

Abstract
BACKGROUND: Patients with ARDS due to COVID-19 may require tracheostomy and transfer to a weaning center. To date, data on the outcome of these patients are scarce. The objectives of this study were to determine the factors associated with time to decannulation and limb-muscle strength recovery.
METHODS: This was an observational retrospective study of subjects with COVID-19–related ARDS requiring tracheostomy after prolonged ventilation, who were subsequently transferred to a weaning center from April 4, 2020–May 30, 2020.
RESULTS: Forty-three subjects were included. Median age (interquartile range) was 61 (48–66) y; 81% were men, and median body mass index (BMI) was 30 (26–35) kg/m2. Tracheostomy was performed after a median of 19 (12–27) d of mechanical ventilation, and the median ICU length of stay prior to transfer to the weaning center was 30 (21–46) d. On admission to the weaning center, the median Medical Research Council (MRC) score was 36 (27–44). Time to decannulation was 9 (7–18) d after admission to the weaning center. The only factor independently associated with early decannulation was the MRC score on admission to the weaning center (odds ratio 1.16 [95% CI 1.06–1.31], P = .005). Two factors were independently associated with MRC gain ≥ 10: BMI (odds ratio 0.88 [95% CI 0.76–0.99], P = .045) and MRC on admission (odds ratio 0.91 [95% CI 0.82–0.98], P = .03. Three months after admission to the weaning center, 40 subjects (93%) were weaned from mechanical ventilation and 36 (84%) had returned home.
CONCLUSIONS: MRC score at weaning center admission predicted both early decannulation and limb-muscle strength recovery.
Introduction
Among patients hospitalized for coronavirus disease 2019 (COVID-19), 15–22% require transfer to the ICU. Eighty percent of patients in this population require invasive mechanical ventilation,1-6 and most of them meet the criteria of ARDS. The median duration of mechanical ventilation among survivors is 10–16 d2-3 with a median ICU length of stay of 16 d.4
This prolonged duration of mechanical ventilation may induce chronic critical illness, including loss of muscle strength, persistent ventilator dependence, and extubation failure.7,8 These clinical features are not uncommon in patients with COVID-19.9 The ICU length of stay is increased in this subgroup, which is potentially responsible for decreased availability of ICU beds, possibly leading to ICU saturation, which can constitute a major problem in the context of a pandemic. For these various reasons, and also because of heterogeneous local practices, some patients may require tracheostomy. Recent cohort studies in subjects with COVID-19 report tracheostomy rates ranging from 9–50%, depending on ICU resources and country.4,10-11 Due to the complex management of weaning in tracheostomized patients after ARDS, and also due to ICU-acquired weakness, some of these individuals are ultimately managed in a weaning and rehabilitation center.12,13
The prognostic factors associated with ICU survival in patients with COVID-19–related ARDS have now been well described, but only limited data are available on the duration of weaning and the recovery of ICU-acquired weakness in this patient population, who required tracheostomy and who were finally transferred to a weaning center.14 A better understanding of these key recovery outcomes may improve the quality of triage and management decisions.
In this article, we report our experience on trajectory of tracheostomized subjects admitted to a weaning center following COVID-19–related ARDS. The primary objective was to identify factors associated with early decannulation. Our secondary objective was to identify the trajectory of limb-muscle strength recovery and associated factors. We hypothesized that Medical Research Council (MRC) score at weaning center admission was associated with both weaning and rehabilitation outcomes. We also described the outcomes of these subjects 3 months after admission to the weaning center.
QUICK LOOK
Current Knowledge
In France, 10% of patients with coronavirus disease 2019 (COVID-19)–related ARDS will require tracheostomy and weaning center admission. France is currently facing its fourth epidemic wave, but no data exist on the management and outcomes of these patients after admission to specialized weaning centers. More specifically, there are not data on factors associated with time to decannulation and limb-muscle strength recovery of patients with COVID-19–related ARDS requiring tracheostomy.
