

Abstract
Pulmonary vascular dysfunction is associated with ARDS and leads to increased right-ventricular afterload and eventually right-ventricular failure, also called acute cor pulmonale. Interest in acute cor pulmonale and its negative impact on outcome in patients with ARDS has grown in recent years. Right-ventricular function in these patients should be closely monitored, and this is helped by the widespread use of echocardiography in intensive care units. Because mechanical ventilation may worsen right-ventricular failure, the interaction between the lungs and the right ventricle appears to be a key factor in the ventilation strategy. In this review, a rationale for a right ventricle-protective ventilation approach is provided, and such a strategy is described, including the reduction of lung stress (ie, the limitation of plateau pressure and driving pressure), the reduction of PaCO2, and the improvement of oxygenation. Prone positioning seems to be a crucial part of this strategy by protecting both the lungs and the right ventricle, resulting in increased survival of patients with ARDS. Further studies are required to validate the positive impact on prognosis of right ventricle-protective mechanical ventilation.
Introduction
Fifty years after its first description by Ashbaugh et al,1 management of ARDS is still a challenge for intensivists. Outcome remains poor, with high mortality and morbidity, despite recent therapeutic advances, such as the development of protective mechanical ventilation,2,3 the use of neuromuscular blockers,4 and prone positioning.5 Although respiratory failure is at the forefront in patients with ARDS, it is commonly associated with hemodynamic instability6 which can be related either to septic shock or to other causes, such as acute cor pulmonale, so hemodynamic management is crucial.7 Acute cor pulmonale reflects right-ventricular failure, initially described as a consequence of pulmonary embolism.8 In patients with ARDS, right-ventricular failure may occur because of pulmonary vascular dysfunction, as demonstrated in 1977 by Zapol and Snider,9 who first reported pulmonary hypertension with increased pulmonary vascular resistance (PVR) in this context. Since the 1980s,10 several authors have studied right-ventricular failure during ARDS and its consequences. Mechanical ventilation, which is central to ARDS management, also interferes with cardiac function,11 by decreasing right-ventricular preload and increasing right-ventricular afterload, and thus may worsen right-ventricular function. This is why a strategy focused only on blood gas optimization, as previously proposed,12 is questionable.
The purpose of this article is to rationalize why right-ventricular function should be integrated into the ventilation strategy for patients with ARDS. We will first describe the pathophysiology of right-ventricular failure during ARDS, focusing on the role of mechanical ventilation. We will then review the diagnosis and incidence of acute cor pulmonale and its impact on prognosis. Finally, we will summarize the right ventricle-protective ventilation approach.
Pathophysiology of Right-Ventricular Failure in ARDS
Along with alveolar damage, ARDS directly causes injury to the pulmonary circulation, through several pathophysiological mechanisms13,14: hypoxic pulmonary vasoconstriction, release of vasoconstrictive mediators, extrinsic vascular compression by interstitial edema, and blood vessel remodeling. Thromboembolic events also participate.15 All of these factors contribute to PVR elevation, pulmonary hypertension, right-ventricular afterload elevation, and eventually right-ventricular failure.
