

Abstract
The word “quality” refers to the features of a product or service to which a certain value is ascribed. When it comes to hospital-based practices, quality has often been considered to be specific to the care provided. However, this specific perspective is transitioning toward a broader concept after the evolution of quality-improvement projects and quality frameworks at the organizational level. Respiratory therapy departments have been identified as an essential part of any hospital because the key nature of discipline for respiratory therapists is widely understood. Due to their professional accountability and professional values, respiratory therapists often have administrative roles in infection control practices and quality-improvement projects. Therefore, it would be ideal to have a core team of respiratory therapists trained in quality management and to initiate quality-improvement processes at the departmental level. Every respiratory therapy department should have its own quality-improvement team to assist with the process of training, implementation, and analysis. Thus, this article aimed to discuss the role of respiratory therapists and respiratory therapy departments in quality-improvement processes and projects to set benchmarks and enhance outcomes.
- quality
- continuous quality improvement
- respiratory therapy departments
- respiratory therapists
- healthcare
Introduction
The term “quality” is an essential component of current hospital and health-care policies because it primarily reflects the desired patient outcomes. The integration of quality in health care is part of the transformation of health-care systems in diverse organizational structures.1 There are 2 well-accepted definitions that describe quality in health care. The first was put forward by the National Academy of Medicine (previously known as the Institute of Medicine of the National Academy of Sciences), which defined quality health care as “safe, effective, patient-centered, timely, efficient, and equitable.”2 Meanwhile, the second definition was given by the Agency for Healthcare Research and Quality, which defined health-care quality “as doing the right thing for the right patient, at the right time, in the right way to achieve the best possible results.”3
Accurate, appropriate, and continuous assessment of quality is the key to efficient care being provided by health-care professionals.4,5 A number of reports in the literature have strengthened the importance of quality in health care from organizational and departmental perspectives6-8 as well as from physicians’ and nurses’ perspectives.9-12 However, there is a paucity of literature specific to allied health-care professions that describe the importance of quality-improvement processes and the need for quality indicators, with a few emphasizing its relevance.13,14 Allied health care is an umbrella term that includes a wide variety of health disciplines and ancillary services, and its professional classification is based on specific disciplines or areas of practice that vary among countries, government bodies, industry, health-care settings, and training institutions.13
Respiratory therapists (RTs) are allied health-care professionals who specialize in cardiopulmonary sciences. They provide a wide range of diagnostic and therapeutic interventions to patients who require cardiopulmonary and related services.15 They are vital in acute care settings, emergency departments, wards, out-patient departments, pulmonary diagnostics and rehabilitation, and sleep medicine departments.16 Furthermore, they are considered to be advantageous for improving patient outcomes by reducing mortality and morbidity.17-19 Respiratory therapy departments are an integral part of many hospitals and health-care settings throughout the world. Administratively, some of them work closely with medical departments, for example, critical care and pulmonology departments. In some countries, the respiratory therapy profession is well organized, with accredited respiratory therapy training programs and heavily supervised robust credentialing and professional development processes.16,20
Providing high-quality patient care in a safe environment has been the prime focus of all hospitals and health-care settings.21 Due to the nature of the work of RTs, and the fact that they practice in multi-disciplinary areas, which range from neonatal ICUs to chronic care and rehabilitation centers, they are expected to be the advocates of quality in health care. Thus, in this article, we review some of the processes that respiratory therapy departments can adopt and adapt to facilitate quality at the departmental level.
The “Value” of Respiratory Therapy in Health-Care Systems
The health-care profession is rapidly moving forward with increasingly focused care owing to various advances in diagnostic and therapeutic interventions. This is particularly evident in terms of providing care to patients who are critically ill and with diverse cardiorespiratory disorders in which RTs hold a key position in patient management.19 Implementation and continuation of respiratory therapy services in a secondary or tertiary care health-care center is resource intensive. Respiratory therapy departments have to prove their value through affordable care and departmental performance. Such objectives directed the American Association for Respiratory Care22 to issue guidelines as to how this can be achieved in respiratory therapy departments.
