

Abstract
BACKGROUND: Volumetric capnography dead-space measurements (physiologic dead-space-to-tidal-volume ratio [VD/VT] and alveolar VD/VT) are considered more accurate than the more readily available time-based capnography dead-space measurement (end-tidal alveolar dead-space fraction [AVDSF]). We sought to investigate the correlation between volumetric capnography and time-based capnography dead-space measurements.
METHODS: This was a single-center prospective cohort study of 65 mechanically ventilated children with arterial lines. Physiologic VD/VT, alveolar VD/VT, and AVDSF were calculated with each arterial blood gas using capnography data.
RESULTS: We analyzed 534 arterial blood gases from 65 children (median age 4.9 y, interquartile range 1.7–12.8). The correlation between physiologic VD/VT and AVDSF (r = 0.66, 95% CI 0.59–0.72) was weaker than the correlation between alveolar VD/VT and AVDSF (r = 0.8, 95% CI 0.76–0.85). The correlation between physiologic VD/VT and AVDSF was weaker in children with low PaO2/FIO2 (< 200 mm Hg), low exhaled VT (< 100 mL), a pulmonary reason for mechanical ventilation, or large airway VD (> 3 mL/kg). All 3 dead-space measurements were highly correlated (r > 0.7) in children without hypoxemia (PaO2/FIO2 > 300 mm Hg), mechanically ventilated for a neurologic or cardiac reason, or on significant inotropes or vasopressors.
CONCLUSIONS: In mechanically ventilated children without significant hypoxemia or with cardiac output-related dead-space changes, physiologic VD/VT was highly correlated with AVDSF and alveolar VD/VT. In children with significant hypoxemia, physiologic VD/VT was poorly correlated with AVDSF. Alveolar VD/VT and AVDSF correlated well in most tested circumstances. Therefore, AVDSF may be useful in most children for alveolar dead-space monitoring.
- respiratory dead space
- pediatrics
- mechanical ventilation
- respiratory failure
- acute lung injury
- capnography
Introduction
Monitoring dead space in critically ill children is useful for both prognostic and therapeutic reasons. Large dead space in mechanically ventilated children and adults is an indicator of respiratory disease severity and is associated with increased mortality, longer duration of mechanical ventilation, and higher extubation failure rates.1–8 Optimizing mechanical ventilation settings by minimizing dead space has the potential to improve outcomes in children with respiratory failure.9,10
Physiologic dead space is composed of both airway dead space and alveolar dead space. In healthy children, the physiologic dead-space-to-tidal-volume ratio (VD/VT) ranges from 0.3 to 0.35.11 Airway dead space represents regions of the respiratory system that receive VT but do not normally participate in gas exchange (eg, large conducting airways and the endotracheal tube [ETT] for intubated children). Alveolar dead space (alveoli receiving ventilation without perfusion) is close to zero in healthy children.12 However, in critical illness, decreased alveolar perfusion can lead to large alveolar dead space due to alveolar overdistention, decreased cardiac output, or a multitude of other causes. Hence, measuring alveolar dead space provides information on the severity of lung disease and adequacy of pulmonary perfusion, both globally and regionally.
Volumetric capnography measures the volume of CO2 exhaled with each breath. The mean expiratory PCO2 and breath-by-breath curve analysis obtained from volumetric capnography, in conjunction with PaCO2 level, provide the data needed to estimate physiologic, airway, and alveolar VD. Although it has limitations, volumetric capnography is generally considered an accurate method to evaluate dead space. However volumetric capnography requires specialized equipment not used for most mechanically ventilated children.
On the other hand time-based capnography is routinely used for mechanically ventilated children, reporting the end-tidal PCO2 (PETCO2) with each breath. Using the PETCO2, the end-tidal alveolar dead-space fraction (AVDSF) can be calculated (AVDSF = [PaCO2 − PETCO2]/PaCO2). Some clinicians use AVDSF at the bedside to monitor changes in dead space.13 PETCO2 is more representative of alveolar gas than proximal airway gas.14 Consequently, AVDSF is viewed as a measurement of alveolar VD.
