

Abstract
BACKGROUND: Community-based pulmonary rehabilitation (PR) programs can be offered to patients with COPD, but the literature on its effects is still not well summarized. Our purpose was to investigate the health-, physical-, and respiratory-related effects of community-based PR in individuals with COPD as compared to control groups.
METHODS: The PubMed and Embase databases were searched up to May 17, 2021. We included randomized control trials that compared the effects of community-based PR as compared to control groups in individuals with COPD. The risk of bias was judged using the Cochrane Risk of Bias 2 (RoB2). Meta-analysis was performed using a random-effects model to estimate the standardized mean difference (SMD) with 95% CI of the mean changes from baseline between groups. The Grading of Recommendations Assessment, Development, and Evaluation was used to interpret certainty of results.
RESULTS: We included 10 randomized control studies comprising a total of 9,350 participants with weighted mean age of 62.3 ± 2.38 y. The community-based interventions were based on exercise programs (resistance and/or endurance). All studies were judged as high risk and/or some concerns in one or more domains the risk of bias. All meta-analyses displayed very low certainty of evidence. The community-based PR interventions were significantly superior to control interventions in improving the St. George Respiratory Questionnaire Activity subscore (−0.40 [95% CI −0.72 to −0.08]; k = 5, n = 382) and total score (−0.73 [95% CI −1.29 to −0.18]; k = 4, n = 268) and the Chronic Respiratory Disease Questionnaire dyspnea subscore (0.36 [95% CI 0.03–0.69]; k = 6, n = 550). The mean changes from baseline were not different between the groups for all other outcomes.
CONCLUSIONS: Community-based PR tended to result in superior health-related quality of life and symptoms than control interventions, but the findings were inconsistent across outcomes and with very low certainty of evidence. Further studies are warranted for stronger conclusions.
Introduction
COPD is a multifactorial progressive chronic respiratory noncommunicable disease. Dyspnea, productive coughing, and production of sputum are the most frequent respiratory symptoms and are associated with higher risk of exacerbations, hospitalizations, and poorer outcomes.1,2 Although COPD is not fully reversible, pulmonary rehabilitation (PR) plays a key role in managing COPD-related respiratory symptoms, prevents and treats exacerbations; slows down the disease progression; improves exercise tolerance, physical function, and autonomy; decreases the risk of chronic comorbidities; and ultimately improves the health-related quality of life.3-8
The structure design (content and settings) and health care professionals involved in PR programs vary according to cultural context, health care systems, and resources available.9 Most studies have been conducted in a hospital-based10-13 or home-based14-23 setting, with fewer studies in community-based settings. Community-based PR programs are developed in a nonspecialized community health service, in a community center, or at the patient's home.24 The community-based PR programs differ from home-based interventions as the PR component of the program is supervised by a trained health care professional rather than performed at home without any supervision. Community-based PR programs can be offered to patients with COPD as an alternative to hospital-based programs and are important to successfully integrate health care interventions that demand the involvement of both patients and family members in care planning, implementation, and monitoring.25,26
The literature on the effects of community-based PR for individuals with COPD is still not well summarized. There are only a few systematic reviews on this topic, but these only include a few trials on community-based PR with searches performed more than 5 years ago24,27 or are focused on community-based self-management interventions.28 The purpose of this systematic review was to investigate the health-, physical-, and respiratory-related effects of community-based PR in individuals with COPD as compared to control groups.
Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement29 and under the guidance of PRISMA in Exercise, Rehabilitation, Sport Medicine, and Sports Science recommendations.30
Eligibility Criteria
The eligibility criteria were set according to the Participants, Intervention, Comparison, Outcome, and Study design framework. Translation services were not available, so we only included studies written in English language.
Population.
We only included studies that comprised individuals with established COPD. Studies comprising mixed populations with respiratory diseases (eg, COPD and asthma) but without provided separate data for COPD participants were excluded. Studies including participants that were only at risk of COPD (not established) were also excluded.
Intervention.