Value in health care is described as measurable improvement in the patient’s health condition against the cost of attaining that improvement.23 Value-based care transformation aims to facilitate health-care systems to be more patient-centric. Quality and value are interrelated in health-care settings based on various inputs for improvement and the compliance to these processes.24 However, it is known that health-care systems may not always provide high-quality, highly reliable, evidence-based care that leads to desired outcomes.25 It is understood that value is not always easy to demonstrate in highly complicated and complex places, for example, health-care settings.26
Planning and implementation of a robust quality-management system in respiratory therapy departments suggest that the department is providing value. Quality-management services ensure that there is a defined and documented quality and safety policy, along with SMART (specific, measurable, attainable, relevant, and time bound) quality and safety goals, objectives, values, and service standards.27 It is the duty of the senior management to ensure that these aspects are planned, implemented, and actually achieved. However, this may be easier said than done. Based on what Deming28 put forward as the system of profound knowledge, improving quality in health-care needs the following 4 elements: (1) appreciation for a system, (2) knowledge about variation, (3) theory of knowledge, and (4) knowledge of psychology. The U.S. Department of Health and Human Services Health Resources and Services Administration29 suggests that all health-care organizations can improve their quality and thereby the value of their delivery by regularly evaluating their structure and process by using the data for benchmarking and by evaluating the patients and the team work involved.
Methods to Reflect the Value of Respiratory Therapy
Two well-known methods have been made available to assess the value of respiratory therapy in health care: (1) performance evaluation and improvement, and (2) continuous quality improvement (CQI). Performance evaluation is based on continuous monitoring and reporting of accomplishments, particularly with progressing toward pre-established goals. This enhances the probability of achieving the desired patient and organizational outcomes. CQI has been identified as a key component of total quality management that uses rigorous, systematic, organization-wide processes to achieve ongoing improvement in the quality of health-care services and operations. The scope of quality improvement is growing in health care and significantly depends on key structure, process, and outcome measures.30
Batalden and Davidoff31 defined quality improvement in health care as “combined and unceasing efforts of everyone — healthcare professionals, patients and their families, researchers, payers, planners and educators — to make the changes that will lead to better patient outcomes (health), better system performance (care) and better professional development.” Hence, it is understood as a process-based, data-driven approach to improve the quality of health-care delivery.
Performance evaluation and improvement is focused more on effectiveness and efficiency, whereas quality improvement is focused more on safety, equitability, timeliness, and patient orientation. Despite the differences in these approaches, they both rely on the following processes30: (1) defining the aspects of quality to be delivered, (2) monitoring the quality that is actually delivered, (3) identifying the gaps between planned and actual delivery, (4) discovering the reasons for the existence of the gaps, and (5) improving the structure and process to close the gaps.
Quality Management in Respiratory Therapy
Quality management in health care has a comprehensive definition. Previously, it was defined as the completion of tasks by the assigned health-care professionals, but, now, its definition has evolved to include the process of providing care.32 Any respiratory therapy department planning to continually improve its quality should have all the organized activities in place to plan, direct, coordinate, and control its quality-management system.30 Recruitment of RTs from the respiratory therapy department to function as a quality-improvement team marks the beginning of the process because the measurement of quality indicators strongly depends on the clinical frontline staff.33 Their commitment is associated with the success of the quality-improvement projects and improved patient outcomes.33,34 RTs, as allied health professionals, should also consider quality-assurance training as a priority for safe and efficient patient care.35 The necessary activities are listed in Table 1. Collecting, monitoring, and measuring data; analysis and review of data; and internal audits that produce conclusions are considered to be a continuous process. This enables management to review and take corrective or preventive actions to improve specific performance or to implement an effective novel method.
Components that Facilitate the Implementation of “Quality”
Implementation of CQI Programs in Respiratory Therapy Departments
Many quality-improvement models exist in hospitals to assess and improve the quality of care they provide (eg, Lean models, Six Sigma, total quality management, and plan-do-check-act cycle); however, none has been found superior to others in providing significant and sustained improvement in patient care outcomes. The “Donabedian model” of “structure, process, and outcome” is possibly one of the most notable conceptualizations of quality improvement.36 Avedis Donabedian, a physician and researcher, developed this model in 1966 and mentioned it in his milestone article entitled “Evaluating the quality of medical care.” He developed a triad of structure, process, and outcome for the evaluation of the quality of health care based on the concept of “input–process–output” used in industrial manufacturing. Donabedian’s framework of structure, process, and outcome evaluation was found to be a valuable and validated approach related to safety and quality outcomes in various areas of multidisciplinary care.37,38
The Donabedian triad can be applied to respiratory therapy departments as follows. The first aspect, structure, pertains to the characteristics of the resources in the health-care delivery system that relate to individual practitioners, groups of practitioners, and organizations and agencies. In terms of health-care professionals, this variable is inclusive of demographic factors (eg, age) and of professional specifications (eg, specialty, licensure, and certification).39 Structure focuses on size, location, governance, accreditation, and licensure status.