The correlation of volumetric capnography dead-space measurements (physiologic and alveolar VD/VT) with the time-based capnography dead-space measurement (AVDSF) has not been previously described in mechanically ventilated adults or children. Our primary objective was to determine the correlation strength between physiologic VD/VT and AVDSF. Secondary objectives were to investigate the correlation strength between alveolar VD/VT and AVDSF and between physiologic and alveolar VD/VT and to identify factors that may explain the relationships between dead-space measurements.
QUICK LOOK
Current knowledge
Monitoring physiologic dead space in mechanically ventilated children has proven to be useful for both prognostic and therapeutic information. Large dead space in mechanically ventilated children and adults is an indicator of respiratory disease severity and is associated with increased mortality, longer duration of mechanical ventilation, and higher extubation failure rates. Optimizing mechanical ventilation settings by minimizing dead space has been proposed, but has not become routine.
What this paper contributes to our knowledge
In a group of 65 mechanically ventilated children without significant hypoxemia or cardiac output-related dead-space changes, the dead-space-to-tidal-volume ratio (VD/VT) was highly correlated with the end-tidal alveolar dead-space fraction (AVDSF). The correlation between VD/VT and AVDSF was weaker in children with low PaO2/FIO2 (< 200 mg Hg), VT < 100 mL, a pulmonary reason for mechanical ventilation, or large airway dead space (> 3 mL/kg). All 3 dead-space measurements were highly correlated (r > 0.7) in children without hypoxemia (PaO2/FIO2 > 300 mm Hg), ventilated for a neurologic or cardiac reason, or on significant inotropes or vasopressors. The utility of these measurements to guide clinical decision making remains unclear.
Methods
This was a prospective cohort study of mechanically ventilated children < 21 y of age with arterial lines who were admitted to the pediatric ICU at Children's Hospital Los Angeles between November 2011 and October 2013. Children with an ETT leak of > 20% ([inhaled − exhaled VT]/inhaled VT) × 100), obstructive airway disease (determined by clinical examination or flow-volume loops), on high-frequency oscillatory ventilation, or on CPAP were excluded.15 Children on CPAP were excluded due to their generally lower VT, shorter inspiratory times, and higher breathing frequencies. All children were ventilated with pressure control, pressure-regulated volume control, or pressure support ventilation. The majority of children received continuous sedation during the study period; however, this was not an inclusion criterion. The Children's Hospital Los Angeles institutional review board approved this study with a waiver of informed consent (CCI 11-00243).
An NM3 device (Philips Respironics, Murrysville, Pennsylvania) was used to monitor volumetric capnography according to the recommendations of the manufacturer. NM3 monitoring adds <1 mL of airway VD for neonatal sensors (ETT size of 2.5–4 mm), <4 mL of airway VD for pediatric sensors (ETT size of 3.5–6 mm), and <8.5 mL of airway VD for adult sensors (ETT size of > 5.5 mm).
At the time of each arterial blood gas test (drawn at the discretion of the treating physicians), volumetric capnography physiologic and alveolar VD/VT and time-based capnography AVDSF were calculated. The NM3 monitor reports PETCO2, which was used to calculate AVDSF. Respiratory therapists performed arterial blood gas tests during periods of stability (ie, arterial blood gas tests were not performed within 15 min of ETT suctioning or ventilator changes).
Physiologic VD/VT was calculated using the Bohr-Enghoff equation: physiologic VD/VT = (PaCO2 − mean expiratory PCO2)/PaCO2. Airway VD was estimated by breath-to-breath analysis of the volumetric capnography curve by the NM3 monitor (Fowler's method) (Fig. 1).16,17 Alveolar VD can then be estimated using the calculated physiologic VD/VT and airway VD and the measured exhaled VT (mL). Alveolar VD = exhaled VT(physiologic VD/VT) − airway VD. Alveolar VD/VT is calculated by dividing alveolar VD by alveolar VT (obtained from NM3 analysis of the volumetric capnography curve). For each variable, 1 min of data obtained at the time of the arterial blood gas test was averaged and used for all calculations (an average of 25 breaths/min were analyzed for data calculations). Physiologically impossible values for any measurement were excluded from the analysis (eg, values of AVDSF < 0). This represented < 10% of the obtained values.

The intersection of the slope line of phase II and the slope line of phase III is where phase III begins. A perpendicular line divides p and q until they are equal, attributing half of the volume to airway dead space (VD) and half of the volume to alveolar VD. The dark grey area represents airway VD. The light grey area represents alveolar VD. PETCO2 = end-tidal PCO2.
