

Introduction
A recent study1 in the United Kingdom with more than 20,000 subjects hospitalized for COVID-19–related acute respiratory failure (ARF) showed that high-flow nasal cannula (HFNC) was the most frequently used (55%) type of respiratory support, followed by noninvasive ventilation (NIV, 16%), whereas invasive mechanical ventilation was used in only 9% of subjects. A randomized controlled trial showed HFNC was beneficial in preventing intubation.2 However, another randomized controlled trial found CPAP as an initial oxygenation strategy was superior to standard oxygen therapy, whereas no differences were found compared to HFNC.3 However, these subjects were not ventilated in the prone position, which may potentiate the effect of NIV in awake subjects.4,5 Ehrmann et al6 recently showed in a multinational meta-trial that awake prone positioning reduced the risk of treatment failure and the need for intubation in subjects receiving HFNC for COVID-19–related ARF.
In this context, early prediction of HFNC outcome may help with management of hypoxemic patients with COVID-19 regarding clinical decisions on optimal setting and magnitude of treatment. The ROX index, corresponding to the ratio of SpO2/FIO2 to breathing frequency, has been validated by Roca et al7 in subjects with ARF and pneumonia under HFNC, outside the COVID-19 context and without prone position. More recently, a few studies evaluated the ROX index in the setting of COVID-19–related ARF since prone position has become a standard of care.8-10 In this observational study, we assessed the performance of the ROX index calculated upon admission and its variation over the first 12 h in the prediction of HFNC failure in subjects with COVID-19–related ARF.
Methods
This was a single-center observational study conducted between September 2020–July 2021. The study received the approval of the institutional review board under as usual care, which waived the need for individual consent.
Study Population
Medical records of subjects age ≥ 18 y consecutively admitted to the medical ICU for confirmed COVID-19 and severe ARF were analyzed. COVID-19 pneumonia was confirmed by positive pharyngeal/nasal swab reverse transcription-polymerase chain reaction. Severe hypoxemic ARF was diagnosed by the presence of dyspnea, tachypnea with breathing frequency ≥ 26 breaths/min, tachycardia, SpO2 ≤ 92% on room air, and a PaO2/FIO2 < 150 mm Hg. Only subjects who received HFNC were included in this study.
Standard medication included dexamethasone (6 mg/d for 10 d), anticoagulation, and tocilizumab following major recommendations for administration to subjects who were not receiving invasive mechanical ventilation.4 HFNC was provided via the Airvo 2 system (Fisher & Paykel, Auckland, New Zealand) and started in supine position with an initial flow between 45–60 L/min. Flow and FIO2 were adjusted as required to fit subject demand and to maintain SpO2 > 94% throughout the treatment period. All subjects were instructed to lie in the prone position if tolerated and to remain in that position as long as possible on a daily basis. If prone position was not tolerated, HFNC was administered in the supine position.
Continuous HFNC was maintained until the subject either clinically improved or worsened. Clinical improvement was defined as an SpO2 consistently > 94% without complaints of dyspnea or clinical signs of distress allowing de-escalation of oxygen therapy to use of a partial rebreathing mask. Clinical worsening and HFNC failure were defined as the need for intubation. Intubation was indicated when at least one of the following occurred: respiratory acidosis (pH < 7.25), severe hypoxemia with SpO2 < 90% despite an FIO2 ≥ 0.8, severe hemodynamic instability, or deteriorating consciousness level.
The duration of the first HFNC session and the number of total HFNC sessions were recorded. Collected respiratory variables included SpO2, frequency, and FIO2, allowing calculation of the ROX index (SpO2/FIO2 to breathing frequency), as well as PaO2/FIO2. These variables were calculated at admission upon HFNC start (baseline), then every 6 h on the first day. Since the 12th hour ROX measurement was available in the majority of subjects whereas only a small proportion of subjects had to interrupt the first prone session before the sixth hour, we calculated the difference between ROX at 12 h and at baseline (ΔROX). The independent association of each of these oxygenation variables and calculated indexes (ROX, ΔROX, PaO2/FIO2) with HFNC failure were evaluated by measurement of area under receiver operating charac-teristic (ROC) curve and logistic regression using IBM SPSS Statistics version 21 (IBM, Armonk, New York).
Results
During the study period, 213/360 patients with COVID-19–related ARF were placed on HFNC and included in the study. Excluded subjects were either invasively ventilated (98) or required other forms of noninvasive respiratory support (30) such as CPAP or BPAP; 6 subjects did not have confirma-tion of COVID-19, 6 had COVID-19 without ARF, 2 had do-not-intubate orders, and 5 were readmitted to the ICU. Overall, 178/213 subjects (83.5%) on HFNC tolerated prone positioning for a median of 12 (6–16) h on the day of admission and 5 (2–7) d total during the hospitalization. The major limitations to prone positioning were back or shoulder pain (47.1%), obesity (23.5%), delirium (17.6%), or general discomfort (11.8%).