In addition to these ARDS-related factors, inadequate mechanical ventilation may have a deleterious effect not only on the lungs (ie, ventilator-induced lung injury),16 but also on right-ventricular function. Positive-pressure ventilation induces lung stress by raising transpulmonary pressure, calculated as the alveolar pressure minus the pleural pressure. Competition between the distending alveolar pressure (local lung stress) and the pulmonary capillaries17 is responsible for an increase in PVR18 and a cyclic alteration of right-ventricular outflow.19 Lung stress induced by mechanical ventilation depends on the ventilator settings, including PEEP and tidal volume, and on the compliance of the lung. Tidal volume reduction, as currently recommended, helps to limit lung stress. Although some authors suggest measuring esophageal pressure as a reflection of pleural pressure,20 thus allowing calculation of transpulmonary pressure, this measurement has several limitations, and lung stress is routinely estimated by the plateau pressure, which represents the alveolar end-inspiratory pressure. Jardin et al21 showed that a low-stress ventilation strategy, with a plateau pressure kept below 27 cm H2O, is associated with a lower incidence of acute cor pulmonale. It should be noted that plateau pressure is not always an adequate surrogate of lung stress,22 because it takes into account chest wall compliance,23 which can be depressed, as seen in obese patients. Driving pressure estimates tidal volume-related lung stress and is defined as plateau pressure minus total PEEP. Driving pressure has the same limitation as plateau pressure, related to chest wall compared with the transpulmonary driving pressure. Driving pressure was recently reported to be strongly associated with survival24,25 but is also a risk factor for acute cor pulmonale.26
Because of the opposite effects of lung inflation on intra- and extra-alveolar blood vessels, the relationship between lung inflation and PVR can be represented by a U-shaped curve18,27: Both atelectasis and alveolar overdistention are responsible for an elevation of PVR. That means that the lowest PVR can be obtained with the ventilator settings that achieve the best balance between alveolar recruitment and overdistention. This is a major concern, because the loss of aeration is not uniform during ARDS,28 and collapsed areas coexist with normally aerated areas. Another point is that the recruitability of the lung is very difficult to easily assess at the bedside and is highly variable among patients. The direct implication is, for instance, that a high PEEP is likely to recruit collapsed areas but also to overdistend normally aerated areas29 and thus to impair right-ventricular function.30
The last variable that contributes to pulmonary hypertension is PaCO2, since hypercapnia (and, more generally, acidosis) is responsible for pulmonary vasoconstriction.31 During ARDS, hypercapnia is the consequence of the reduction of tidal volume on the one hand and of the alveolar dead space on the other hand. The latter has been reported to be associated with poor prognosis.32 The negative impact of hypercapnia on right-ventricular function in patients with ARDS has been clearly demonstrated.33
To summarize, 4 risk factors for acute cor pulmonale in a cohort of 752 subjects with ARDS receiving protective mechanical ventilation have recently been reported: pneumonia as the cause of ARDS, a PaO2/FIO2 < 150 mm Hg, a PaCO2 ≥ 48 mm Hg, and a driving pressure ≥18 cm H2O.34
Diagnosis, Incidence, and Impact on Outcome of Acute Cor Pulmonale
Historically, acute cor pulmonale was suspected using a pulmonary arterial catheter in the case of right atrial pressure higher than pulmonary artery occlusion pressure, which is a dramatic situation. Nowadays, echocardiography is considered the accepted standard. The transesophageal approach seems to be more accurate than the transthoracic approach because of a better quality image in mechanically ventilated patients.35 The echocardiographic pattern of acute cor pulmonale is the association of right-ventricular dilatation with paradoxical motion of the interventricular septum at end-systole (“D-shape” aspect of the left ventricle) (Fig. 1).36 When the right-ventricular end-diastolic area is greater than the left ventricular end-diastolic area, acute cor pulmonale is considered to be severe.