Physiologically plausible confounders of the correlation between dead-space measurements were evaluated, including physiologic VD/VT, exhaled VT/kg, exhaled VT, modified inotrope score, PaO2/FIO2, breathing frequency, reason for mechanical ventilation, PEEP, and airway VD. A modified inotrope score of the most commonly used vasoactive medications in our pediatric ICU was used: dopamine (μg/kg/min) + epinephrine (mg/kg/min) × 100 + milrinone (μg/kg/min) × 10.18 The reason for mechanical ventilation was classified as primarily for cardiac, neurologic, or pulmonary reasons. Hypoxemia severity was measured using PaO2/FIO2.
Statistical Analysis
Analysis was performed using R 2.13 (R Foundation for Statistical Computing, Vienna, Austria) and SAS 9.3 (SAS Institute, Cary, North Carolina). The correlation between (1) physiologic VD/VT and AVDSF, (2) alveolar VD/VT and AVDSF, and (3) physiologic and alveolar VD/VT was calculated using the Pearson correlation coefficient with repeated measurements for correlations within subjects.19 Correlation coefficients were also calculated within variable subgroups: physiologic VD/VT, exhaled VT/kg, exhaled VT, modified inotrope score, PaO2/FIO2, breathing frequency, reason for mechanical ventilation, PEEP, and airway VD. There is no statistical test to compare Pearson correlation coefficients with repeated measurements precluding a single P value. For this reason, confidence intervals for each correlation coefficient were calculated using a bootstrap methodology. This simulates the variability of the correlation coefficients by resampling with replacement 1,000 times from the repeated measures of the 2 variables being analyzed and computing the corresponding correlation coefficient each time.20 The 95% CIs were deduced from the histogram of simulated correlation coefficients.
Multivariate mixed linear regression modeling was used to control for patient-level effects while examining potential confounders. The absolute difference between the 2 variables was normally transformed using the log function and used as the dependent variable in the linear regression models. Univariate models were built for (1) log(absolute [physiologic VD/VT − AVDSF]) and (2) log(absolute [alveolar VD/VT − AVDSF]) controlling for patient-level effects first and then examining the effect of each potentially influential variable. Variables with P < .2 were considered for inclusion in our multivariate model. Multivariate models controlling for patient-level effects were built, and variables with P < .05 remained in the final multivariate model.
Results
We enrolled 65 mechanically ventilated children (52% male) with a median age of 4.9 y (interquartile range 1.7–12.8) and median weight of 16.8 kg (interquartile range 11.2–31.9). The primary reason for mechanical ventilation was pulmonary disease in 26 children (40%), cardiac disease in 26 children (40%), and neurologic disease in 13 children (20%). A mean ± SD of 8.2 ±5.2 arterial blood gases (range 2–23) per child were evaluated. In total, 534 arterial blood gases were used for the analysis (Table 1). The mean ±SD difference between the maximum and minimum physiologic VD/VT per child was 0.14 ±0.09 (median difference 0.14, minimum difference 0.02, maximum difference 0.45, interquartile range 0.07–0.19).
Pulmonary Characteristics at the Time of Arterial Blood Gas Testing
Correlation Between Physiologic VD/VT and AVDSF
The correlation between physiologic VD/VT and AVDSF for all arterial blood gases was good (r = 0.66, 95% CI 0.59–0.72) (Fig. 2 and Table 2). The correlation between physiologic VD/VT and AVDSF was higher in children with moderately elevated physiologic VD/VT (0.4 > VD/VT ≤ 0.6), higher VT/kg (exhaled VT/kg > 8 mL/kg), on inotropes or vasopressors, breathing frequencies in the middle range (20 > f < 30 breaths/min), and low PEEP (≤ 6 cm H2O). On the other hand, in children with significant hypoxemia (PaO2/FIO2 < 200), low VT (exhaled VT < 100 mL), mechanically ventilated for pulmonary disease, or large airway VD (> 3 mL/kg), the correlation was lower. Multivariate linear regression analysis demonstrated that the difference between physiologic VD/VT and AVDSF increased in children with lower VT/kg (P > .001), lower modified inotrope score (P = .003), higher breathing frequency (P = .009), and larger airway VD (P < .001) (Table 3).
