

Abstract
BACKGROUND: Automatic tube compensation (ATC) is an option available in any ICU ventilator that compensates for the resistive pressure drop due to the endotracheal tube. The goal of the present study was to compare ATC to other patient triggered modes of support in terms of spontaneous breathing trial (SBT) and extubation success.
METHODS: Two authors (JB and PCF), independently and blinded to each other, searched through PubMed, Web of Science, and Cochrane from inception–May 26, 2021, with the following search terms entered as MeSH terms in all fields: “Automatic Tube Compensation.” Inclusion criteria: randomized studies that included subjects > 16 y old undergoing an SBT. Exclusion criteria: crossover studies, pediatric studies, animal studies, or experimental studies on test lungs or on computer simulation; other languages than French, Spanish, or English; studies not published in a full-text format (eg, abstract or letter); and reviews. A frequentist network meta-analysis was conducted with the aim to investigate the effectiveness of ATC on SBT and extubation outcomes. SBT was defined as successful if patients could tolerate the SBT based on predetermined criteria, whether it was followed by extubation. Successful extubation was defined as the absence of re-intubation, noninvasive ventilation, or signs of respiratory distress within the 48 h after extubation. The pooled analyses used random-effect models, and the effect size was expressed as relative risk or mean difference for categorical and continuous variables, respectively. P-scores were used to rank all treatments and to identify the intervention with the highest probability of being the best.
RESULTS: Of the 234 retrieved papers, 7 met the inclusion criteria. In terms of SBT success, ATC100+PEEP < 7.5 and PS10+PEEP < 7.5 were superior to T-piece. Likewise, PS10+PEEP < 7.5 was the intervention with the highest probability of being the best (P-score: 0.90). In terms of extubation success, ATC100+PEEP < 7.5 cm H2O was significantly better than PEEP < 7.5 and T-piece. Likewise, it had the highest probability of being the best (P-score= 0.90).
CONCLUSIONS: ATC is the modality with the highest probability of extubation success but not in terms of SBT success.
Introduction
Intubation is a lifesaving procedure performed in the ICU. However, duration of invasive mechanical ventilation should be minimized, secondary to the risk of ventilator-induced lung injury,1 lung infection, myotrauma,2 and hemodynamic impairment. Therefore, weaning a patient from invasive mechanical ventilation is a key process aimed at reducing the number of days under invasive mechanical ventilation, and minimizing the risk of extubation failure and need for re-intubation, as this can lead to adverse patient outcome.3 Since the pioneering work by Ely et al,4 the weaning process is driven by the caregiver team selecting patients who are suitable for a spontaneous breathing trial (SBT) based on physiological indexes to predict weaning failure or success and suitability to extubate. Low pressure support (PS) level or T-piece, each with or without a low level of PEEP, are the most commonly used SBT techniques.5 Results from a recent multi-center randomized controlled trial6 support the use of the former method.
The use of low PS was initially proposed as a method to counterbalance the resistive work of breathing due to endotracheal tube (ETT) resistance.7 However, low PS provides inspiratory support that is not precisely calibrated to compensate ETT-related workload.8 Automatic tube compensation (ATC) provides support equivalent to the selected ETT size.9 Although several studies have been carried out in this field, it is still not clear which approach is the most effective in terms of extubation success. Therefore, we sought to answer the following questions: In individuals ready to be extubated (subjects and controls) is ATC different than other SBT methods in terms of SBT and extubation outcome? A recent meta-analysis on this topic did not provide any definitive conclusion.10 This, at least in part, is determined by the absence of direct comparisons across the different weaning approaches. Thus, we performed a network meta-analysis (NMA) to compare ATC versus other SBT modes. NMAs allow the comparison of more than 2 interventions simultaneously when studies making direct comparisons are not available, also ranking the interventions according to their effectiveness.11
Methods
Inclusion Criteria of the Studies
The inclusion criteria of the studies were based on the population-intervention-comparison-outcome approach: (1) Subjects: adults (> 16 y old) intubated in the ICU for ≥ 24 h; (2) intervention: ATC; (3) control: no ATC intervention; and (4) outcome: SBT and extubation success.