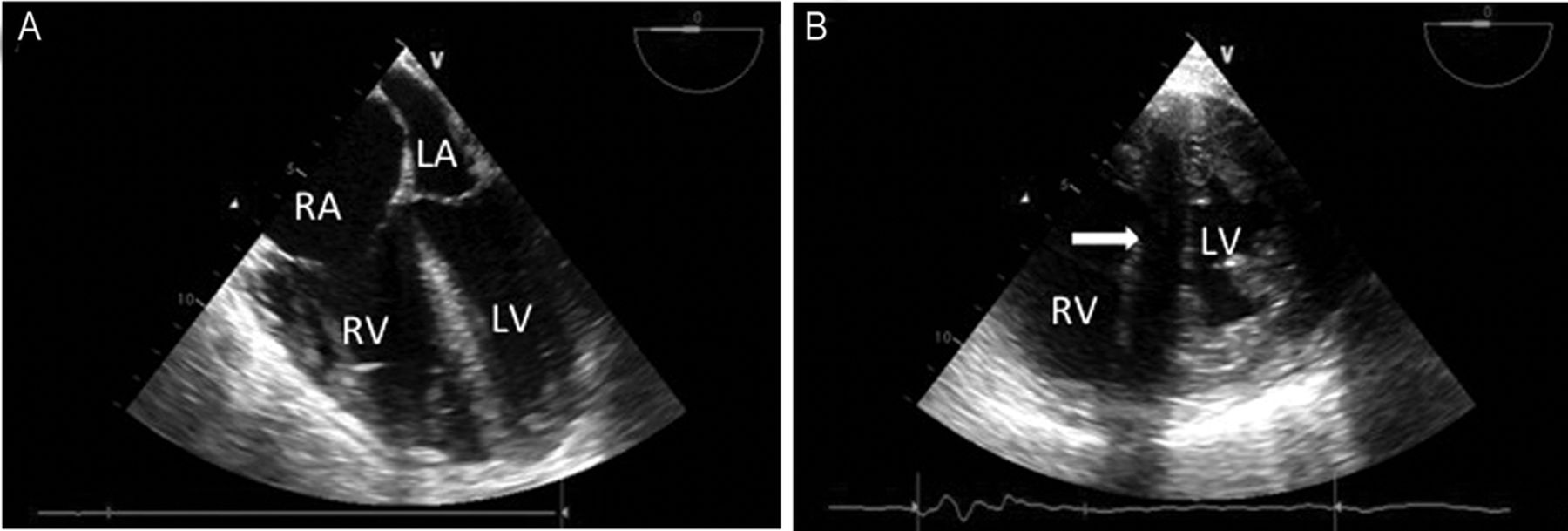
Transesophageal echocardiography demonstrating acute cor pulmonale. A: Mid-esophageal 4-chamber view showing severe right-ventricular dilatation (right ventricle bigger than left ventricle). The bulging of the interatrial septum toward the left atrium indicates right atrium pressure elevation. B: Transgastric short axis view showing paradoxical septal motion (arrow), with a D-shaped left ventricle. RA = right atrium; LA = left atrium; RV = right ventricle; LV = left ventricle.
The spread of protective mechanical ventilation has reduced the incidence of acute cor pulmonale in patients with ARDS because of airway pressure limitation. Recently, Mekontso Dessap et al34 reported the largest prospective cohort of subjects presenting with moderate and severe ARDS with transesophageal echocardiographic evaluation. In this cohort, the prevalence of acute cor pulmonale was 22%, confirming the results of several previous studies.26,35,37 In recent decades, the exact influence of acute cor pulmonale on outcome has been debated. Acute cor pulmonale may induce or worsen circulatory failure: Patients with acute cor pulmonale have a lower cardiac index38 and a higher incidence of shock26 than patients without acute cor pulmonale and require more frequent vasopressor perfusion.35 However, acute cor pulmonale has been reported as an independent factor associated with mortality by some authors26,39 but not by others,35,37 although pulmonary vascular dysfunction is also reported to be independently associated with mortality.40 The study by Mekontso Dessap et al34 brings clarification to the debate, since it shows that mortality in this cohort did not differ between subjects with and without acute cor pulmonale but was significantly higher in the subgroup of subjects presenting severe acute cor pulmonale. This is very remarkable, especially because prone positioning was used more often in subjects with acute cor pulmonale, which probably helps to reduce the difference in mortality. In the same study, acute cor pulmonale prevalence varied from <10% for subjects with no more than one of the previously described risk factors to ∼75% for subjects with all 4 factors, which allows the building of a predictive score between 0 and 4. This score should be very useful in the future for early identification of patients most at risk of developing acute cor pulmonale, to mandate echocardiographic evaluation and early adaptation of respiratory management. Indeed, all of these risk factors, except for pneumonia as a cause, are the direct or indirect consequences of ventilator settings.
Description of Right Ventricle-Protective Ventilation
The right ventricle-protective approach, as extensively described before,41 should focus on 3 components: reducing lung stress by limitation of plateau pressure and driving pressure, improving oxygenation to reverse hypoxic pulmonary vasoconstriction, and reducing hypercapnia. Sometimes, in the most severely ill patients, these goals may be contradictory, and proning may then be useful. Tidal volume and PEEP should be adjusted to maintain plateau pressure <27 cm H2O and driving pressure <18 cm H2O. The optimal PEEP remains controversial but could probably be seen as the PEEP associated with the best PaO2/FIO2 ratio without reducing the compliance of the respiratory system or even increasing this compliance, as suggested by Suter et al42 many years ago with their concept of best compliance. If so, PEEP would have the better balance between recruitment and overdistention, in favor of the former, thus not harming the right ventricle.