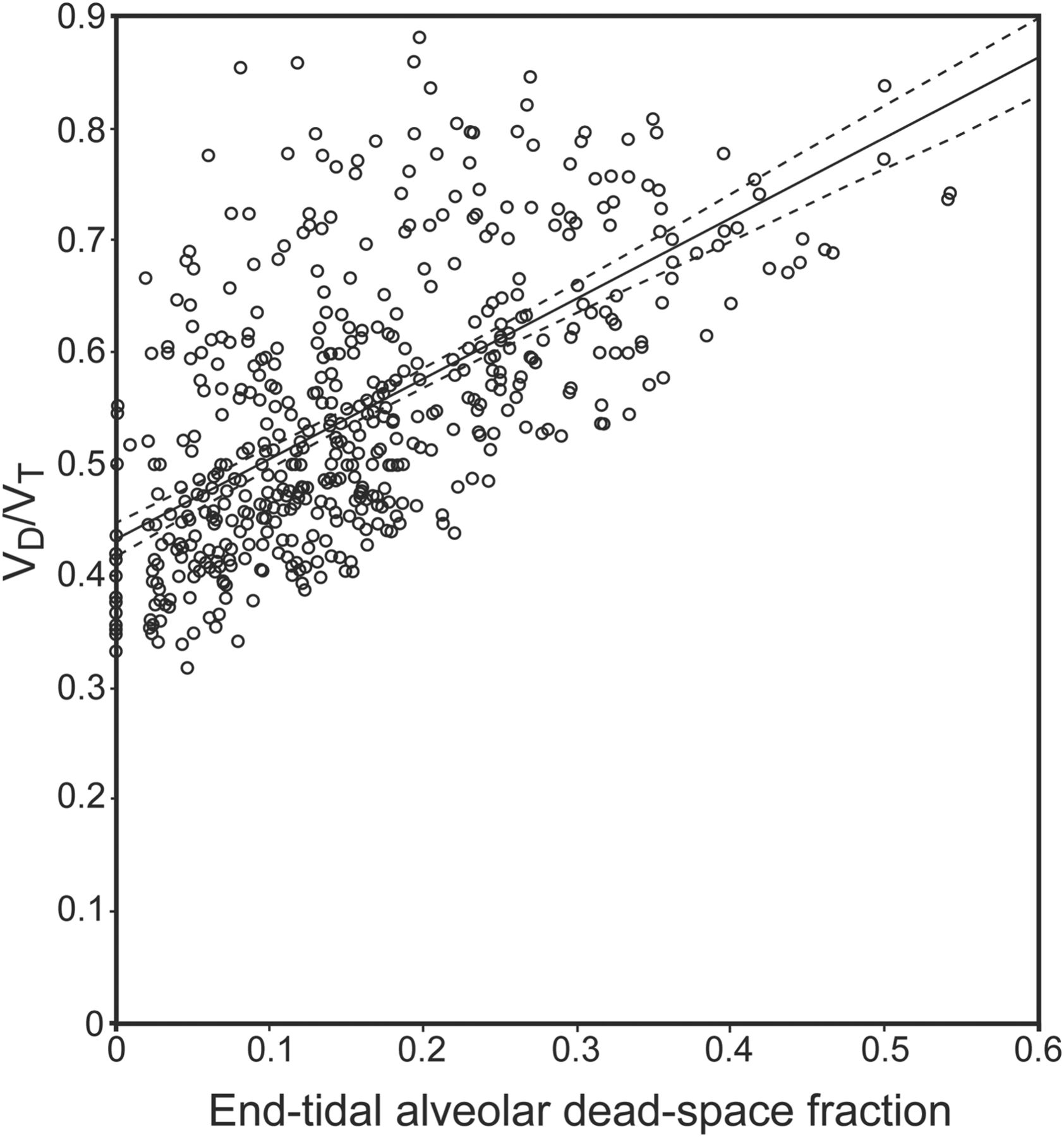
Scatterplot of physiologic dead-space-to-tidal-volume ratio (VD/VT) and end-tidal alveolar dead-space fraction with 95% CI (dashed lines). Within-subjects Pearson correlation coefficient = 0.66 (95% CI 0.59–0.72).
