

Abstract
BACKGROUND: Two orotracheal extubation techniques are described in the literature: the traditional technique and the positive-pressure technique. Although prior studies reported better clinical outcomes with the positive-pressure extubation technique, its superiority has not been extensively studied yet. This study was to determine whether the positive-pressure orotracheal extubation technique, compared with the traditional orotracheal extubation technique, reduces the incidence of major postextubation complications (up to 60 min) in critically ill adult subjects.
METHODS: This was a multi-center randomized clinical trial. Subjects age > 18 y, requiring invasive mechanical ventilation through an endotracheal tube, who met the orotracheal extubation criteria were included and randomized to traditional extubation group (removing the endotracheal tube by applying continuous endotracheal suctioning during the entire procedure) or positive-pressure group (application of pressure support mode at 15/10 cm H2O during cuff deflation and extubation). The primary measure was postextubation major complications, defined as the clinical evidence of at least one of the following: desaturation, upper-airway obstruction, or vomiting.
RESULTS: A total of 725 subjects was randomly assigned to the traditional extubation group (n = 358) and positive-pressure group (n = 367). Seventeen subjects were eliminated and not included in the per-protocol analysis. Of 708 subjects, 185 (26.1%) developed at least one major complication. The incidence was 27.8% (96/345) in the traditional group compared with 24.5% (89/363) in the positive-pressure group. No statistically significant differences were observed between the 2 groups (absolute risk 3% [95 CI −3 to 10]; relative risk, 0.88 [95 CI 0.69−1.13], P = .32).
CONCLUSIONS: Despite the trend toward the positive-pressure group, no statistically significant differences were observed. Our findings agree with the literature in that positive-pressure extubation is a safe procedure; therefore, both techniques may be used during extubation in critically ill adult patients.
- airway extubation
- ventilator weaning
- extubation methods
- extubation complications
- positive pressure
- positive-pressure extubation
Introduction
Extubation is the removal of the endotracheal tube (ETT) when it is no longer required.1 This procedure may be associated with complications, such as desaturation, stridor, bronchospasm, and severe cough.2,3 The complication rates reported in the literature range from 6.6–100%.4-6 In some cases, these complications may lead to extubation failure. 7
Two orotracheal extubation techniques are described in the literature.8 The traditional extubation technique consists of introducing a suction catheter into the ETT and trachea, deflating the cuff, and removing the ETT by applying continuous endotracheal suctioning during the entire procedure. The positive-pressure extubation technique, on the other hand, involves applying positive pressure through the airway during cuff deflation and extubation. Thus, the air flow passing between the ETT and the larynx pushes pooled subglottic secretions toward the oropharynx so that they can be expelled through the oral cavity.
Any strategy toward preventing leakage of fluid during cuff deflation and ETT removal should be considered. The traditional extubation technique suggests applying continuous endotracheal suctioning during the procedure.9,10 However, the negative pressure generated by suctioning seems to counteract the positive-pressure gradient created by the ventilator, which promotes rather than reduces leakage.2,5,6 Still, over 85% of professionals reported applying endotracheal suctioning during extubation.11,12
A noninferiority clinical trial showed that the positive pressure extubation technique was safe and noninferior to the traditional technique in terms of the incidence of immediate postextubation complications, postextubation pneumonia, extubation failure, and re-intubation.13 Although prior studies reported better clinical outcomes with the positive-pressure extubation technique,6,14 its superiority has not been deeply studied yet. Therefore, the objective of our study was to determine whether the positive-pressure extubation technique, compared with the traditional extubation technique, reduces the incidence of major postextubation complications (up to 60 min) in critically ill adult subjects.
QUICK LOOK
Current Knowledge
Two orotracheal extubation techniques are described in the literature: the traditional technique and the positive-pressure technique. Although prior studies reported better clinical outcomes with the positive-pressure extubation technique, its superiority has not been extensively studied yet.