We included studies reporting the results of community-based PR programs. As community-based PR programs, we considered PR interventions were implemented or supervised by a health care professional and that were employed in the community, either in a nonspecialized community health service, in a community center, or at the patient's home.24 Studies that provided supervised community-based PR interventions and that were supplemented by home-based exercises (for maintenance purposes) were considered for inclusion. To be included, the study had to implement an intervention for a minimum of 6 weeks. All studies reporting the results of noncommunity-based PR programs (eg, single exercise, exclusive to home based, hospital based, online or telephone based, ambulatory based) were excluded. Studies that the intervention was only based on education or counseling were also excluded. There was no restriction to who performed the intervention.
Comparator.
As comparator group to the PR, we considered groups with usual care, self-management, or wait and see (no intervention). Other noncommunity-based PR programs (eg, hospital based or ambulatory based) were not considered as comparator group because our goal was to compare the community-based PR intervention to a homogenous comparator group without PR intervention.
Outcome.
As outcomes, we considered all health-, physical- and respiratory-related outcomes after PR intervention as previously described.31 Further description of these outcomes is further detailed on data extraction subsection.
Study design.
We only included randomized control trials with at least 10 participants per group. Other types of studies were excluded (reviews, nonrandomized cohort studies, observational, case-control and cross-sectional studies, case series, case studies, qualitative studies). Conference abstracts were also excluded.
Search Strategy
A systematic electronic literature search was conducted on PubMed and Embase databases. All searches were performed independently by 2 authors (MB and RA) from database inception up to in May 17, 2021. The full search strategy for each database is described in Supplement 1 (Supplement 1, see related supplementary materials at http://www.rc.rcjournal.com). The reference list of included studies and other relevant reviews was scanned for other potential eligible studies.
Study Selection
All records were exported to EndNote X7 (Thomson Reuters, Toronto, Ontario, Canada), and the duplicate records were removed using the software automated tool and hand checked for any duplicate records. Two authors (MB and RA) independently scanned all titles and abstracts and identified all potentially relevant studies that required further analysis. The full text of all the potentially relevant studies was analyzed according to the eligibility criteria. Disagreements between the 2 authors on study selection were resolved by consensus.
Data Extraction
Two authors (MB and RA) independently extracted all data; disagreements were discussed until consensus. We used an Excel spreadsheet to record data related to (1) study characteristics (study design and country), (2) population characteristics (sample size, mean age, female/male ratio, FEV1, COPD classification, and smoking status), (3) intervention characteristics (type, frequency, duration and setting of intervention, adherence to the intervention, who performed the intervention, and comparator group), and (4) the baseline and post-intervention outcomes (health, physical, and respiratory related). The intervention outcomes were further categorized into domains.31 Physical-related measures comprised exercise capacity, functional capacity, peripheral muscle strength, body composition, and quantification of physical activity. The health-related outcomes included quality of life, symptoms (dyspnea, anxiety, and depression), and mental health and behavior. The respiratory-related outcomes measured expiratory and inspiratory lung function. Exacerbations, hospitalizations, and medication taken were also collected.
Data Management
When the study reported data for the same outcome for several follow-up time points, we used the data from 12-months follow-up (when available); otherwise, we used the closest follow-up time point and analyzed the influence of follow-up in sensitivity analyzes. Studies with overlapping populations reporting the same outcomes but with different follow-ups we used the study that presented the 12-month follow-up. Whenever possible, we used data from the participants compliant to the protocol. Missing data were requested by e-mail to corresponding authors. Missing raw SD was imputed (if possible) using within-group standard errors or confidence intervals as suggested by Cochrane Handbook.32 When data were reported within figures, we used the WebPlotDigitizer software to extract the means and SDs.33 For comparisons of studies with 2 or more intervention groups, we divided the sample size of the control group proportionally to the sample size each intervention group to eschew overweighting the data synthesis with the same group sample.34 Population characteristics are presented as pooled means and SDs weighted to the sample size (if continuous variables)35 or pooled rates (if dichotomous or categorical variables).