What This Paper Contributes to Our Knowledge
Three months after weaning center admission, 93% of subjects was weaned from mechanical ventilation and 84% of subjects had returned home. Medical Research Council (MRC) score on weaning center admission predicted early decannulation, whereas body mass index and MRC on weaning center admission predicted limb-muscle strength recovery
Methods
Design and Settings
This retrospective observational cohort study was carried out in a 12-bed weaning center in Paris, France. The weaning center is part of the medical ICU and Respiratory Division, located in a 1,600-bed university hospital. There are 3 weaning centers in the greater Paris area. This weaning center (about 200 admission per year) is devoted to weaning from mechanical ventilation, decannulation, refeeding, motor rehabilitation, and global management of chronic critical illness. Patients receive adapted nutritional care provided by a dedicated dietitian. Several physiotherapists equipped with specific tools work daily to promote early mobilization of patients admitted from ICUs with persistent ventilator dependence and ICU-acquired weakness. Therefore, these patients simultaneously receive muscle rehabilitation and progressive ventilator weaning. Mechanical ventilation weaning was defined as the first day of definitive withdrawal without reconnection in the ventilator. Figure S1 describes the mechanical ventilation weaning protocol, and Figure S2 (see related supplementary materials at http://www.rcjournal.com) describes the decannulation protocol used in this unit.
This study was approved by the Sorbonne University Ethics Committee (CER-SU 2020–96), and subjects or their relatives gave their informed consent. Reporting of this retrospective study followed the guidelines for Strengthening the Reporting of Observational Studies in Epidemiology Statement.
Subject Selection.
Subjects were included in the study if they (1) had been invasively mechanically ventilated in an ICU for laboratory-confirmed SARS-CoV-2–related ARDS according to the Berlin definition,15 (2) had been tracheostomized during their ICU stay, and (3) were transferred to the La Pitié-Salpêtrière Hospital weaning center between April 4, 2020–May 30, 2020. There were no exclusion criteria; thus, all consecutive subjects admitted during the study period were included. Laboratory confirmation of SARS-CoV-2 was defined as positive real-time reverse transcriptase-polymerase chain reaction assay of nasal and pharyngeal swabs. Patients < 18 y old and pregnant women were excluded.
Data Collection.
Data were retrospectively analyzed from the subjects’ electronic medical records. Demographic data consisted of age, gender, body mass index (BMI), and underlying diseases, such as hypertension, diabetes, and immunosuppression (defined as neutropenia below 1,000/mm3, malignancy treated by cancer chemotherapy, immunosuppressive therapy for solid-organ transplantation, corticosteroid therapy at doses of 20 mg or more per d for at least 3 weeks, or acquired immunodeficiency syndrome). The following data on the ICU stay were collected: Simplified Acute Physiology Score (SAPS) II,16 blood urea, and PaO2/FIO2 on admission. According to the Berlin definition, severity of the ARDS was based on the lowest PaO2/FIO2 during the first 24 h after intubation.15 Adjunctive therapy such as neuromuscular blockers and prone positioning, life support therapy such as extracorporeal membrane oxygenation and renal replacement therapy, occurrence of ventilator-associated pneumonia, duration of mechanical ventilation prior to tracheostomy, and ICU length of stay were also collected. Finally, we recorded the following data on admission to the weaning center: SAPS II,16 weight loss,17 PaO2/FIO2, blood urea, and albumin. Limb muscle strength, as assessed by the MRC score, was measured on admission to the weaning center and at discharge by trained physiotherapists. Subjects did not receive any sedative drugs and had to be able to cooperate. ICU-acquired weakness was defined by an MRC score < 48 (19–20). Finally, the following parameters were collected: time to decannulation, duration of mechanical ventilation, and weaning center length of stay. Subjects were followed for a 3-month period from the time of admission to the weaning center to determine predictive factors of early decannulation and mortality.
Statistical Analysis.
Data are expressed as number and percentage (n, %) for categorical variables and as median (interquartile range) for continuous variables. Categorical variables were compared using the chi-square test or Fisher exact test, and continuous variables were compared using the Mann-Whitney test. All tests were 2 sided with a limit of significance of 0.05. Multivariate logistic regression was used to identify factors independently associated with early decannulation, defined as a time from weaning center admission to decannulation < 9 d (median time). Multivariate logistic regression was also used to identify factors independently associated with an increase of the MRC score ≥ 10 points during the weaning center stay.