Clearly, hypercapnia cannot be an objective per se, as proposed.43 If so, it may induce the risk of developing acute cor pulmonale. PaCO2 should be maintained <48 mm Hg, which represents moderate hypercapnia. To limit hypercapnia, the breathing frequency should be increased very carefully, because this may induce intrinsic PEEP and dynamic hyperinflation and thus not improve CO2 clearance and impair right-ventricular function.44 This is why total PEEP must be closely monitored in patients with ARDS. The use of a heated humidifier, to decrease the instrumental dead space,45 should be preferred.
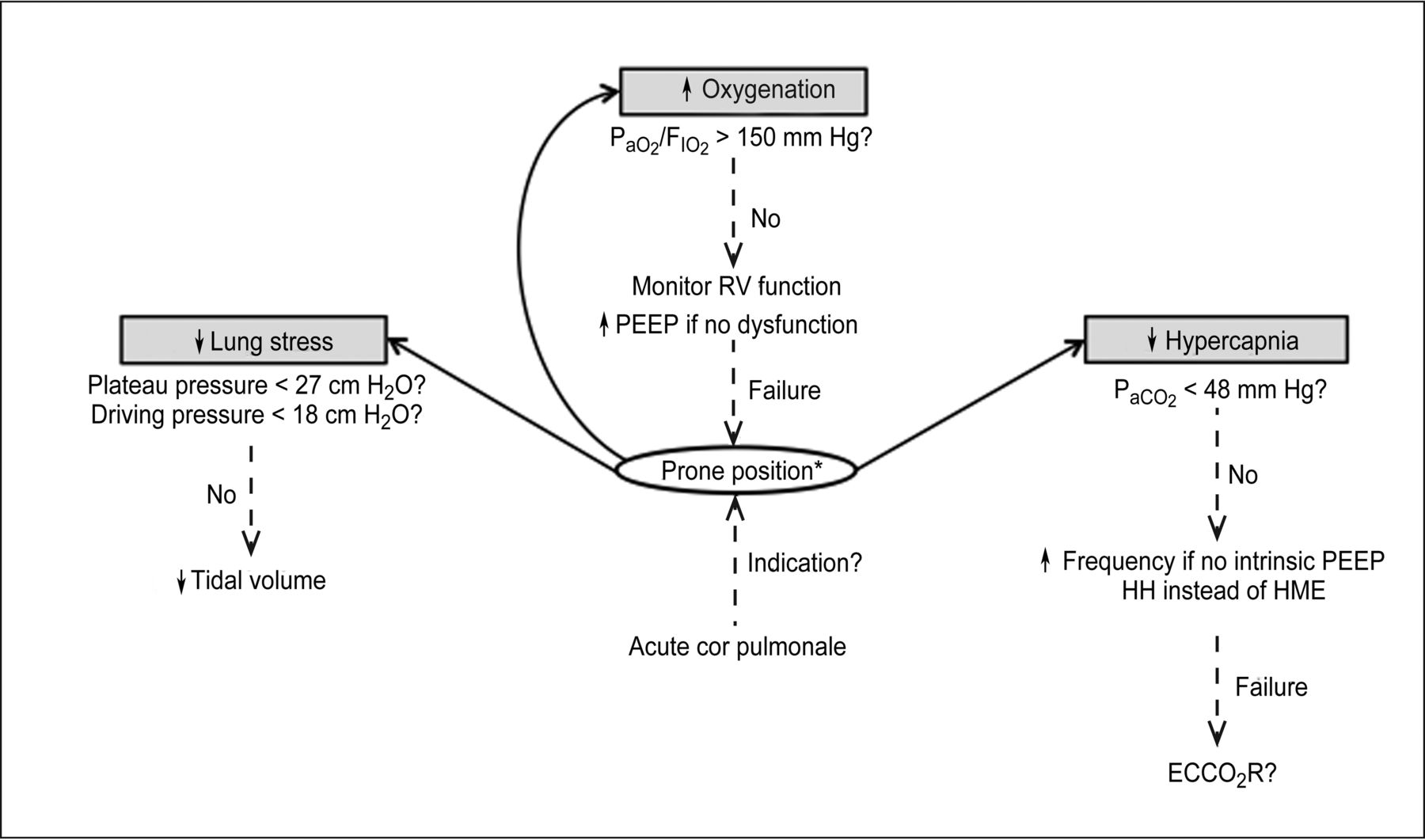
Prone positioning can be understood as the perfect approach to achieve these goals, inducing alveolar recruitment without overdistention46 and thus protecting both the lungs and the right ventricle (Fig. 2). A few years ago, the PROSEVA study5 showed a dramatic decrease in mortality after prone positioning of subjects with severe ARDS. The reasons for this decrease are not so clear. It has been reported that it is not associated with changes in gas exchange, PaO2/FIO2, or PaCO2.47 At the same time, the PROSEVA study results showed that subjects in the proning group had less cardiac arrest and more free days of cardiovascular failure 28 d following inclusion.5 Both suggest that the better outcome could mainly be the consequence of the positive hemodynamic effect of prone positioning. Two mechanisms may drive this beneficial hemodynamic effect of proning. First, prone position has been reported to decrease lung inflammation48,49 and therefore probably systemic inflammation, which may limit cardiac function impairment related to cytokine release. Second, prone position has been