Risk of Bias
The risk of bias was assessed using the revised Cochrane Risk of Bias 2 (RoB2) tool.29,30,36 This RoB2 appraises 5 different domains of bias that arise from (1) randomization process, (2) deviations from intended interventions, (3) missing outcome data, (4) measurement of outcomes, and (5) selection of the reported result. Two authors (MB and RA) judged each domain as “low risk of bias,” “some concerns,” or “high risk of bias.” The overall risk of bias judgment was based on the bias judgment from the 5 domains.
Data Synthesis
Quantitative synthesis (meta-analysis) was conducted on RStudio 3.3.1 software (RStudio, Boston, Massachusetts) using the “dmetar,” “meta,” and “metafor” packages. Meta-analyses were performed when there were 3 or more comparable studies for the same outcome. A random-effects model (Sidik-Jonkman estimator with Hartung-Knapp adjustment37) was used due variations in community-based PR interventions and specific methods of outcome collection/scoring. Continuous outcomes are expressed as standardized mean differences (SMDs) with their 95% CI. The SMD magnitude was interpreted as large (≥ 0.8), moderate (0.5–0.79), or weak (0.2–0.49).38 The mean change from baseline was used for all meta-analyses. When studies did not provide the mean and SD of changes from baseline, we computed the mean change from baseline to estimate the mean improvement assuming a correlation coefficient of r = 0.5 to calculate the SD of mean changes.39 The level of statistical heterogeneity for pooled data was established using I-squared statistics, which is interpreted as not important (< 50%), moderate (50–75%), and high (> 75%).40
Sensitivity analyses were performed by removing studies with (1) a follow-up time point that is different from 12 months, (2) a control group that is different from usual care, and (3) outlier results (the 95% CI of study did not cross the 95% CI of the pooled effect). Further sensitivity analyses were performed by using correlation coefficients of r = 0.3 and r = 0.7 to test the effect of this coefficient in the pooled effect. The risk of publication bias was assessed by inspecting the funnel plots for symmetry and with the Eggers test41 if there were 10 or more studies for the same meta-analysis.
Certainty of Evidence
Two authors (MB and RA) rated the certainty of evidence using the Grading of Recommendations Assessment, Development, and Evaluation approach.42 Certainty of evidence was graded as high, moderate, low, or very low certainty. Certainty was downgraded if there were concerns with risk of bias, inconsistency, imprecision, and indirectness. Publication bias could not be reliably assessed (no meta-analysis had 10 or more studies), and no study was downgraded due to risk of publication bias.