Eligibility Criteria of the Studies
Randomized controlled trials that compared ATC with other SBT methods and provided data on success/failure of extubation or SBT at the end of the SBT were eligible. Exclusion criteria were crossover studies, pediatric studies, animals studies, or experimental studies on test lungs or on computer simulation; other languages than French, Spanish, or English; studies not published in a full-text format (eg, abstract or letter); and reviews.
Search Strategy
Two authors (JB and PCF), independently and blinded to each other, searched through PubMed, Web of Science, and Cochrane from inception–May 26, 2021, with the following search terms entered as MeSH terms in all fields: “Automatic Tube Compensation.” The same authors also searched for references in the included studies by using a snowballing strategy.
The same 2 investigators selected the retrieved studies, first by reading the title and then after reading the abstract. The discrepancy in the list of the retrieved and included studies by each investigator was resolved by consensus. If needed, a third person (CG) was asked for the final decision.
From the selected articles, a NMA was carried out according to the protocol sent to the register PROSPERO on June 28, 2020. Despite many queries we sent to the PROSPERO web site, we did not receive any answer; and hence, we decided to start the systematic review without a PROSPERO number.
Data Extraction
The same 2 authors (JB and PCF) independently extracted the data of selected studies. Data were stored in a custom Excel spreadsheet (Microsoft, Redmond, Washington) and included author, year of publication, number of subjects, success of SBT, success of extubation, age, gender, severity score (Acute Physiology and Chronic Health Evaluation [APACHE]), and duation of mechanical ventilation.
Definition of Groups
The ATC group was defined regardless of the proportion of the tube compensation provided by the ventilator and whether the compensation was done during inspiration or expiration or in both directions. Risk of bias was assessed using the Cochrane risk-of-bias assessment tool from the following 7 items: randomization sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessors, incomplete outcome data, and selective reporting another bias. Each item was labeled as low, unclear, or high risk of bias according to the evaluation criteria.12
End Points
The primary end point was SBT and extubation outcomes, and the secondary end point was the duration of invasive ventilation. A priori, 4 variables (APACHE II score, age, sex, and PaO2/FIO2 at the time of SBT) were considered as confounding factors. We hypothesized that if there is no difference between SBT modality for each confounding variable it can be assumed that all studies are comparable. The definition of SBT success/failure was that of the authors; it was similar in all included studies and briefly considered the immediate extubation after the SBT. The definition of extubation failure included re-intubation, noninvasive ventilation, or signs of respiratory distress within 48 h of extubation.
Data Analysis
We followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines involving NMA. The completed PRISMA-NMA checklist is available at Appendix 1 (see related supplementary materials at http://www.rcjournal.com). Continuous variables were expressed as mean and SD. When the data were not given as numbers in tables or in main text but only in figures, we used the WebPlotDigitizer 4.4 software online (Ankit Rohatgi, Pacifica, California) to extract the relevant data. In addition, continuous variables reported as percentiles were transformed in mean and SD.13
ATC was always the reference treatment. A random-effects model was used assuming heterogeneity across the studies. We used network plots to illustrate the map of direct and indirect comparisons. In this plot, each node corresponds to the intervention under investigation. The size of the node is proportional to the number of included subjects in the group; the thickness of the line between 2 nodes is proportional to the number of studies involved in the between-group comparison.
We used a forest plot to report the effect and the probability of being the most effective SBT intervention to predict the outcome of interest versus ATC as the control (ATC100+PEEP < 7.5). The effect was reported in terms of relative risk (95% CI) or mean difference (SD). Meanwhile, the probability of being the best was estimated according to the P-score (note that P-score is different from P value) of each treatment. The P-score of treatment i is defined as the mean of all 1 − P[j], where P[j] denotes the one-sided P value of accepting the alternative hypothesis that treatment i is better than one of the competing treatments j. For the sake of clarification, P-score could be considered as an analog of the surface-under-the-cumulative-ranking-curve method for Bayesian NMA. It is based solely on the point estimates and standard errors of the frequentist NMA estimates under normality assumption. It measures the mean extent of certainty that a treatment is better than the competing treatments (the higher the P-score, the higher the probability of being successful). Thus, if treatment i is better than many other treatments, many of these P values will be small and the P-score will be large. Vice versa, if treatment i is worse than most other treatments, the P-score is small.14
We used matrix tables to report the results of direct and indirect comparisons. Tables include a diagonal row with each intervention (highlighted in black letters); above this line is reported the direct evidence (blank cell means that no direct evidence is available) and below indirect evidence. The effect of each comparison is reported as relative risk (95% CI) or mean differences. Significant results are highlighted in red.