reported to decrease right-ventricular afterload50 and to correct right-ventricular failure when present.51 This is probably supported by its ability to improve oxygenation without increasing PEEP too much, as shown in the PROSEVA study5; to decrease PaCO2 by rendering lung ventilation more homogenous52; and to decrease driving pressure due at least to the recruitment of the dependent dorsal regions.
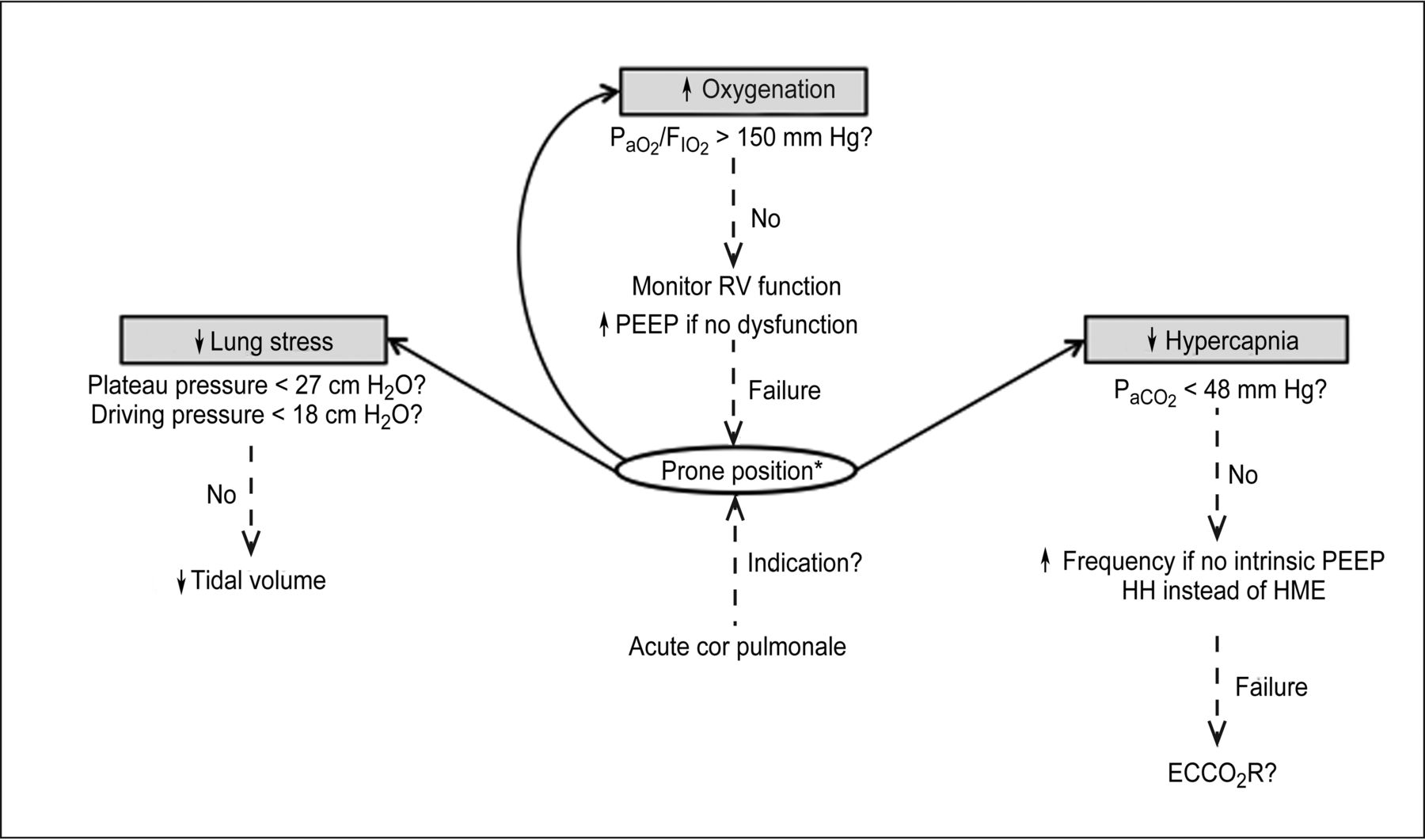
Mechanical ventilation strategy to protect the right ventricle. RV = right-ventricular; HH = heated humidifier; HME = heat and moisture exchanger; ECCO2R = extracorporeal carbon dioxide removal. * In the absence of contraindication.5
Perspectives
Quite strict control of PaCO2 is one of the major goals in the strategy we describe. However, for some patients, hypercapnia may be difficult to reduce with conventional methods. In this situation, extracorporeal CO2 removal could be an interesting approach. In an experimental model of ARDS with respiratory acidosis, Morimont et al53 showed that venovenous CO2 removal therapy normalized PaCO2, with a decrease in pulmonary artery pressure and an improvement in right-ventricular function. In humans, the same result was described in a case report,54 but this requires confirmation in a clinical study.
As mentioned before, the best compromise between alveolar recruitment and overdistention should be targeted, but it may be difficult to identify in clinical practice. Computed tomography of the lung is the accepted standard,55 but its routine use is not feasible. Lung ultrasonography is another way to assess recruitment, but it does not detect overdistention.56 For this purpose, the stress index, a variable based on the shape of the pressure-time curve, could be valuable in optimizing ventilator settings.57