Correlation Coefficients for All Arterial Blood Gases and Subgroup Analyses
Multivariate Regression Models
Correlation Between Alveolar VD/VT and AVDSF
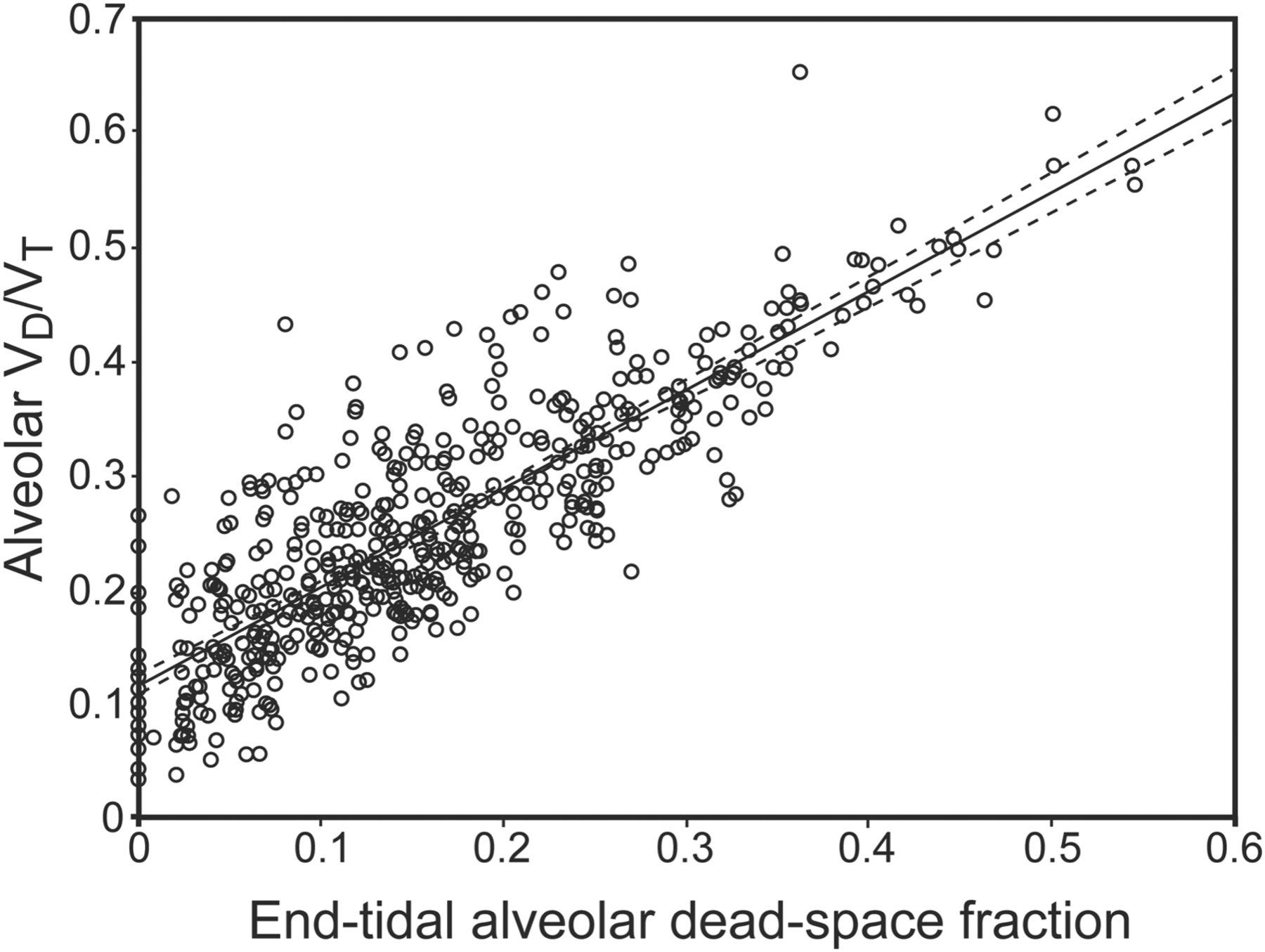
The correlation between alveolar VD/VT and AVDSF was strong (r = 0.80, 95% CI 0.76–0.85) (Fig. 3 and see Table 2). The correlation remained strong consistently in all subgroups with the only r value < 0.65 in children with a normal-to-low VD/VT (≤ 0.4, r = 0.38) or small airway VD (≤ 2 mL/kg, r = 0.59). In multivariate analysis, lower breathing frequency (P = .008), smaller airway VD (P = .004), and higher VT/kg (P = .03) were significantly associated with a larger difference between alveolar VD/VT and AVDSF (see Table 3). The correlation between alveolar VD/VT and AVDSF was statistically significantly higher than the correlation between physiologic VD/VT and AVDSF when analyzing all arterial blood gases and in many subgroup analyses. In children with a high physiologic VD/VT (> 0.6), significant hypoxemia (PaO2/FIO2 < 200), a large amount of airway VD (≥ 3 mL/kg), or on no inotropes or vasopressors (modified inotrope score of 0), the correlation between alveolar VD/VT and AVDSF was r ≥ 0.2 higher than the correlation between physiologic VD/VT and AVDSF.