What This Paper Contributes to Our Knowledge
We examined the superiority of the positive-pressure extubation technique in terms of major postextubation complications (up to 60 min) in critically ill adult subjects. Although there was a tendency in favor of the positive-pressure group, no statistically significant differences were found. This supports prior studies according to which positive-pressure extubation is safe, and professionals may use either technique in their habitual practice.
Methods
Design
A multi-center randomized clinical trial was conducted in 13 centers from Argentina. Subjects admitted to the ICUs between April 1, 2019, and March 26, 2020, were included in the analysis. Our study was reviewed and approved by the institutional review board of the Hospital Donación Francisco Santojanni (#12-2018-05, approved on February 28, 2019) and is registered on ClinicalTrials.gov (NCT03918811, April 18, 2019). The results were reported according to the CONSORT guideline.15
Subjects
We included subjects age > 18 y, requiring invasive mechanical ventilation through an ETT, who had successfully completed a spontaneous breathing trial (SBT)16,17 and met the following extubation criteria: an adequate level of consciousness (Glasgow coma scale score ≥ 8/15)18 and effective cough (cough at order and/or at endotracheal suctioning).19,20 The participants’ or their legal representatives’ informed consent was also required. Patients with a history of upper-airway injury or surgery, with an adequacy therapeutic effort, who had previously been extubated or tracheostomized, or who had required noninvasive ventilation (NIV) as a weaning method were excluded from our study.
Randomization
The randomization sequence was generated before the study, by using a web site (https://www.sealedenvelope.com, Accessed January 10, 2019), in blocks of 6 and stratified by participating center and by the risk of extubation failure (high or low), as reported in prior studies.19,21 High risk of extubation failure was defined as the presence of at least one of the following criteria: age ≥ 66 y, moderate or severe COPD, > one comorbidities (COPD, peripheral artery disease, immune deficiency, liver disease, hypertension, diabetes, neurological disease, heart failure, chronic renal failure), body mass index > 30 kg/m2, congestive heart failure as main reason for invasive mechanical ventilation, difficult intubation, invasive ventilation > 7 d, a requirement of suctioning respiratory secretions (> 2 suctions within 4 h before extubation), difficult or prolonged weaning, and/or Acute Physiology and Chronic Health Evaluation II (APACHE II) > 12 the day before extubation. Randomization assignment was blinded to researchers in charge of recruiting subjects through an online platform designed exclusively for the purpose of this study.
Blinding
Due to the nature of the intervention, blinding of subjects and operators performing the extubation procedure was not possible. The evaluator who recorded measures of interest after extubation was blinded to the assigned extubation technique. The database was monitored by third parties with no direct participation in the study and no interest in its outcomes. The data were analyzed pursuant to the statistical analysis plan devised before the study, and the person in charge of data statistical analysis was blinded to the technique used.
Procedures
Subjects were included in the study once they had successfully completed the SBT and met extubation criteria. SBT was conducted with a T-tube, by applying CPAP at 5 cm H2O, or by applying pressure support ventilation (PSV) from 5–8 cm H2O for a period ranging from 30–120 min. The oxygen flow or  was regulated to keep an oxygen saturation >90%. Subjects who met the eligibility criteria and successfully completed the SBT were immediately randomized.
was regulated to keep an oxygen saturation >90%. Subjects who met the eligibility criteria and successfully completed the SBT were immediately randomized.
The blinded evaluator followed a preextubation checklist. It entailed discontinuing enteral nutrition, adjusting the head of the bed to 45o, suctioning oropharyngeal and tracheobronchial secretions, and recording preextubation monitoring on the pertaining sheet. Regardless of the procedure, the alarms were silenced, and the ventilator parameters were set at PSV mode with an inspiratory pressure of 15 cm H2O and PEEP of 10 cm H2O so that the blinded evaluator could not hear the maneuver or read the ventilator parameters. The blinded evaluator left and was replaced by the operators, who knew about the technique assigned. They initiated the randomization through an online platform and were in charge of the extubation and postextubation oxygen delivery. Regardless of the extubation technique, the subjects received supplemental oxygen through a nasal cannula placed before ETT removal to keep the same FIO2 used at the end of the successful SBT.