Results
Study Selection
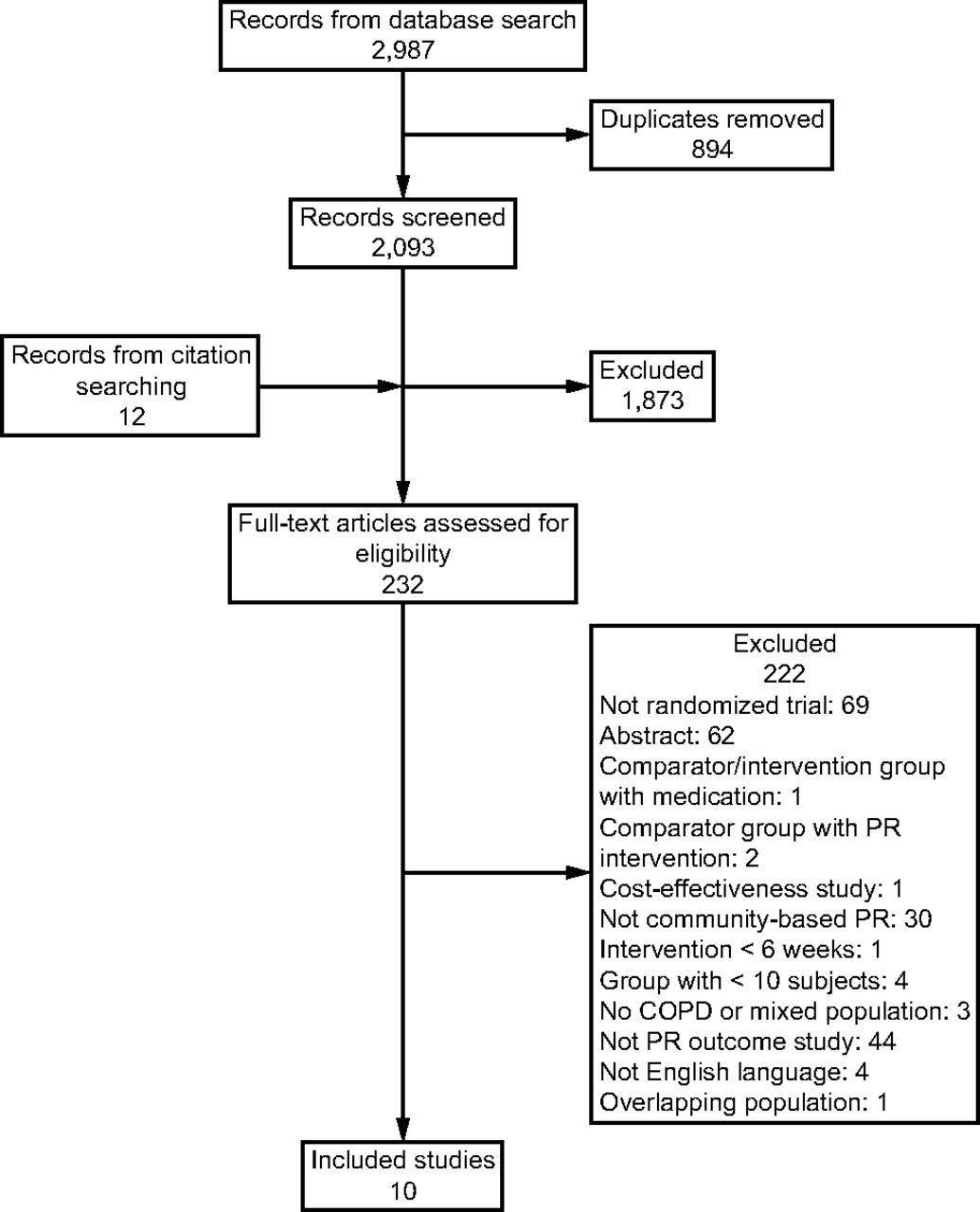
The database searches yielded a total of 2,987 results. Following duplicates removal, there were 2,093 unique records, of which 221 full texts were selected for further analysis. Hand searches yielded another 12 records. A total of 10 studies43-52 fulfilled the eligibility criteria and were included for qualitative analysis (Fig. 1). The majority of the studies was performed in Europe (80%).

Flow chart. PR = pulmonary rehabilitation.
Risk of Bias
All randomized control trials were judged as high risk (80%) or some concerns (20%). No study was judged with an overall low risk of bias (Fig. 2). Nearly all studies (90%) were judged with low risk of selection bias arising from randomization process. Most studies (70%) were judged with some concerns regarding performance bias due to deviation from intended interventions, with 2 studies judged with high-risk bias in this domain. The most common concerns for risk of performance bias were related inability to blind of participants or caregivers implementing the interventions because interventions were exercise based and some deviations that occurred due to the trial context. Risk of attrition bias was also common (50% of studies with high risk and 20% with some concerns) that was related to high rates of dropout and/or loss to follow-up. Four studies (40%) also showed some concerns for detection bias as these studies failed to blind the outcome assessor. More than half of the studies was judged with high risk (30%) or some concerns (40%) for risk of selective reporting bias.

Risk of bias judgment using the Cochrane Risk of Bias 2 tool. A: Domain-based risk of bias for each included study. B: Unweighted summary of risk of bias for each domain across studies.
Population Characteristics
There was a total of 9,350 participants with weighted mean age of 62.30 ± 2.38 y, with a homogenous age distribution among groups (62.30 ± 2.12 y for intervention group and 62.20 ± 2.50 y for control group). The overall sample was homogenous according to sex (4,687 males and 4,663 females). The median sample size was 125 participants but ranged from 26–8,217 participants (Table 1).
Characteristics of Included Studies and Population
The weighted mean FEV1 predicted (%) was 26.7 ± 10.3, which was similar between intervention and control groups (26.7 ± 10.1 and 26.7 ± 10.4, respectively). Around half of participants (56%) had history of smoking (either current or ex-smokers). Two studies43,48 did not report the percentage of participants that was smokers.