Scatterplot of volumetric capnography alveolar dead-space-to-tidal-volume ratio (VD/VT) and end-tidal alveolar dead-space fraction with 95% CI (dashed lines). Within-subjects Pearson correlation coefficient = 0.8 (95% CI 0.76–0.85).
The correlation between physiologic and alveolar VD/VT (r = 0.66, 95% CI 0.57–0.74) was similar to the correlation between physiologic VD/VT and AVDSF. The correlations between physiologic VD/VT, alveolar VD/VT, and AVDSF were all r > 0.7 in children with a high VT/kg (> 8 mL/kg), minimum hypoxemia (PaO2/FIO2 > 300), low PEEP (< 6 cm H2O), mechanically ventilated for neurologic or cardiac disease, or on significant inotropes or vasopressors (modified inotrope score of > 10).
Discussion
Our data demonstrate that AVDSF is highly correlated with both physiologic and alveolar VD/VT in mechanically ventilated children with changing alveolar VD related to cardiac output and in the absence of significant hypoxemia. However, in children with significant hypoxemia, physiologic VD/VT may not adequately indicate changing alveolar VD, as physiologic VD/VT is poorly correlated with both AVDSF and alveolar VD/VT. In most of the conditions tested in this group of children, alveolar VD/VT and AVDSF correlated well.
All measurements of VD make assumptions and have limitations. Volumetric capnography uses the Enghoff modification of the Bohr equation to estimate the physiologic dead-space fraction by substituting the PaCO2 for the alveolar PCO2, assuming they are equal. Alveolar VD calculated by volumetric capnography makes this assumption and assumes that the dead-space volume attributable to alveolar VD during phase II of the volumetric capnography curve is equal to airway VD (see Fig. 1). Because PETCO2 is the maximum CO2 pressure, typically measured at the end of exhalation, AVDSF would be expected to be most representative of alveoli with long emptying times. In contrast, alveolar and physiologic VD/VT may better account for alveolar emptying heterogeneity represented by the slope of phase III. Furthermore, volumetric and time-based capnography dead-space measurements are affected by a large amount of pulmonary or cardiac shunting, increasing the PaCO2 more than the alveolar PCO2 and creating shunt-related dead space.21
Given that physiologic VD/VT, alveolar VD/VT, and AVDSF are each unique dead-space measurements, with none precisely measuring the alveolar or physiologic dead-space fraction, we analyzed how they trended together rather than their ability to estimate each other. Although the correlation between alveolar VD/VT and AVDSF could be affected by changes in phase III slope, this is unlikely in the subjects in this group, who, for the most part, were not ventilated on high PEEP and had minimum obstructive airway disease.22 Although we did not collect data on phase III slopes, we did not find evidence of a weaker correlation between alveolar VD/VT and AVDSF in children with significant hypoxemia (low PaO2/FIO2). Rather, technical limitations in capnography curve interpretation (smaller airway VD, lower VD/VT) appeared to have more impact on the correlation between alveolar VD/VT and AVDSF. This is logical, as the correlation would be more affected by small variations in capnography curve analysis in these situations. As AVDSF does not represent airway VD, it should be less correlated with physiologic VD/VT when changes in airway VD are more prominent than changes in alveolar VD. This is supported by our multivariate analysis, in which increasing airway VD was associated with a larger difference between physiologic VD/VT and AVDSF. A higher breathing frequency, common in small children, can make it more difficult to interpret both volumetric and time-based capnography curves.23,24 This issue was confirmed by our multivariate analysis, demonstrating an association between increasing breathing frequency and a larger difference between physiologic VD/VT and AVDSF.