Once the extubation was completed, the blinded evaluator assessed the outcome measures recorded within 60 min after extubation. Daily monitoring of outcome measures within 72 h after extubation was carried out. All variables were collected and recorded in specific forms.
The decision to extubate and to use NIV or high-flow nasal cannula (HFNC) to prevent extubation failure, follow-up, and treatment was taken by the blinded evaluator, or the respiratory therapist on duty, who was blinded to randomization assignment. If preventive NIV or HFNC had previously been decided, it was implemented 15 min after extubation so as not to affect monitoring of outcome measures.
Interventions
Extubation maneuvers were performed in accordance with the procedure reported in the literature.13,22,23 Both procedures were performed by 2 operators. In the traditional orotracheal extubation (extubation), a closed suction system catheter was placed into the ETT by the first operator, and endotracheal suctioning was initiated. The cuff was immediately deflated by the second operator, and the ETT was removed with continuous endotracheal suctioning during the entire procedure. In the positive-pressure extubation, the first operator set the ventilator parameters to PSV 15/10 cm H2O. Then the cuff was deflated by the second operator, and the suction catheter was introduced through the mouth to suction secretions drawn to the oropharynx while the ETT was removed by the first operator without applying endotracheal suctioning. Before the study, the participating centers were trained in both extubation procedures by means of videos.
Outcome Measures
Postextubation overall complications13 were defined as clinical evidence of at least one of:
Either at 1, 5, or 15 min after extubation:
Desaturation:3,6,24
 < 90% or a 4-point decrease compared with preextubation .5 A lower value maintained for at least 10 s was recorded.
< 90% or a 4-point decrease compared with preextubation .5 A lower value maintained for at least 10 s was recorded.Hypertension:3,4,24 systolic blood pressure > 180 mm Hg or increased by > 20% from preextubation.1
Tachycardia:3,4,24 heart rate > 140 beats/min or increased by > 20% from preextubation.1
Tachypnea:25 breathing frequency > 35 breaths/min or increased by > 50% from preextubation.1
Poor respiratory mechanics:25 the presence of thoraco-abdominal asynchrony or inspiratory and/or expiratory effort, as observed by the evaluator.


Within 60 min after extubation:
Upper-airway obstruction: the presence of laryngeal stridor, audible with or without a stethoscope.4,26
Postobstructive pulmonary edema: defined as desaturation and pink frothy sputum after upper-airway obstruction.2,26
Bronchospasm:5,26 audible with or without a stethoscope. Bronchospasm was considered a complication only in subjects not presenting the event during the T-piece test performed before orotracheal extubation.
Severe cough:3,5 defined as more than one episode of sustained cough (> 5 s).27
Postextubation major complications:13 clinical evidence of desaturation (within 15 min after extubation) or clinical evidence of upper-airway obstruction or vomiting (at least one within 60 min after extubation).
Postextubation minor complications:13 clinical evidence of hypertension, tachycardia, tachypnea, or poor respiratory mechanics (at least one within 15 min after extubation) or clinical evidence of postobstructive pulmonary edema, bronchospasm, or severe cough (at least one within 60 min after extubation).
Postextubation pneumonia was defined as the presence of new or increased pulmonary infiltrate on chest radiography after extubation in addition to the presence of fever, leukocytosis (> 10,000/mm3), or leukopenia (< 4,000/mm3) compared with preextubation values and/or increase of tracheobronchial secretions or change in their quality (within 72 h after extubation).19
Extubation failure was defined as the need for NIV or HFNC to treat the failure or re-intubation within 72 h after extubation.1,28 Re-intubation was defined as the need for a new introduction of the ETT within 72 h after extubation.1,29
Sample Size Calculation
Based on a major complication rate of 37.6%, reported in a prior study,13 778 subjects (389 per group) were required to have an 80% chance of detecting, as significant at the 5% level, a decrease in the incidence of major complications from 37.6% in the control group (traditional technique) to 28.2% in the experimental group (positive-pressure technique) (relative difference of 25%) (obtained via https://www.sealedenvelope.com/power/binary-superiority, Accessed November 25, 2018).