The multivariate model was built with variables that yielded P values < .20 on univariate analysis and/or that were considered clinically relevant, except for SAPS II that was colinear with urea and age in the prediction model of early decannulation and muscle strength recovery, respectively. A backward stepwise selection procedure was performed with an elimination process based on P values < .05. Adjusted odds ratios of variables present in the final model are presented with their 95% CIs. All analyses were performed with R software version 3.5.2 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Subject Characteristics
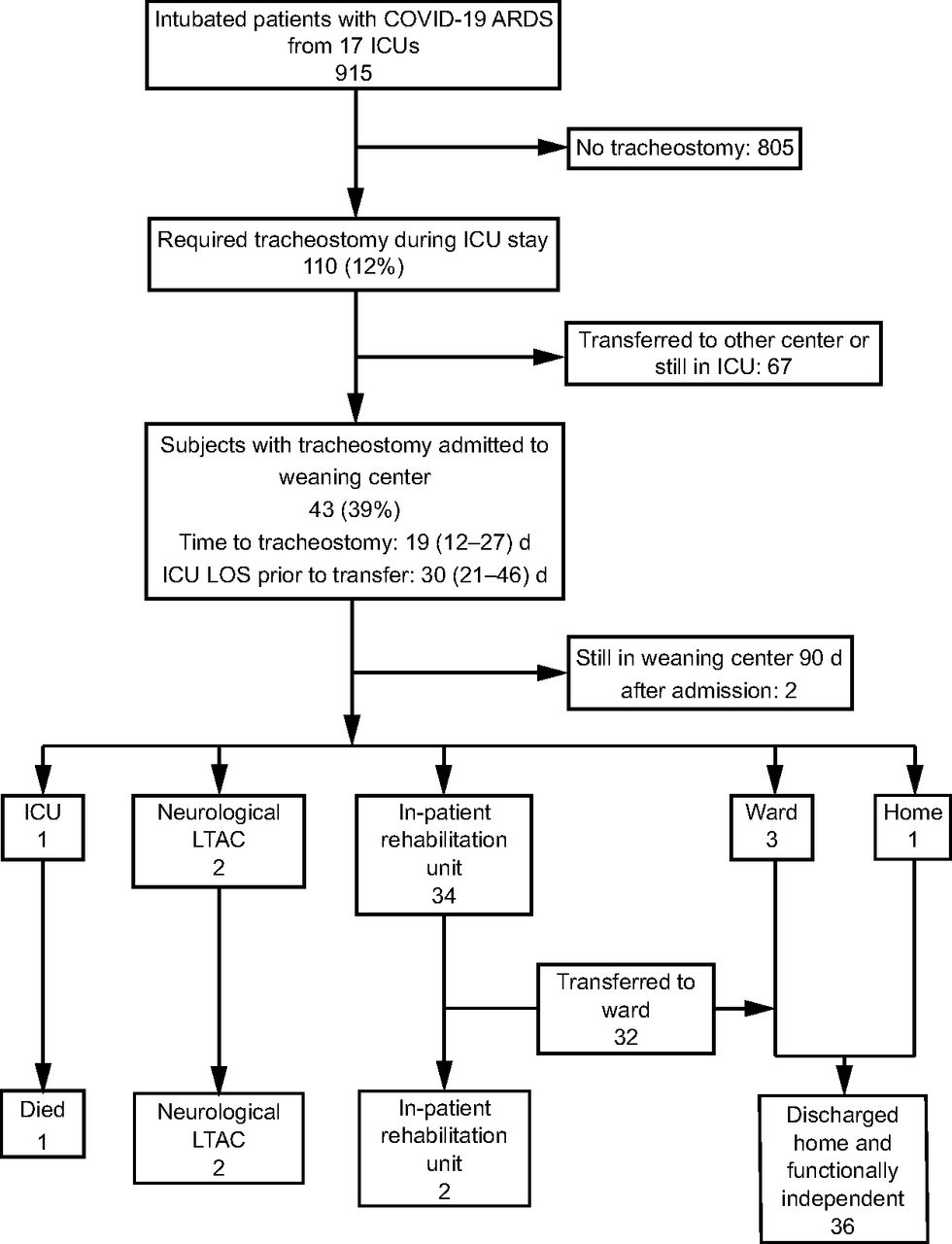
Figure 1 displays the study flow chart. Between March 15, 2020–May 1, 2020, 915 patients were hospitalized in 17 ICUs in the greater Paris area and needed invasive mechanical ventilation for an ARDS due to COVID-19. Among these 915 patients, 110 (12%) required tracheostomy. Among these 110 tracheotomized patients with COVID-19 ARDS, 43 subjects (39%) were transferred to our weaning center. The main subject characteristics are detailed in Table 1. Median age was 61 (48–66) y; 35 (81%) subjects were male, and median BMI was 30 (26–35) kg/m2. Underlying conditions were hypertension in 24 subjects (56%), diabetes in 13 subjects (30%), and immunosuppression in 9 subjects (21%). Median SAPS II on ICU admission was 33 (27–43). ARDS was severe in 11 subjects (26%), moderate in 23 subjects (53%), and mild in 9 subjects (21%). Tracheostomy was performed after a median of 19 (12–27) d of invasive mechanical ventilation, and the median ICU length of stay prior to transfer to the weaning center was 30 (21–46) d (Fig. 2).

Flow chart. LOS = length of stay, LTAC = long-term acute care.
Subject Characteristics and Factors Associated With Time to Decannulation

Subject outcomes: 3-month period after admission to the weaning center.
On admission to the weaning center, median PaO2/FIO2 was 256 (208–329) mm Hg. Median weight loss was 9 (5–12) kg compared to ICU admission, and median blood albumin was 27 (24–31) g/L1. The median MRC score was 36 (27–44), and 31 (81%) subjects had ICU-acquired weakness. Nine subjects (21%) presented signs of brachial plexus injury related to prone position. At discharge of the weaning center, 19 (44%) subjects still had post-ICU–acquired weakness.