Intervention Characteristics
All interventions were community-based exercise programs (resistance and/or endurance), with 3 studies44,47,50 supplementing the intervention with specific PR breathing exercises. Interventions were delivered by physiotherapists (7 studies), nurses (3 studies), fitness instructors (2 studies), or a combination of health care providers (1 study). Interventions ranged from daily to 1 session per week, with a duration of 30–120 min per session (Table 2). Two studies44,46 tailored the exercise programs to participants’ needs. The total duration of interventions ranged from 6 weeks–2 y, with 4 studies45,50-52 supplementing the main intervention (compulsory) with further months of home-based intervention for maintenance (optional). Adherence to the intervention protocol varied from 36.1–95.6%, with 3 studies46,49-51 not reporting the adherence rate. The setting was heterogenous across studies, but the majority of studies recruited participants from primary care services (referral from hospital). As comparators, most studies (80%) employed a control group with only usual care (without any further interventions), and 2 studies45,52 applied a self-management program.
Characteristics of Intervention and Control Groups
Outcome Measures
Thirty-eight different outcomes and measures were reported among the included studies, which were categorized within 12 different domains (Table 3). Exercise capacity (90%), health-related quality of life (90%), and symptom-related measures (60%) were the most commonly reported domains. Exacerbations (40%), hospitalizations (50%), and medication (30%) were also frequently reported.
Characterization of Post-Intervention Outcomes and Measures Grouped by Outcome Domain
Follow-up time points ranged from 6 weeks–48 months. The most common follow-up time points were 3 months (4 studies) and 12 months (5 studies). Other reported time points included 6 weeks (1 study), 4 months (1 study), 6 months (1 study), 7 months (1 study), 24 months (2 studies), and 48 months (1 study).
Data Synthesis
A total of continuous 11 outcomes was eligible for meta-analysis from 4 different domains: exercise capacity, health-related quality of life, symptoms, and lung function. Only 3 outcomes from the health-related quality-of-life domain, St. George Respiratory Questionnaire (SGRQ) activity subscore, SGRQ total score, and Chronic Respiratory Disease Questionnaire (CRQ) dyspnea subscore, were significant different between intervention and control groups when comparing the mean change from baseline to follow-up (Fig. 3). The community-based PR interventions were significantly superior to control interventions in improving the SGRQ activity subscore (SMD −0.40 [95% CI −0.72 to −0.08]; weak effect and very low certainty), SGRQ total score (SMD −0.73 [95% CI −1.29 to −0.18]; moderate effect and very low certainty), and CRQ dyspnea subscore (SMD 0.36 [95% CI 0.03–0.69]; weak effect and very low certainty). For all other outcomes, the mean changes were not statistically different between the groups (Table 4 and Supplement 2, see related supplementary materials at http://www.rc.rcjournal.com).

Forest plots for statistically significant outcomes comparing community-based pulmonary rehabilitation (PR) and control interventions. A: St. George Respiratory Questionnaire (SGRQ) total score: A negative standardized mean difference (SMD) indicates superior improvement for the community-based PR group. B: SGRQ activity subscore: A negative SMD indicates superior improvement for the community-based PR group. C: Chronic Respiratory Disease Questionnaire dyspnea subscore: A positive SMD indicates superior improvement for the community-based PR group.
Quantitative Synthesis of the Comparison of Intervention and Control Groups for Post-Intervention Outcome Mean Changes
More than one-third of the meta-analyses displayed statistically significant heterogeneity (36%). When analyzing the sensitivity analyses using 0.3 and 0.7 as correlation coefficients (Supplement 3, see related supplementary materials at http://www.rc.rcjournal.com), the heterogeneity did not change significantly in almost all analyses; only the CRQ mastery outcome changed to significant heterogeneity using the 0.7 correlation coefficient. Using the 0.3 correlation coefficient did not yield any influence on the effect sizes, but when using the 0.7 value, only the SGRQ total score was statistically significant between groups. Sensitivity analyses by removing studies outside the 12-month follow-up end point tended to slightly decrease the heterogeneity figures (Supplement 4, see related supplementary materials at http://www.rc.rcjournal.com), but whereas the intergroup differences on CRQ dyspnea outcome remained statistically significant, the SGRQ total score was not different between groups. Sensitivity analyses by removing studies with self-management control group produced no discernible changes in heterogeneity, but no outcome remained statistically different between groups. We also performed sensitivity analysis by removing the study Lou et al47 with a high sample size (overrepresented in meta-analyses), but no significant changes were seen in the pooled effect size.