Statistical Analysis
The primary analysis of outcomes was a per-protocol analysis. An intention-to-treat analysis was also performed. Thus, a worst-case scenario method was adopted, assigning the event of interest to the subjects lost to follow-up who were randomly assigned to the positive-pressure group and not allocating the event of interest to the subjects lost to follow-up who were randomly assigned to the traditional group. No interim analyses were planned. Chi-square test or Fisher exact test was used for the comparison categorical variables. Continuous variables with normal distribution were presented as mean and SD and were compared with the Student t test for independent samples. Non-normally distributed variables were presented as median and interquartile range (IQR). For outcome measures (primary and secondary), relative risk and 95% CI were calculated. Effect estimates were also reported with their absolute risk differences and their corresponding 95% CI. Tests were 2-tailed, and a P value < .05 was considered significant. Statistical analysis was performed using SPSS Version 25.0 (IBM, Armonk, New York).
Results
Subjects’ Characteristics
Due to the outbreak of the SARS-CoV-2 pandemic in Argentina and the lack of information about the potential risks of contamination from extubation and aerosolization, we stopped recruiting subjects before achieving the predefined sample size. Therefore, and by recommendation of the research ethics committee, our study ended on March 26, 2020.
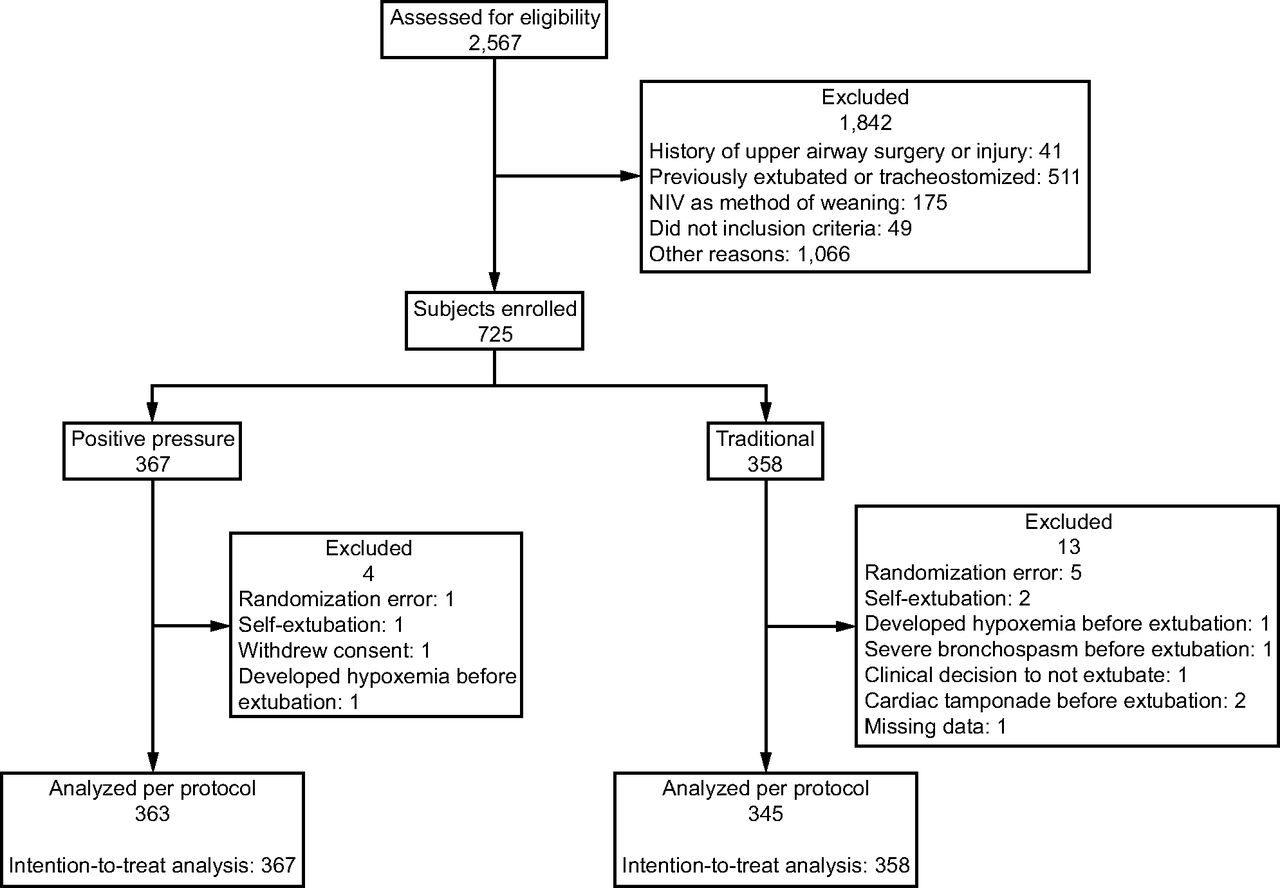
A total of 2,567 patients met the eligibility criteria; 1,842 were excluded from the study, and 725 were randomly assigned to the traditional extubation group (n = 358) and positive-pressure extubation group (n = 367). Seventeen (2.3%) subjects were eliminated and not included in the per-protocol analysis (Figure 1). No statistically significant differences were observed in baseline and preextubation characteristics between the 2 groups (Tables 1 and 2). Of the 13 participating centers, 8 reported using the traditional technique and 4 the positive-pressure technique as their habitual practice. One center reported using both techniques.

