of this systematic review may be due to the variety of subject characteristics captured in the studies, such as differences in the quantity of cigarettes smoked each day, length of smoking history, age, and gender.12,13,15 Physical activity can impact a  score, thus making it a factor that needs to be considered in the future.
score, thus making it a factor that needs to be considered in the future.
The 9 studies in this review evaluated the impact of smoking on maximum  . This focus does not minimize the dozens of other negative effects that smoking can have on an individual. Developing a lung disease such as COPD, pneumonia, or even lung cancer from smoking will eventually negatively impact an individual's maximum
. This focus does not minimize the dozens of other negative effects that smoking can have on an individual. Developing a lung disease such as COPD, pneumonia, or even lung cancer from smoking will eventually negatively impact an individual's maximum  . Only 2 studies specified that the subjects were sedentary.12,13 One study noted that subjects engaged in regular physical activity.15 Three studies did not find statistically significant differences between groups.
. Only 2 studies specified that the subjects were sedentary.12,13 One study noted that subjects engaged in regular physical activity.15 Three studies did not find statistically significant differences between groups.
Footnotes
- Correspondence: Nauris Tamulevicius PhD, Department of Health Sciences and Human Performance, University of Tampa, 401 W Kennedy Blvd, Tampa, Florida 33606. E-mail: ntamulevicius{at}ut.edu
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}