The overall inconsistency was assessed by the I2 statistics, its imprecision with 95% CI. We used funnel plot to analyzed the publication bias adjusted for the main result. The asymmetry in funnel plots was tested by the Egger method. A P < .05 was considered statistically significant. The NMA was performed using the frequentist method with the netmeta library of the R software version 4.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
The search retrieved 234 studies, 7 of which were15-21 randomized controlled trials (Fig. 1 and Table 1). Supplementary Table 1 (see related supplementary materials at http://www.rcjournal.com) summarizes the articles included in each network. The quality of evidence assessment is reported in Supplementary Figure 1 (see related supplementary materials at http://www.rcjournal.com). All studies were at high risk of bias mainly because they were not blinded. Moreover, in some studies the randomization procedure was not reported.

Flow chart.
Included Studies
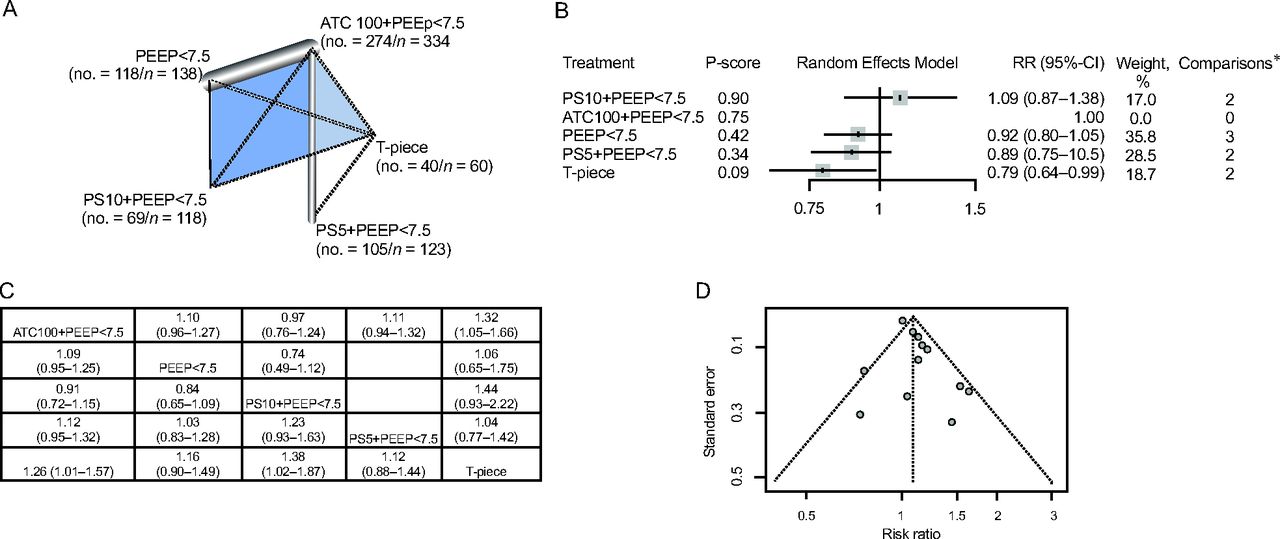
No differences in age, sex, and PO2/FIO2 according to the SBT procedure were identified. However, mild differences in severity at ICU admission were identified (Supplementary Fig. 2, see related supplementary materials at http://www.rcjournal.com). For the SBT outcome, there were 6 studies with 655 participants (Fig. 2A).15-18,20,21 Direct comparison showed that ATC100+PEEP < 7.5 was associated with a significantly higher probability of a successful SBT compared to T-piece. Indirect comparison also showed that PS10+PEEP < 7.5 was superior to T-piece trials (Fig. 2B and 2C). Likewise, PS10+PEEP < 7.5 was the intervention with the highest probability of a successful SBT (P-score: 0.90). The net was consistent (Q: 0.15) with a low heterogeneity estimate but with high imprecision, indicating an underpowered test (I2 59.9% [1.7−83.7], P = .03). Consistency between direct and indirect evidence can be appreciated on Supplementary Figure 3 (see related supplementary materials at http://www.rcjournal.com). No publication bias was identified (P: .07) (Fig. 2D).