Exacerbations, hospitalizations, and intake of medication were poorly reported across studies. Three studies reported the rate of exacerbations, with one study49 showing a lower rate for the community-based PR group and 2 studies43,50 showing a comparable rate between community-based PR and usual care groups. Four studies43,47,48,50 reported the rate of hospitalizations, with a trend to a higher rate in the usual care group. Three studies46,47,50 reported the rate of medication intake showing inconsistent findings across studies when comparing the community-based PR and usual care groups (Table 5).
Rates of Exacerbations, Hospitalizations, and Intake of Medication
Discussion
The main finding of our systematic review with meta-analysis is that community-based PR interventions tended to result in superior improvements in health-related quality of life and symptoms (dyspnea) than control interventions. These findings are clinically relevant as dyspnea is a frequent respiratory symptom in patients with COPD and is associated with higher risk of exacerbations, hospitalizations, and poorer outcomes.1,2 Therefore, in addition to improving the health-related quality of life, community-based PR interventions can decrease the symptoms of dyspnea and the risk of exacerbations and the need for hospitalization. These implications will ultimately result in a significant socioeconomic impact for patients with COPD and reduce the load of hospital resources.55-58
Our findings should, however, be interpreted with some caution. The results from meta-analyses were inconsistent across outcomes, with significantly superior effect in the community-based PR group for only 3 of the 11 outcomes analyzed. The certainty of evidence was judged as very low for all outcomes, and most studies show an overall high risk of bias. Although there were significant superior effects for the community-based PR group at the SGRQ activity subscore, SGRQ total score, and CRQ dyspnea subscore, the effect ranged from weak to moderate. The findings of the quantitative syntheses often showed conflicting and imprecise results, with the pooled SMD crossing either or both the −0.5 and 0.5 effect size. When analyzing the results in sensitivity analyses, some of the findings were no longer statistically significant, especially when removing the studies with a self-management control group.
Over the last 5 years, there have been several systematic reviews that underpin positive effects of exercise-based PR (either supervised or unsupervised)14,27,59-80 or respiratory exercises79,81-83 on several health-related outcome domains in subjects with COPD. However, none of the previous systematic reviews focused community-based PR interventions, and the majority of their meta-analysis findings were reported without informing the degree of certainty of evidence. There is a previous systematic review28 of randomized control trials that found no significant effect in health-related quality of life outcomes for community-based PR interventions. However, this systematic review28 only included community-based self-management interventions, which was not considered in our systematic review. Our systematic review focused on community-based PR interventions that were led by a trained health care professional or fitness instructor. Nevertheless, although we found a significant effect for SGRQ activity subscore, SGRQ total score, and CRQ dyspnea subscore, other outcomes were not significantly superior as compared to control groups, which is in line with the previously mentioned systematic review28 that found no significant differences.