Flow chart. NIV = noninvasive ventilation.
Subjects’ Characteristics
Preextubation Characteristics
Primary Outcomes
Of 708 subjects, 185 (26.1%) developed at least one major complication. The incidence was 27.8% (96/345) in the traditional group compared with 24.5% (89/363) in the positive-pressure group. No statistically significant differences were observed between the 2 groups (absolute risk 3% [95% CI −3 to 10]; relative risk 0.88 [95% CI 0.69–1.13], P = .32). To identify and control for potential confounding variables related to major complications, we constructed a post hoc conditional backward stepwise multivariable logistic regression model including the variables age, ETT diameter, extubation technique as their habitual practice, comorbidities > 1, COPD, congestive heart failure, difficult airway, APACHE II on extubation day, difficult or prolonged weaning, body mass index > 30, duration of ventilation before SBT, endotracheal suction > 2 on extubation day,  % before extubation, type and duration of SBT, and extubation technique. The multivariable regression model showed that the variables independently associated with major complications were
% before extubation, type and duration of SBT, and extubation technique. The multivariable regression model showed that the variables independently associated with major complications were  % before extubation (odds ratio 1.074 [95% CI 1.002–1.151), P = .044] and duration of ventilation before SBT (odds ratio 1.043 [95% CI 1.008–1.079], P = .02). COPD (odds ratio 0.610 [95% CI 0.362–1.029], P = .064) and comorbidities > 1 (odds ratio 1.391 [95% CI 0.980–1.975], P = .065] were retained in the final step of the model. The extubation technique and the rest of the variables were discarded from the model.
% before extubation (odds ratio 1.074 [95% CI 1.002–1.151), P = .044] and duration of ventilation before SBT (odds ratio 1.043 [95% CI 1.008–1.079], P = .02). COPD (odds ratio 0.610 [95% CI 0.362–1.029], P = .064) and comorbidities > 1 (odds ratio 1.391 [95% CI 0.980–1.975], P = .065] were retained in the final step of the model. The extubation technique and the rest of the variables were discarded from the model.