Structure also includes many physical elements, for example, special units and computer and/or network capabilities, and organizational factors (eg, the number of staff, staff-to-patient ratios, and employee turnover). For respiratory therapy departments, the structure includes departmental settings, the qualifications of RTs, the administrative systems through which care is provided, the recruitment process, and utilization of departmental and organizational resources. Once this information is compiled, a set of values about human and organizational performance is available for evaluation. The information can guide change and improvement efforts, such as, requesting additional information technology support or planning additional education for the staff. These variables need to be compared against relevant published local, regional, national, and international data.
The second element in the triad is process, which focuses on what is done to and for the patient. Process assessment is one of the most common methods of quality assessment and assurance, which can be achieved individually, by a group of professionals, or by the entire system of care. The process includes all aspects of the right care at the right time and addresses problems that occur during the delivery of care.39 Such steps include identification of a problem, precise definition of the problem, identification of all possible causes, assessment of root causes, and development of a solution.
The last domain of the triad is outcome. Outcome is the end results of care, that is, the health and well-being of the patients as an outcome of the care provided. Outcomes are usually based on the various units of measurement that are used, for example, death rates, nosocomial complication rates, functional capacities and performance, emotional balance, cognitive functioning, and of patient-related factors, for example, satisfaction, knowledge, and compliance.39 At the respiratory therapy department level, outcomes include patient-related factors (eg, recovery, restoration of function, and survival after various levels of care from RTs) and department-related factors (eg, RTs’ satisfaction levels, adherence to guidelines after departmental induction, and revenue generation). This domain involves implementation and monitoring of the effectiveness of the solution, which thus provides feedback for a continuous improvement loop.
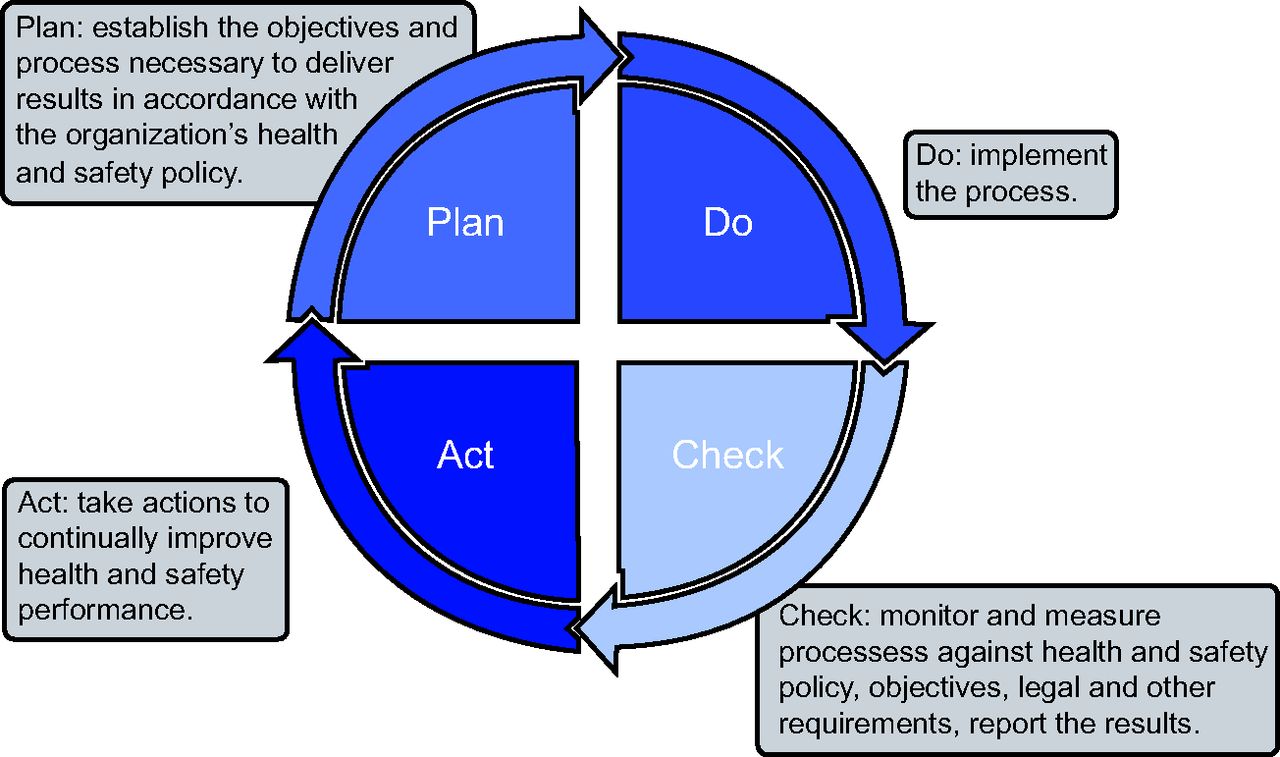
Another important framework used to analyze various approaches for quality improvement in health care is the plan-do-check-act cycle, sometimes known as the plan-do-study-act cycle.40 This is a 4-step model for bringing change. Every step in this method is important and dependent on other steps, which thus contributes to the success of the other steps. Therefore, these steps need to be taken collectively and not individually. Florence Nightingale aptly brought out the importance of each step in her famous quotation, “The ultimate goal is to manage quality. But you cannot manage it until you have a way to measure it, and you cannot measure it until you monitor it.”41 The processes of the plan-do-check-act cycle are shown in Figure 1.

The plan-do-check-act (PDCA) cycle for continuous quality improvement.