Time to Decannulation
The first deventilation session occurred 4 (2–8) d after weaning center admission, and only 3 (7%) subjects were deventilated for the first time in intensive care before weaning center transfer. The median time to decannulation was 9 (7–18) d after admission in weaning center. The total tracheostomy time was 20 (13–33) d. Table 1 shows the factors associated with early decannulation identified by univariate analysis. The only factor identified by multivariate analysis to be independently associated with early decannulation was the MRC score on admission to the weaning center (odds ratio 1.16 [95% CI 1.06–1.30], P = .005).
Gain of MRC Score
The median MRC score at the time of discharge from the weaning center was 48 (43–53) and was established in only 40 patients because of MRC information was missing for 3 patients. The median gain in MRC score during the weaning center stay was 10 (4–16). Table 2 shows the factors associated with ≥ 10-point gain in MRC score identified by univariate analysis. Multivariate logistic regression analysis identified 2 factors independently associated with ≥ 10-point gain in MRC score: BMI (odds ratio 0.88 [95% CI 0.76–0.99], P = .045) and MRC score on admission to the weaning center (odds ratio 0.91 [95% CI 0.82–0.98], P = .03).
Univariate Analysis: Gain of Medical Research Council Score During Weaning Center Stay
More details on multivariate prediction models are provided in the electronic supplement (see related supplementary materials at http://www.rcjournal.com).
Subject Outcome
The median stay in the weaning center was 13 (10–21) d, and the total length of stay from ICU admission to weaning center discharge was 44 (33–65) d. Three months after admission to the weaning center, 36 subjects (84%) had returned home, including one subject who still required noninvasive ventilation due to preexisting obesity hypoventilation syndrome. Six subjects (14%) remained hospitalized, 2 in the weaning center, 2 in a neurological long-term acute care facility, and 2 in an in-patient rehabilitation unit. Two of these 6 subjects were still tracheostomized, but had been weaned from mechanical ventilation, and 2 required nocturnal noninvasive ventilation due to persistent diaphragmatic dysfunction. One subject (2%) died after return to ICU.