Secondary Outcomes
The incidence of minor complications was 45.2% (156/345) in the traditional group compared with 39.75% (144/363) in the positive-pressure group. No statistically significant differences were observed between the 2 groups (absolute risk 5% [95% CI −2 to 13]; relative risk 0.88 [95% CI 0.74–1.04], P = .13).
A total of 387/708 subjects (54.7%) developed at least one immediate postextubation complication. No statistically significant differences were observed in overall complications between the groups (absolute risk 5% [95% CI −3 to 12]; relative risk 0.92 [95% CI 0.8–1.05], P = .20).
Postextubation pneumonia was diagnosed in 42 subjects, 24 (7%) of the traditional group and 18 (5%) of the positive-pressure group (absolute risk 2% [95% CI −1 to 6]; relative risk 0.71 [95% CI 0.39–1.29], P = .26).
A total of 109 (15.4%) subjects failed extubation within 72 h. Extubation failure was more prevalent in the traditional group compared with the positive-pressure group, but there were no statistically significant differences (61 [17.7%] subjects vs 48 [13.2%]); (absolute risk 5.0% [95% CI −1 to 10]; relative risk, 0.75 [95% CI 0.53–1.06], P = .10) (Table 3). Of the 109 subjects, 76 were directly re-intubated (41 [67.2%]) in the traditional group versus 35 (72.9%) in the positive-pressure group; P = .52.
Primary and Secondary End Points
Extubation failure within 72 h after extubation was more prevalent in subjects at high risk of extubation failure than in subjects at low risk, both in the traditional group (54/284 high-risk subjects [19.0%] vs 7/61 low-risk subjects [11.5%]; P = .16) and in the positive-pressure group (42/299 high-risk subjects [14%] vs 6/64 low-risk subjects [9.4%]; P = .32), but there were no statistically significant differences (96/583 [16.5%] vs 13/125 [10.4%]; P = .09).
Re-intubation within 72 h after extubation, whether direct re-intubation or after failure with NIV or HFNC, was more prevalent in the traditional than in the positive-pressure group with no statistically significant differences (51 [16.3%] vs 44 [13.8%]; absolute risk 3% [95% CI –2 to 8]; relative risk 0.82 [95% CI 0.56–1.19], P = .36).
Thirty-eight (34.9%) subjects died in the ICU after developing postextubation respiratory failure (34/96 high-risk subjects [35.4%] vs 4/13 low-risk subjects [30.8%]; P = .99). No statistically significant differences were observed in mortality between the 2 groups (P = .48). Another 48 subjects died in the ICU after 72 h due to reasons not related to extubation.
Mortality was more prevalent in subjects failing extubation within 72 h (38/109 [34.9%] subjects in the extubation failure group and 48/599 [8%] subjects in the group without failure; P < .001). In this group, mortality in subjects re-intubated within 72 h after failing NIV or HFNC was higher than in those directly re-intubated. However, no statistically significant differences were observed (8/19 [42.1%] vs 29/76 [38.2%]; P = .75).
The median ICU length of stay was not statistically different between the 2 groups (9 d [IQR 5–17]) in the traditional group vs 8 d [IQR 5–16] in the positive-pressure group; P = .38).
Complications
The most prevalent postextubation complication was desaturation (23.0%), followed by hypertension (21.6%) and tachycardia (14.4%). Only one subject (0.3%) developed pulmonary edema after extubation (Table 4). Desaturation was observed in 163 subjects with a median of decrease in  compared with preextubation
compared with preextubation  of 5 points (IQR 4–6), without statistically significant difference between the 2 groups (5 points [IQR 4–6] decrease in the traditional group vs 5 points [IQR 4–6] decrease in the positive-pressure group; P = .37).
of 5 points (IQR 4–6), without statistically significant difference between the 2 groups (5 points [IQR 4–6] decrease in the traditional group vs 5 points [IQR 4–6] decrease in the positive-pressure group; P = .37).
Postextubation Complications
Discussion
Positive-pressure extubation was expected to be superior to the traditional extubation technique.13,22 Although there was a tendency in favor of the positive-pressure group, no statistically significant differences were found. The multivariable regression analysis supports these results.