The Donabedian model, the plan-do-check-act cycle, and other frameworks related to quality improvement share complementary conceptual perspectives. Furthermore, a combination of these can provide a thorough and attainable basis for an effective quality strategy.40 The classic Donabedian model of “structure, process, and outcomes” remains a firm foundation for any quality-improvement program, followed by the plan-do-check-act framework, as an efficient tool to design, implement, and assess quality improvement in various intensive care settings.42,43 The same structure may be adopted in respiratory therapy departments as well.
CQI is neither a 1-step nor a 1-stop process, that is, it is continuous and progressive. Every step mentioned in the Donabedian model and the plan-do-check-act cycle is a discrete part of a quality-improvement project, and many such projects make up implemented CQI programs. To initiate a CQI program, respiratory therapy departments should begin with a single quality measure and then prepare a project and implement it. Table 2 enumerates the 10 steps adapted from the literature as a base for a CQI process framework in respiratory therapy departments.44,45
Ten Steps for the Continuous Quality Improvement Process in a Respiratory Therapy Department
The following goals of CQI are found to be ideal for respiratory therapy departments, as per the limited available literature:16 (1) provide a method for continuous monitoring of quality and relevance of respiratory care practices, (2) ensure that the respiratory care protocols and procedures are cost-effective, (3) ensure that the respiratory care protocols and procedures are effective in terms of clinical outcomes, and (4) recognize, prioritize, and resolve all the problems centered on patient care.
It is obvious from the above discussion that, to achieve or improve, the department must monitor and measure the structure, process, and outcomes before it proceeds further. Monitoring and measuring can be tedious processes without involvement by the bioinformatics department. A robust electronic medical or health record system that captures chronologically accurate, complete, and verifiable clinical data that can be integrated with a quality-monitoring system should be established. Although manual entry of such data is possible, it is prone to errors and thus not easily verifiable. Many quality monitoring tools are freely available and can be easily integrated into the monitoring process. Systems can be developed locally or can be adopted from vendors. Statistical process control allows the display of data that can be easily visualized and interpreted. Using the correct quality tools can help with the display of relevant data in a matrix that can be updated and compared with a benchmark. Any deviations can be highlighted and corrected.46 The following paragraphs describe these processes in detail.
Understanding Quality and Safety Indicators
A basic understanding of the characteristics of quality and safety indicators has been identified to be necessary for the quality-improvement team of the respiratory therapy department to determine what can be useful. There are various definitions and descriptions of “indicators” in health care. Clinical quality indicators are described as measurement tools or flags that are used to monitor, evaluate, and improve the quality of patient care, clinical support services, and organizational functions to improve patient outcomes.1,40,47 The essential characteristics of indicators that are related to respiratory therapy departments are presented in Table 3.