Discussion
The main results of the study can be summarized as follows. In tracheostomized subjects with COVID-19 ARDS admitted to a weaning center, (1) decannulation was able to be successfully performed in 50% of cases during the first 9 days following admission, and time of decannulation was strongly influenced by the MRC score at admission; (2) despite a high rate of ICU-acquired weakness, half the subjects gained more than 10 MRC points during their weaning center stay, and this improvement was dependent on BMI and MRC score at admission; and (3) 3 months after weaning center admission, the vast majority of subjects had returned home.
Time to Decannulation
In this study, the median total duration of tracheostomy was 13 d (9 d from weaning center admission) with a median interval between intubation and decannulation of 43 d. These results are consistent with those reported by other authors in subjects with COVID-19–related ARDS requiring tracheostomy.14 However, this duration of tracheostomy or time to decannulation is shorter than that commonly observed in usual weaning centers patients, for which the median duration of tracheostomy is about one month.18-20 There are various possible explanations for this finding. First, the median age in our study was 10 years younger than that usually reported in subjects hospitalized in other weaning centers.18,20-22 Second, subjects with COVID-19 ARDS appeared to present fewer respiratory comorbidities (such as COPD) than non–COVID-19 subjects.21,22 Third, as sepsis is a major risk factor for ICU-acquired limb muscle and diaphragm weakness, the low prevalence of septic shock on ICU admission in subjects with COVID-19 ARDS may partly explain the low prevalence and severity of respiratory and limb muscle weakness, 2 major determinants of weaning success.7,23-27 The neuromuscular consequences could be less severe or may resolve more rapidly in sepsis-free subjects with ARDS. Finally, a recruitment bias was related to the need for high ICU patient turnover, resulting in tracheostomy of individuals who, under normal circumstances, would have been successfully weaned without tracheostomy. It is noteworthy that the tracheostomy was able to be permanently removed in the vast majority of subjects.
The MRC score at the time of admission to the weaning center was the only factor independently associated with time to decannulation. A positive correlation is observed between limb muscle and respiratory muscle strength, which means that patients with adequate muscle strength are more likely to have adequate respiratory muscle strength, a major determinant of weaning success.27 However, decannulation also requires adequate cough,28,29 and ICU-acquired weakness is associated with weak cough.8 In addition, ICU-acquired weakness induces bed rest, which, in turn, promotes atelectasis and hospital-acquired infections including pneumonia,31,32 thus contributing to the vicious circle of prolonged mechanical ventilation.
Higher BMI was associated with lower chance of 10-point MRC gain during the weaning center stay. To the best of our knowledge, this association has never been investigated in the weaning unit setting, but this finding could be put in relation with the muscular dysfunction observed in obese patients (eg, reduced mobility, neural adaptations, and changes in muscle morphology)32 or by the presence of sarcopenic obesity33 in some patients. In other settings, obesity is associated with accelerated muscle strength decline in men34 and functional decline in older adults,35 whereas sarcopenic obesity has been demonstrated to negatively affect poststroke rehabilitation outcome.36
Subject Outcomes
Three months after admission to the weaning center, 93% of subjects were weaned from mechanical ventilation; 98% were alive, and 84% had returned home. To the best of our knowledge, this is the first study to provide a detailed description of the outcome and discharge disposition of tracheostomized COVID-19 ICU survivors. The 3-month mortality rate was much lower in our cohort compared to patients in other weaning centers, who were tracheotomized for reasons other than COVID-19 (2% vs 30%).37,38 Similarly, Unroe et al37 showed that only 10% of subjects had returned home without paid home health care at 3 months.