Aspiration of oropharyngeal content (leakage) during cuff deflation and extubation may have no relevant clinical manifestations; however, it may result in pneumonitis or pneumonia.9,11,30-33 To reduce the risk of leakage, different methods are used during this procedure.8,9,22,23 In a previous study, the incidence of postextubation pneumonia within 72 h was 4%.19 The overall incidence of postextubation pneumonia in our study was 6%, and it was lower in the positive-pressure group. However, there were no statistically significant differences between the 2 groups. Although postextubation pneumonia seems to be greatly influenced by extubation, its pathophysiology and development are still unclear and depend on multiple factors.34
One maneuver to reduce the volume of leakage during extubation involves applying positive pressure. Two lab studies reported a decreased volume of leakage by applying different positive-pressure levels during deflation and extubation.9,23 In a clinical trial, the PSV set at 15/10 cm H2O reduced the rate of major complications by 13% compared with the traditional technique.13 Such decrease was much higher than the 3% difference observed in our study. It could be attributed to the fact that in that study the professionals did not use the traditional extubation technique in their daily practice; therefore, they were highly trained in the positive-pressure technique. This could have biased the results in favor of positive-pressure extubation. In the present study, on the other hand, we included 13 centers with different levels of experience in the techniques. Of them, only 5 used the positive-pressure extubation technique in their habitual practice, which agrees with the literature in that most professionals use the traditional technique.11,12 For standardization, we provided training through explanatory videos and conducted a pilot test. Another possible explanation for the difference could be based on other variables not related to the inherent benefits of positive pressure (less leakage, lower loss of lung oxygen stores, among others).6,9,23
Although there were no significant differences between groups, applying positive pressure reduced the rate of major complications by 3%, which may account for the lower rate of desaturation. Oxygenation impairment is one of the most prevalent extubation complications3 and is associated with decreased lung volume and oxygen stores during endotracheal suctioning. That is the reason why several studies comparing extubation techniques have analyzed this variable.6,14,35
Similarly, applying positive pressure decreased the rate of minor complications by 5%. Positive-pressure extubation reduced the leak volume during cuff deflation and extubation.9,23 Leakage may cause isolated events of cough and higher discomfort and, consequently, induce a higher adrenergic discharge and tachycardia. This procedure may account for a lower rate of minor complications in the positive-pressure group.13,36
Immediate postextubation complications were frequent in our sample of critically ill subjects who required invasive mechanical ventilation due to different reasons. However, it is unknown whether these complications lead to worse clinical results or they are a mere effect of the extubation procedure.
Postextubation complications have a different impact on patients’ clinical course in terms of extubation failure and re-intubation,37 and major complications cause a higher impact on their clinical course. Fifteen percent of our subjects failed extubation and required re-intubation. Similar rates were reported in the literature.19,28,38-44 These subjects have a poor prognosis and may require prolonged invasive mechanical ventilation with an increased risk for death of up to 50%.19,28,45 Although there were no significant differences between the groups, it should be noted that extubation failure and re-intubation were lower in the positive-pressure group, mainly in the subgroup identified as at high risk of extubation failure. In a prior study, this subgroup also had a better outcome.21
One finding of our study was that preventive NIV to avoid extubation failure was used in only 12% of subjects, considering that > 80% of our sample met at least one of the criteria for high risk of failure. The decision to apply preventive NIV remained at the discretion of the attending physician and local protocols.
Our study described a mortality rate in the ICU of 12%, which was higher than the rate reported in a prior study with a similar population.21 Although the mortality rates were lower in the positive-pressure group, no statistically significant differences were found between the 2 groups, as mortality may be associated with long-term conditions after extubation and other conditions not related to the procedure.
One strength of our study was the analysis of a heterogeneous population, which included critical subjects with clinical and surgical pathologies. As the study included multiple centers, public and private, and was conducted on subjects at low and high risk of extubation failure, outcomes may be extrapolated and generalized to different critical care units.