Characteristics and Description of Terminologies Related to Quality Indicators
Selection of Indicators for Respiratory Therapy Departments
Few indicators for respiratory therapy departments are currently available in the literature. Most of the quality indicators currently used globally in critical care settings have direct involvement of respiratory care practices and, hence, can be adopted for respiratory therapy departments after tailoring them appropriately to the practice.48-51 The respiratory therapy departments planning to embark on the process of establishing a departmental quality framework must search the literature from other related specialties to create suitable indicators, and, when doing so, it will be important to stick to the principles outlined in Table 3. Importance should be placed on choosing the initial indicators that are going to be measured. In particular, the quality or safety measure must be important, valid, reliable, responsive, interpretable, and feasible.52
The essential components of an ideal indicator are listed in Table 4, as suggested in “An Introduction to Indicators,” published by the Monitoring and Evaluation Division of United Nations Program on human immunodeficiency virus/acquired immune deficiency syndrome in 2010.53 It is possible that various indicators suitable for consideration by respiratory therapy departments may not be in broader use. However, indicator selection is an achievable task if based on the principles, as mentioned in Table 3 and 4.
The Essential Components of an Ideal Indicator
Suggested Indicators for Respiratory Therapy Departments
Some examples of the indicators that are suitable for respiratory therapy departments, as adopted and modified from the existing related literature, are illustrated in Table 5.48-51
Examples of Suggested Indicators for a Respiratory Therapy Department Based on the Donabedian Model
The Process of Implementing “Quality”
Once the respiratory therapy department chooses the group of indicators that are going to be monitored, a specific cycle is suggested to be performed as follows52:
Each indicator needs to be carefully constructed based on the characteristics described in Table 3. This is vital and, hence, must be precise. It is ideal that the staff members involved in any particular indicator are involved in this process.
It is preferable to involve the information technology department with collection and analysis of the data. Although it is possible to collect the data and analyze it manually, computerizing the process makes the job much easier.
The information technology department may be entrusted with the task of developing and using the correct templates for data collection. The quality-improvement team of the respiratory therapy department can then easily monitor and ensure verification of the methods of collection. The information technology department can integrate the software used in the following departments: registration, admission and discharge, billing, ICU, emergency, pulmonary function laboratory, medical records, and human resources.
The quality-improvement team in the respiratory therapy department must monitor the collection of data daily, weekly, monthly, or quarterly, as needed, to collate and review the data.
A core group of RTs trained in quality management should perform a system analysis when the values fall outside expected limits or beyond benchmarks, and the causes must be identified.
Benchmarking 2.0 software endorsed by the American Association for Respiratory Care (https://www.respiratorybenchmarking.org/default.aspx, Accessed July 27, 2021.) has been defined as a useful tool for system analysis.
The core group then drafts proposals for correction and preventive action; this draft is approved by the staff concerned with implementation and then is submitted and discussed by the quality committee.
The minutes of the meeting of the quality committee are shared with all the stakeholders, and an action plan is created for implementation.
The quality link in the respiratory therapy department follows up on the action plan implementation process and troubleshoots when needed.
The process of data monitoring, collection, and analysis is repeated per plan-do-check-act cycle.
The outcomes of these action plans, whether positive or negative, are shared with the quality committee and management for review and submission to the hospital board.
Difficulties in Implementing a CQI Program
Any CQI intervention based on quality- or safety-indicator monitoring must have clear-cut benefits for patients, be suited to local needs and budgetary provisions, and be supported by robust evidence. It must be understood that, although CQI projects may seem easy to perform, this is seldom the case. There may be multiple challenges related to the design and planning of improvement interventions, organizational perspectives, professional and leadership levels, sustainability and continuity beyond the initial interventional phase, and unintended outcomes.54 For these reasons, persistence, perseverance, and practice will significantly help any CQI program.