Table 1 depicts the main characteristics of subjects included in the study. At admission, their median PaO2/FIO2 was 104 (73–143) mm Hg, and SpO2 on room air was 85 (77–88)%.
Baseline Characteristics of Subjects Receiving High-Flow Nasal Cannula
Body Position, ROX Index, and HFNC Outcome
Sixty-one subjects (28.1%) required intubation. Proportions of HFNC failure were similar between prone subjects and those who received therapy in the supine position (29% and 26%, respectively; risk ratio 1.14 [95% CI 0.62–2.10]). In comparison to successfully treated subjects, those who failed HFNC had significantly higher severity scores (Simplified Acute Physiology Score II and Sequential Organ Failure Assessment [SOFA]) and lower SpO2, PaO2/FIO2, and baseline ROX (Table 1). The ΔROX index increased significantly more in the HFNC success group compared to the group failing this therapy (medians, IQR): 2.7 (−0.7 to 3.6) and 0.47 (−4.3 to 2.9), respectively.
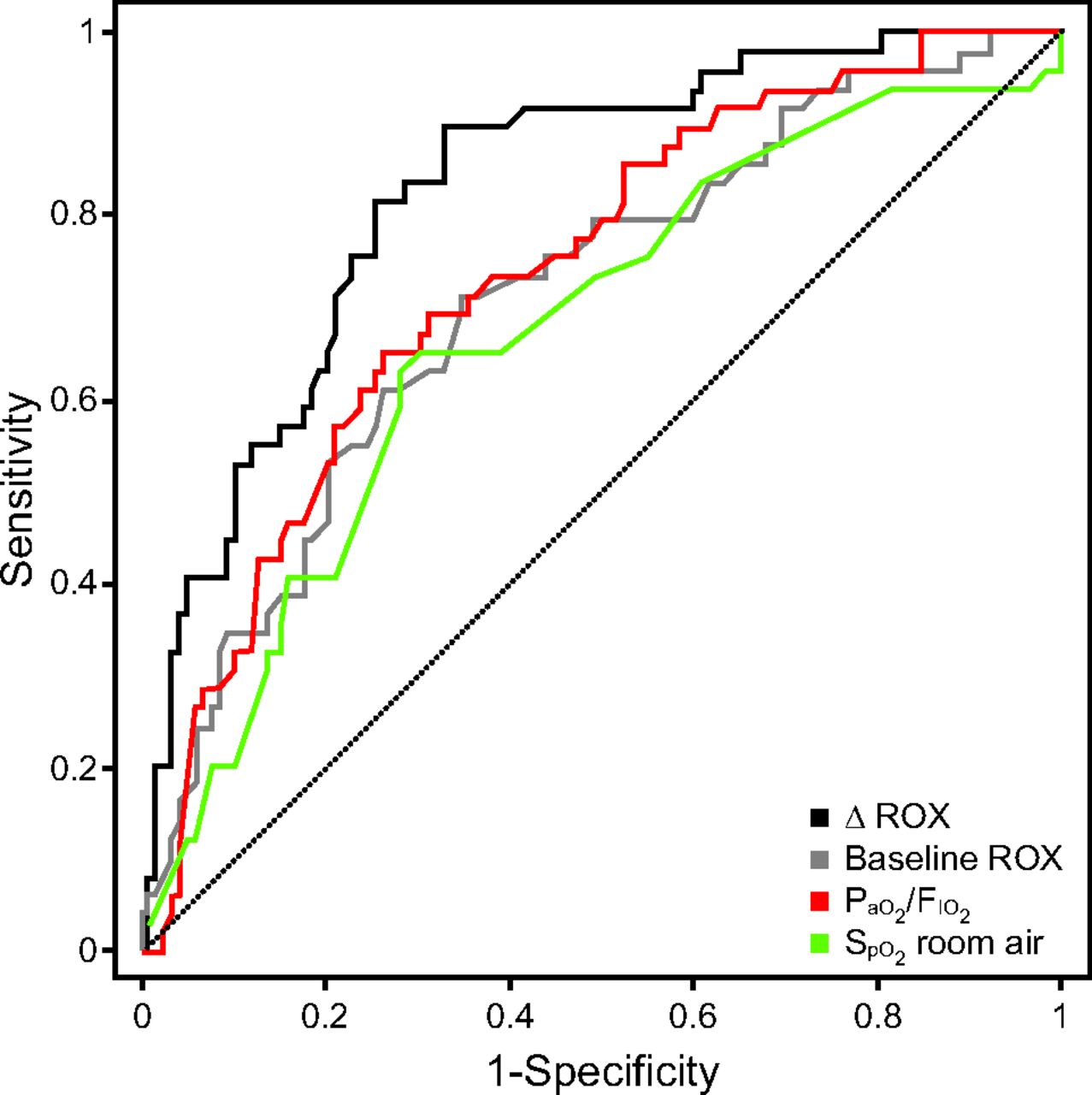
The area under the ROC curve was the highest for ΔROX (area under the curve = 0.83) (see figure). In contrast, the area under the curve for baseline level of ROX, PaO2/FIO2, and SpO2 on room air were, respectively, 0.71 (P = .04 vs ΔROX by DeLong test), 0.73 (P = .05 vs ΔROX), and 0.67 (P = .03 vs ΔROX) (see figure). A ΔROX cutoff ≤ 1.8 had the best Youden index indicating the best combination of sensitivity (0.89) and specificity (0.61) with a positive likelihood ratio of 2.33 and a negative likelihood ratio of 0.17 to predict HFNC failure.