Some questions remain unanswered. For example, what is the optimal timing of prone positioning and in which patients? Although a PaO2/FIO2 <150 mm Hg is now a clear indication, one can say that prone position could be useful in patients with acute cor pulmonale but a PaO2/FIO2 >150 mm Hg. In patients at high risk of developing acute cor pulmonale, as well as those with isolated right-ventricular dilatation, right-ventricular function should probably be closely monitored. This could be facilitated by the use of a single-use transesophageal echocardiography probe, which can be left in place for up to 72 h.58 Finally, we await the results of the EOLIA trial59 concerning the role of venovenous ECMO for managing the most severe patients.
Conclusions
In the light of recent research, the negative impact of right-ventricular failure in ARDS is now well established, as are its risk factors. Clinicians should not forget hemodynamics and right-ventricular function in the ventilation strategy, keeping in mind that the lung and the right ventricle are closely connected. For this purpose, echocardiography as a monitoring tool and prone positioning as a therapeutic option are key. The ability of a right ventricle-protective approach to improve the prognosis of patients with ARDS requires further validation.
Footnotes
- Correspondence: Antoine Vieillard-Baron MD PhD, Service de Réanimation Médico-Chirurgicale, Hôpital Ambroise Paré, 9 Avenue Charles de Gaulle, 92100 Boulogne, France. E-mail: antoine.vieillard-baron{at}aphp.fr.
The authors have disclosed no conflicts of interest.
- Copyright © 2016 by Daedalus Enterprises





{kind=link}
{kind=link}