A: Network plot (no. = number of events/n = all subjects). Main characteristics: quantifying heterogeneity/inconsistency: τ2 = 0.0097; τ = 0.0987; I2 = 59.9% [1.7–83.7]. Tests of heterogeneity (total): Q = 12.48; d.f. = 5, P = .03. B: Forest plot (ATC100+PEEP < 7.5 cm H2O is the reference*); only direct comparisons. C: Table of direct (above the interventions diagonal line) and indirect (below the interventions diagonal line) evidence (significant variables are shown in red). D: Funnel plot of publication bias. RR = relative risk.
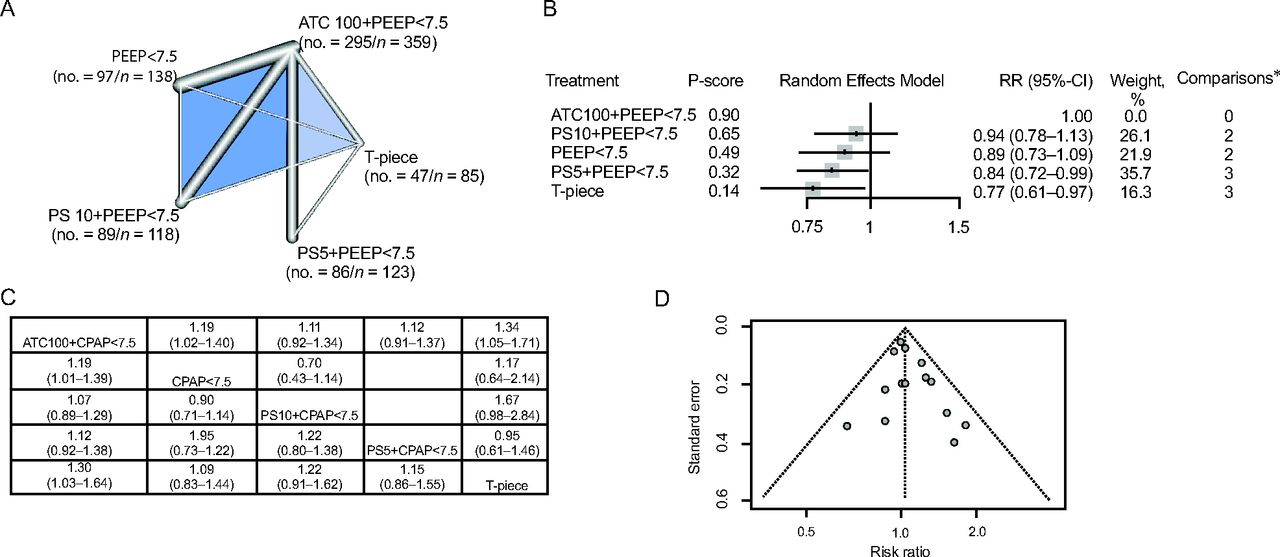
For the extubation outcome, there were 7 studies with 705 participants (Fig. 3A).15-21 Direct and indirect comparisons showed that ATC100+PEEP < 7.5 was significantly better than PEEP < 7.5 and T-piece (Fig. 3B and D). Likewise, ATC+PEEP < 7.5 was the intervention with the highest probability of successful extubation (P-score: 0.90). The net was consistent (Q: 0.20) with low heterogeneity estimate but high imprecision (I2 27.6% [0−68.7], P: .22). Consistency between direct and indirect evidence can be appreciated on Supplementary Figure 4 (see related supplementary materials at http://www.rcjournal.com). No publication bias was identified (P: .17) (Fig. 3D).

A: Network plot (no. = number of events/n = all subjects). Main characteristics: quantifying heterogeneity/inconsistency: τ2 = 0.0076; τ = 0.0874; I2 = 27.6% [0–68.7]. Tests of heterogeneity (total): Q = 8.28; d.f. = 6, P = .22. B: Forest plot (ATC100%+PEEP < 7.5 cm H2O is the reference*); only direct comparisons. C: Table of direct (above the interventions diagonal line) and indirect (below the interventions diagonal line) evidence. D: Funnel plot of publication bias. RR = relative risk. Significant values are shown in red.