Receiver operating characteristic curves of variables with potential for predicting high-flow nasal cannula success. Area under the curve for ΔROX (area under the curve = 0.83) was significantly higher than area under the curve of baseline ROX (area under the curve = 0.71, P = .04 vs ΔROX), baseline PaO2/FIO2 (area under the curve = 0.73, P = .05 vs ΔROX), and SpO2 on room air (area under the-curve = 0.67, P = .03 vs ΔROX). ROX = ratio of SpO2/FIO2 over Respiratory rate.
Variables with a P < .10 in univariate analysis were included in the multiple logistic regression analysis, which identified the following as being independently associated with HFNC failure: ΔROX odds ratio 0.44 ([95% CI 0.32–0.62], P < .001); baseline ROX index odds ratio 0.58 ([95% CI 0.39–0.85], P = .005); SOFA score odds ratio 0.6 for each point ([95% CI 1.1–2.2], P = .007); and PaO2/FIO2 at admission odds ratio 0.96 (95% CI 0.94–0.99). Prone positioning was not related to HFNC success. Fifty-two subjects died in the ICU (24.4%) primarily secondary to ventilator-associated pneumonia (bacterial and fungal) or refractory hypoxemia.
Discussion
Of 213 subjects receiving HFNC with COVID-19–related severe hypoxemic respiratory failure and instructed to lie in the prone position, 35 subjects did not tolerate prone position, whereas the remaining 178 (83.5%) received HFNC and awake prone position. There was no difference in intubation rates between groups. By the 12th hour following admission, the ROX index increased significantly more in subjects treated successfully with HFNC than in those failing therapy. ΔROX had the best operative characteristics. A ΔROX cutoff ≤ 1.8 had the best combination of characteristics in predicting the failure of HFNC. HFNC outcome was independently associated with indicators of ARF severity (such as SOFA score, baseline PaO2/FIO2, or baseline ROX) and with ΔROX. As a simple and accessible measure of initial physiological response to HFNC, ΔROX could contribute to the identification of subjects at risk of HFNC failure in order to help in making the appropriate clinical decision to continue or stop HFNC in a timely manner.
Environmental exposure and spread of COVID-19 to health care workers can occur with aerosol-generating procedures such as intubation. Whereas some forms of noninvasive respiratory support may disperse bioaerosols, many guidelines have recommended their use secondary to the high morbidity and mortality rates associated with invasive ventilation.11,12 Combining prone position with noninvasive respiratory support in awake patients has progressively gained scientific ground.5,13,14 Its use in patients with COVID-19–related ARF has been reported to improve oxygenation in several retrospective studies and small prospective cohorts.5,13,15 The evidence for the superiority of awake prone positioning over supine in COVID-19–related hypoxemic respiratory failure stems from the meta-trial by Ehrmann et al.6
In addition to information on feasibility and outcome of awake prone in everyday practice, our data provide information on factors that are independently associated with HFNC outcome in the specific setting of COVID-19–related hypoxemia. Our study confirms the performance of the ROX index evaluated outside the COVID-19 setting. Moreover, we emphasize the higher yield of the magnitude of ROX change by the 12th hour following HFNC initiation in comparison to the ROX index calculated at baseline. An increase by the threshold of 1.8 appears to have the best operative characteristics to predict HFNC failure. Our study did not deal with a critical unanswered question concerning the yield of an earlier physiological response such as time points allowing calculation of ΔROX between 0–6 h or that between 6–12 h. Future studies should explore the performance of ΔROX calculated earlier (0–6 h or 6–12 h). HFNC with awake prone positioning was feasible in most subjects with severe hypoxemic COVID-19. Among oxygenation indicators, the change in ROX indicated the response to treatment related to independent association with HFNC outcomes, compared to static indicators and needs to be validated prospectively.
Footnotes
- Correspondence: Fekri Abroug MD, ICU, CHU F.Bourguiba, 5000, Monastir, Tunisia. E-mail: fekri.abroug{at}gmail.com
The authors have disclosed no conflicts of interest.
- Copyright © 2023 by Daedalus Enterprises





{kind=link}