The rate of exacerbations was comparable between the community-based PR and control interventions, whereas the need for medication showed inconsistent findings. Only the rate of hospitalizations seems to be reduced in the community-based PR group. Only a few studies analyzed these outcomes, which were heterogeneously collected and reported and thus not allowing any sound conclusions. Future studies must consider collecting these outcome events and reported them in a more standardized fashion to allow a clearer picture. The literature on this topic is still not conclusive, and further research is warranted. Reducing the risk of hospitalization is important in patients with COPD because a recent hospitalization (in the previous year) is a primary risk factor for further COPD-related readmissions.84 Implementing PR interventions that start no longer than 3 weeks after hospital discharge from an acute COPD exacerbation or that add an educational component to exercise program seem to be more effective in reducing the rate of hospital readmissions.12
The heterogeneity in the outcomes and measures reported among the included studies was another concern, which is also seen in other systematic reviews.31,85-88 There is a clear need to standardize a set of core outcomes to measure the improvement of individuals with COPD following PR interventions.31 Future studies should assess the importance of each outcome for PR involving different stakeholders and decide on which are the outcomes with higher priority. The follow-up time points to assess patient improvement also varied considerably across included studies. Future research should focus on standardizing the follow-up time points, very short-term, short-term, midterm, and long-term follow-up, to allow a more direct and valid comparison between studies. The use of a comparable and interchangeable outcome throughout the studies would allow to reach a more consistent recommendation in future systematic reviews with meta-analysis to answer if the community-based PR programs are superior in improving the health-related quality of life and symptoms in patients with COPD.
There are some limitations that need to be acknowledged. Although we excluded studies with home-based PR interventions, some of the included studies implemented a component of home-based exercises. However, the home-based component of the included studies was intended only as reinforcement or maintenance to the main community-based program. We intended to perform subgroup analyses stratified by grade of COPD, but the included studies did not provide their results separately according the COPD grading. We expected to stratify the meta-analyses according to the categorization of follow-up duration (very short term, short term, midterm, and long term), but there were not enough studies (at least 3 studies for the same outcome and same follow-up time point) besides the 12-month time point; therefore, we undertook the meta-analyses with the 12-month follow-up (or the closest follow-up time point) and then analyzed the effect of follow-up in sensitivity analysis, which effects were negligible. We also intended to test for the risk of publication bias, but as the meta-analyses included fewer than 10 studies, it was not reliable to use the funnel plots or the Egger test; the results should thus be interpreted with caution because the risk reporting bias could not be evaluated. There were covariates that could be analyzed in a meta-regression analysis (duration and adherence to the intervention), but given the small number of studies, the meta-regression is likely underpowered. The use of minimally clinical important difference (MCID) cutoffs would improve the applicability of our findings, but as we used the SMDs instead (due to the heterogeneity across studies), the use of MCID values was not possible; however, the SMDs are translated into effect sizes that showed weak to moderate effects. A moderate effect size (SMD > 0.5) has been suggested to approximate, in most cases, to the MCID.89 There were only a few studies that reported the rates of exacerbations, hospitalizations, and intake of medication; and the way these outcomes were collected was not comparable across included studies, which precluded us from meta-analyzing the relative risk of these outcomes comparing community-based PR versus usual care. We thus decided to analyze these outcome as simple rates. Another limitation was that some studies had considerable dropout rates and did not report separately the baseline outcome data for those subjects who finished the trial; in these studies, when calculating the improvement for the meta-analyses, we used the total sample for the baseline outcome and the participants that were adherent to the protocol (or that did not drop out) for the outcome follow-up.
Conclusions
Community-based PR interventions tended to result in superior health-related quality of life and symptoms than control interventions, but the findings were inconsistent across outcomes and with very low certainty of evidence. A superiority of community-based PR over usual care could still not be established, and future studies are needed to strengthen the evidence on community-based PR interventions in patients with COPD. There were, however, some significant findings that should encourage the investment of resources into researching and improving strategies of community-based PR interventions. Further studies are warranted for stronger and more definitive conclusions.
Footnotes
- Correspondence: Marisela Barbosa MSc. E-mail: mariselabarbosa{at}gmail.com
Supplementary material related to this paper is available at http://rc.rcjournal.com.
The authors have disclosed no conflicts of interest.
This work was primarily performed at Faculty of Sports, University of Porto, Porto, Portugal.
- Copyright © 2022 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.↵
- 4.
- 5.
- 6.
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.↵
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.
- 22.
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.
- 54.
- 55.↵
- 56.
- 57.
- 58.↵
- 59.↵
- 60.
- 61.
- 62.
- 63.
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.↵
- 80.↵
- 81.↵
- 82.
- 83.↵
- 84.↵
- 85.↵
- 86.
- 87.
- 88.↵
- 89.↵





{kind=link}
{kind=link}
{kind=link}