Effective leadership is the driving force for developing a quality-focused organizational culture and effective performance in health-care delivery.55 Respiratory therapy departments are often linked or interlinked with the medical direction. Thus, it may be difficult for the RT quality leader to independently modify the structure or ensure continued availability of a skilled workforce and/or add necessary technology in the department. Hence, RT leadership needs to champion the process and allocate the roles and resources. Although it may be easy to get the policies, protocols, and procedures put on paper, it may, in fact, be difficult to implement them on a day-to-day basis. Therefore, advice and support from the quality department of the organization is recommended. The leadership team and/or managers of respiratory therapy departments are the key to quality in the department, providing evidence-based inputs to establish professionalism, employee satisfaction, and better clinical and patient outcomes.56
Other key efforts are required to ensure provision of ongoing training to continuously update all staff on planned processes (particularly because processes are likely to be updated after CQI cycles to improve outcomes) and appropriate funding because budgetary provisions in respiratory therapy departments rarely include provisions for data collection or analysis for CQI. It should be remembered that a CQI program may be an emerging requirement of the respiratory therapy department team. For example, an ongoing accreditation process may require a CQI program. The problems related to quality and outcomes and to their solutions might seem simple and obvious. However, analysis of the problem may be based on little, subjective, evidence. Implementation might not be easy, and obstacles can occur at various levels. In addition, initiating a corrective action may itself lead to subsequent appreciation of new aspects to the previous problem.43
Once the best practice is identified, the quality-improvement teams may encounter resistance to implementation, which includes changes in routine practice and difficulty in acceptance. This can be addressed by awareness sessions, including classes, discussions, and posters that reflect the results of before and after phases of the project. Two challenges that are likely to be encountered by the quality-improvement teams include identification and implementation of best practices.57 Interventions that seem to be intuitively promising may not always lead to desired results. Even when they are beneficial, the resultant improvement in quality may be much smaller than anticipated and may have unintended consequences. Some consequences of CQI might include (1) unintended effects of changes in resource use, including increased cost and increased health disparities, (2) unintended effects on care provider behavior, and (3) unintended effects on patients.58
Although the basic science of CQI may seem to differ from the rest of medicine, this is not an accurate perception. CQI interventions need to undergo experimentation and phased evaluation trials similar to any other clinical intervention. If these phases are not done, then minimally effective or useless interventions may be pursued, scant resources may be squandered, and harmful results may be generated. Worse still, delusions with regard to the effectiveness of an intervention may result in its adoption by an increasing number of institutions.
This discussion of potential issues is not intended to dissuade RTs and respiratory therapy departments from implementing a CQI program, rather it aims to clearly explore the problems so that departments that implement the program will avoid common pitfalls. Even though our knowledge on the best practices in respiratory care remains incomplete, the quality-improvement teams are thought to have an important role in improving respiratory care plans and practices.57
In respiratory therapy departments, the CQI program that is performed will probably be the sole responsibility of a few key team members and the team leader. They will be expected to develop, educate, and include all staff members; implement the CQI program, analyze its effect on quality, and continue with a revised and updated process as recommended by the hospital’s quality experts. It is also noted that local data on outcomes for comparison may be difficult to obtain. It is understood that structural improvement may be beyond the reach of an emerging CQI initiative. Unless the respiratory therapy department’s environment is receptive, the quality-improvement team is expected to initially focus on improvement of processes rather than on more-complex improvements of structure or outcomes. When the respiratory therapy department’s CQI process has proven itself to be worthwhile, then the quality-improvement team of the respiratory therapy department will find themselves in a better position to address other issues.59
Summary
The concept of quality in health-care settings is growing and is considered to be a worthwhile goal for health-care professionals and management when it comes to patient safety and provision of care. No CQI program in a hospital should exclude the respiratory therapy department. The best way to ensure quality in respiratory therapy departments is to establish an optimal structure and equip it with carefully laid out processes. This will lead to a set of outcomes that need to be monitored and improved. Any CQI intervention must have a clear-cut benefit for patients, be suited to local needs and budgetary provisions, and be able to provide evidence that reflects its utility.
Blindly following unproven CQI interventions may not prove to be effective but may prove to be exhaustive and expensive. CQI in health-care organizations is in the nascent stages and will undergo validation and improvement. It is important for the leadership and the quality-improvement team of respiratory therapy departments to be aware of these changes and to incorporate them into their practice. RTs are considered to be the clinical experts of multidisciplinary respiratory care areas in any hospital or health-care setting. Besides the clinical practice, their involvement in quality-improvement programs as process experts, therefore, will likely have a favorable outcome in organizational objectives, employee satisfaction, and, most importantly, in patient-centered care.
ACKNOWLEDGMENT
The authors thank B Krishnamurthy MD and Dhanista Battula (Quality Consultants, India) and Catherine Hogan (Director of Institutional Quality, Effectiveness and Accreditation, Khawarizmi International College, UAE.) for sharing their valuable insights during the preparation of this article.
Footnotes
- Correspondence: Manjush Karthika PhD, Department of Health and Medical Sciences, Khawarizmi International College, Abu Dhabi, UAE 25669. E-mail: manjushnair{at}hotmail.com
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}