The weaker correlation between physiologic VD/VT and AVDSF may be related to inaccuracies in physiologic VD/VT or AVDSF calculation or changes in airway VD that affect physiologic VD/VT and not AVDSF. Although not often considered at the bedside, airway VD can change in mechanically ventilated children.25,26 For example, increasing PEEP in a child with non-recruitable lungs may lead to overdistention of conducting airways. The consistently stronger correlation between alveolar VD/VT and AVDSF versus physiologic VD/VT and AVDSF suggests that the weaker correlation may frequently be related to changing airway VD.
Although there are limitations in the accuracy of all these measurements of dead space, both volumetric capnography and time-based capnography dead-space measurements have been consistently associated with worse outcomes in mechanically ventilated children and adults.2–5,27 Larger dead space is associated with mortality in children with acute hypoxemic respiratory failure and longer duration of mechanical ventilation in neonates with congenital heart disease.7,28 Increased alveolar VD can be due to decreased pulmonary perfusion (microvascular thrombosis, low cardiac output, pulmonary hypertension) or alveolar overdistention. Although it cannot be determined without further study, physiology would suggest that the association between mortality and elevated dead space is due primarily to alveolar VD, not airway VD.29 Therefore, future studies should focus on deciphering the source of mortality risk (alveolar or airway VD) and should not report only physiologic dead-space fraction (VD/VT).
There is evidence to suggest that dead-space measurement trends, perhaps with the easily monitored AVDSF, should also be investigated further to determine whether they are more useful for prognostication than individual values.4 Monitoring trends in dead-space measurements can provide continuous bedside information describing improving or deteriorating lung disease and detecting changing pulmonary perfusion. For this reason, capnography is now recommended in cardiopulmonary resuscitation to detect the return of spontaneous circulation by identifying resuming pulmonary perfusion.30
Our study has some important limitations. Respiratory therapists actively involved in caring for children rather than research staff recorded the data. This likely resulted in collection of some of the physiologically impossible data. We did not collect breath-to-breath capnogram waveforms with each arterial blood gas test. Evaluation of these may have been helpful to understand how waveform abnormalities affected the correlations. In addition, we did not measure cardiac output, which would have provided data on how pulmonary perfusion directly affected the correlation between AVDSF and physiologic VD/VT. We recognize that PaO2/FIO2 does not fully characterize severity of lung disease; therefore, additional analysis using subgroups based on dynamic compliance was performed, with results consistent with our reported findings (analysis not shown). ETT leaks could affect the correlation between dead-space measurements, and when we performed an analysis limiting data to an ETT leak of < 10%, there was a trend toward improved correlation that did not reach statistical significance. To have a larger sample size for subgroup analysis, we chose to allow an ETT leak of up to 20%.
An advantage of volumetric capnography over time-based capnography is the ability to distinguish between airway and alveolar VD. This allows a better understanding of how physiologic VD/VT, alveolar VD/VT, and airway VD change in response to changing PEEP or VT and could be used to optimize ventilator settings based on minimizing dead space. The use of dead-space measurements for therapeutic purposes, in addition to prognostication, may be a promising next step in pediatric mechanical ventilation. A more detailed understanding of airway, alveolar, and physiologic VD will help make these therapeutic options a reality.
Conclusions
For most mechanically ventilated children, AVDSF is analogous to alveolar VD/VT in estimating changes in alveolar VD and is more easily and simply followed at the bedside. As hypoxemia worsens, the correlation between physiologic VD/VT and AVDSF decreases, perhaps related to changing airway VD or limitations in capnography curve analysis. Because alveolar VD likely drives the strong relationship between mortality and large dead space, it may be simpler to monitor AVDSF than physiologic VD/VT for prognostic purposes. However, volumetric capnography may be important when using dead-space measurements to guide ventilator support.
Footnotes
- Correspondence: Anoopindar K Bhalla MD, Children's Hospital Los Angeles, 4650 Sunset Boulevard, MS 12, Los Angeles, CA 90027. E-mail: abhalla{at}chla.usc.edu.
Dr Bhalla presented a version of this paper at the Society of Critical Care Medicine's 42nd Critical Care Congress, held January 19-23, 2013, in San Juan, Puerto Rico.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1711
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}