Our study has some limitations. The classification into major and minor complications was only supported and validated by the experts' opinion. The experts were asked, through an e-mail survey, to classify complications into major and minor according to their potential clinical impact on recently extubated subjects.13,37 Complications were identified in studies conducted on subjects extubated immediately after anesthetic recovery, which could differ from the complications in critical subjects.3,5,24,45,46
The sample size was predefined to identify a difference similar to our prior study. The clinical implications of lower differences between the groups are unknown. Due to the pandemic, the recruitment period had to end before reaching the necessary sample size. A post hoc power analysis (obtained via http://powerandsamplesize.com, Accessed October 28, 2020) indicated that the sample size of this randomized clinical trial achieved a power of 86.2% according to the magnitude of the differences observed (−3%). We consider that if the sample size had been reached our findings would not have changed.
The cuff-leak test was proposed to predict the presence of laryngeal edema and postextubation airway obstruction.47,48 The limitation of cuff-leak test has been repeatedly discussed. Cuff-leak test can be susceptible to relationship of tube size to laryngeal diameter,49 respiratory system compliance and resistance, inspiratory flow, expiratory flow and time, and airway collapse,50 and clinicians should bear in mind that the ability of cuff-leak test may vary according to the condition or type of patients.51 A recently systematic review and meta-analysis52 informed that the cuff-leak test has excellent specificity but moderate sensitivity. The authors concluded that the cuff-leak test works better to rule in than to rule out potential postextubation airway obstruction; therefore, patients should still be closely monitored postextubation. Continued research to find better modalities to rule out postextubation airway obstruction is needed. In our study, the cuff-leak test was excluded as a criterion for extubation because it is not systematically performed in our clinical practice.
On the other hand, we have not registered other variables that have been related to the risk of failure during extubation (eg, sedation doses, ventilation modes, requirements for neuromuscular relaxation, use of corticosteroids, delirium).53,54 Furthermore, we have not protocolized weaning, extubation, postextubation care, or strategies for preventing ventilator-associated pneumonia and postextubation pneumonia. Our pragmatic approach is a reflection of daily clinical practice in different centers with different approaches to postextubation airway management, which improves the external validity of our study.
Finally, we did not assess the impact of both techniques on the risks sustained by professionals resulting from exposure to aerosolization. Aerosolization has gained considerable importance since the outbreak of the COVID-19 pandemic. We followed the personal care standards recommended for extubation in both groups.22,55
Positive-pressure extubation is a safe and simple procedure that requires a small number of professionals compared with traditional extubation, since the latter requires an operator to apply continuous endotracheal suctioning and another to deflate the endotracheal cuff simultaneously before removing the ETT.8 There were no significant differences, but all estimates favored the positive-pressure group. This supports prior studies according to which positive-pressure extubation is safe, and professionals may use both techniques in their habitual practice. However, some aspects need further consideration. It would be interesting to identify the risks of aerosolization of extubation techniques considering recently available information arising from the COVID-19 pandemic. It would be also relevant to determine the effects on other outcome measures, such as patients’ comfort.
Conclusions
Despite the trend toward the positive-pressure group, no statistically significant differences were observed. Our findings agree with the literature in that positive-pressure extubation is a safe procedure; therefore, both techniques may be used during extubation in critically ill adult subjects.
Acknowledgements
We would like to thank the chiefs of all the ICUs that participated and allowed us to conduct this study as well as the respiratory therapists, nurses, and physicians who collaborated with us during the procedures and data collection.
Footnotes
- Correspondence: Mauro Andreu PT, Department of Health Sciences, Universidad Nacional de la Matanza, Florencio Varela 1903, B1754, San Justo, Buenos Aires, Argentina. E-mail: mfandreu@gmail.com
This trial is registered on clinicaltrials.gov (NCT03918811, April 18, 2019).
The authors have declared no conflicts of interest.
- Copyright © 2022 by Daedalus Enterprises





{kind=link}