In the light of these favorable outcomes, tracheostomy should not be discouraged in patients with COVID-19–related ARDS presenting weaning difficulties or extubation failure. Weaning unit length of stay is also usually longer (about 40–50 d) for patients requiring tracheostomy for other causes than COVID-1919,21,37,39 than that observed in subjects with COVID-19 (13 d). This shorter stay suggests more rapid turnover of patients with COVID-19 in weaning centers, which is of critical importance in the pandemic setting.
Finally, half the subjects gained > 10 points in the MRC score during their weaning center stay. Although no specific data are available concerning the minimal clinically important difference of MRC score in post-ICU units, a 10-point gain can be considered to be of practical significance and roughly corresponds to a one-point increase in each lower-extremity muscle group. However, in terms of absolute MRC values, it should be noted that ICU-acquired weakness (defined by an MRC score < 48) had not resolved in 50% of subjects at the time of weaning center discharge. Limb muscle weakness justified transfer from the weaning center to an in-patient rehabilitation unit for a great majority of subjects, emphasizing the fact that patients with severe COVID-19 experience a prolonged negative impact on limb muscle strength, which could be effectively managed in structured care networks.
Limitations
Our study comprises several methodological limitations. First, this study was single-center, but the vast disparity in weaning and decannulation protocol across the 3 weaning centers of the greater Paris area precluded any multi-center design. Second, this was a retrospective study, which involves a potential bias in patient selection or data collection, but our prefilled electronic record limited erroneous or missing data. The study was geographically confined to Paris, which limits its generalizability to other weaning centers in France and in other countries. Third, we did not collect scores assessing quality of life or the degree of functional dependence 3 months after weaning center admission. Finally, our study is probably underpowered to identify other variables associated with the outcomes due to the small sample size of our cohort.
Conclusions
MRC score at weaning center admission was an independent predictor of early decannulation and limb-muscle strength recovery in subjects with COVID-19 who required tracheostomy. Moreover, 3 months after admission to a weaning center, 84% of subjects were alive and had returned home, a much higher rate than that commonly observed in usual weaning center patients. The stay in the weaning center was also shorter. These results suggest that the outcome of these severe and/or complicated forms of COVID-19–related ARDS requiring prolonged ICU stays and mechanical ventilation could be less severe than initially feared. In the uncertain and anxiety-prone setting of the COVID-19 pandemic, these results may be encouraging. However, these favorable outcomes are related specifically to COVID-19 ARDS and cannot be extrapolated to usual ICU population.
Acknowledgments
Physicians, nurses, respiratory therapists, physiotherapists, psychologists, and dieticians of the Pitié-Salpêtrière weaning center for their major collaborative work.
Footnotes
- Correspondence: Maxens Decavèle MD, Service de Pneumologie, Médecine Intensive - Réanimation, Hôpital Universitaire Pitié-Salpêtrière, 47–83 boulevard de l’Hôpital, 75651 Paris Cedex 13, France. E-mail: maxens.decavele{at}aphp.fr
Dr Faure discloses relationships GE Medical System, Pfizer, Bayer Healthcare, and Actelion. Dr Decavèle discloses a relationship with Isis Medical. Dr Dres discloses relationships with BioSerenity and Lungpacer. Dr Mayaux discloses a relationship with Gilead. Dr Caliez discloses a relationship with Oxyvie. Dr Similowski discloses relationships with ADEP Assistance, AstraZeneca France, Chiesi France, GlaxoSmithKline France, Lungpacer Canada, Novartis France, and Teva France. Dr Demoule discloses relationships with Philips, Baxter, Fisher & Paykel, French Ministry of Health, Getinge, Respinor, Lungpacer, Lowenstein, and Gilead. The remaining authors have disclosed no conflicts of interest.
A version of the paper was presented by Dr Morgane Faure at the 2021 French Intensive Care Society International Congress, held in Paris, France, June 9–11, 2021.
The study was performed at Groupe Hospitalier Universitaire APHP-Sorbonne Université, site Pitié-Salpêtrière, Service Médecine Intensive et Réanimation (Département R3S), F-75013 Paris, France.
Drs Decavèle and Demoule are co-first authors.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2022 by Daedalus Enterprises





{kind=link}
{kind=link}