The analysis of days on mechanical ventilation included 3 studies with 220 subjects.17,18,21-23 Direct and indirect comparison showed that ATC100+PEEP < 7.5 was associated with more days in mechanical ventilation than PEEP < 7.5 (Supplementary Fig. 5, see related supplementary materials at http://www.rcjournal.com). The net was consistent (Q: 0.42) with low heterogeneity (I2 0% [0−88], P: .42). No publication bias was identified (P: .17).
Discussion
This is the first NMA reported on the performance of ATC to assist weaning from mechanical ventilation. The main findings of the present study are that (1) PS10+PEEP < 7.5 was associated with the highest probability of a successful SBT and (2) ATC+PEEP < 7.5 was associated with the highest probability of extubation success.
At the bedside, it is of paramount importance to identify patients who are potential candidates for extubation. Using ATC+PEEP < 7.5 was associated with a lower rate of a successful SBT but a higher rate of successful extubation. The objective of an SBT is to simulate the conditions of spontaneous breathing without an artificial airway. ATC theoretically compensates for artificial airway resistance, whereas PS provides ventilatory assistance that can facilitate SBT success while reducing patient effort.
While the majority of patients only require simple weaning,3,24 some fail their first attempt at ventilator liberation. In patients who are difficult to wean, providers should first assess the mechanism for that to occur and in particular the imbalance between the loads imposed to the respiratory muscles and the efficiency of them to provide an adequate work of breathing in synergy with the other components of the ventilatory pump. Another strategy to prevent difficult weaning is to minimize the work of breathing.
ATC was more frequently used than expected in a declarative survey,25 with > 60% of the respondents claimed they used it. Interestingly, quite a large number of trials comparing ATC to other weaning modes have been performed outside Western countries. On the bench, we assumed that the delivered tidal volume (VT) is comparable without ATC and regardless of ETT size,25 and this is what was found in modern ICU ventilators. A reduction in work of breathing on the bench with ATC was previously found with older ICU ventilators.26 We found substantial use of ATC in the ICU and reliable ventilator performance using this feature but low quality of trial evidence. Thus, research should be conducted to test ATC as a weaning method against the current standard using low levels of PS or CPAP. Among the arguments against ATC, one is that the equation used to compensate for the resistive pressure drop across the ETT is for new tubes and may be less accurate in used tubes after several days under invasive mechanical ventilation with accumulation of secretions in the distal parts of the tube, reducing its lumen and increasing its flow resistance.27 However, on the bench when ATC was set for an 8-mm internal diameter tube and a 7-mm internal diameter tube was used, the delivery of VT was maintained.25 It should be also mentioned that the algorithm for ATC in ICU ventilators does not include the Blasius equation, which is probably the most accurate tool to assess flow resistance across tube.28 Another potential drawback is that ATC, like low-level PS, has been shown to reduce breathing variability compared to T-piece in one study.29 The lack of variability of breathing has been found to be associated with weaning failure.30,31
This study has some weaknesses. First, we only compared studies that included ATC as an intervention. This explains why several manuscripts related to SBT were not been considered. Second, the time elapsed between the first and the last study is 22 years. Despite the potential confounding factors introduced by this time frame, we believe the analyzed outcomes are robust enough to support our conclusions. Third, ATC was delivered by different ventilators applying various algorithms. However, our recent bench data showed that ICU ventilators performed very close to adequately with ATC.29 Fourth, there is an intrinsic limitation of NMA: there is no direct randomization of comparison groups, and we relied on an assumption of homogeneity that cannot be reliably demonstrated and thus may have led to bias. Evidence provided should thus be rated as observational.32 Thus, our findings although based on a robust methodology can provide only a contribution to evidence in this field that needs further confirmation.
Conclusions
ATC could improve the rate of extubation success but was not the best in term of SBT success.
Footnotes
- Correspondence: Claude Guérin MD PhD, Service de Médecine Intensive-Réanimation, 5 Place d’Arsonval 69003 Lyon, France. E-mail: claude.guerin{at}chu-lyon.fr
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2022 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}