

Abstract
OBJECTIVE: Information and opinions were sought on the need for graduating and practicing respiratory therapists to obtain 66 competencies necessary for practice in 2015 and beyond, the required length of respiratory care programs, the educational needs of practicing therapists, current and future workforce positions, and the appropriate credential needed by graduating therapists.
METHODS: Survey responses from respiratory therapy department directors or managers are the basis of this report. After pilot testing and refining the questions, a self-administered, Internet based, American Association for Respiratory Care (AARC) endorsed survey was used to gather information from 2,368 individuals designated as respiratory therapy department directors or managers in the AARC membership list as of May 2010.
RESULTS: A total of 663 valid survey responses (28.0%) were received. On average, the vacancy rate of surveyed hospitals was only 0.81 full-time equivalents (FTEs). Responses by directors on 66 competencies described in the second 2015 conference as needed by graduate and practicing respiratory therapists indicated 90% agreement on 37, between 50% and 90% agreement on 25, and < 50% agreement on 4 competencies. There was no consensus among directors on the academic preparation of new graduates, with 245 (36.8%) indicating a preference for a baccalaureate or master's degree, 243 (36.7%) indicating a preference for an associate degree, and 176 (26.5%) indicating no preference. There were 270 (41.8%) respondents who indicated that a baccalaureate or master's degree in respiratory therapy should be required to qualify for a license to deliver respiratory care. The survey indicated that 523 (81.2%) of directors are in favor of the RRT credential being required to practice in 2015 and beyond.
CONCLUSIONS: There was good agreement that graduate and practicing therapists should obtain the vast majority of the 66 competencies surveyed and that the entry level credential should be the RRT. Similar numbers of managers favored an entry level baccalaureate degree as favored an associate degree.
Introduction
In 2008 and 2009 the first two 2015 and Beyond conferences were conducted, sponsored by the American Association for Respiratory Care (AARC).1,2 The outcomes of these conferences clearly outlined what the conference attendees perceived were the future trends in healthcare in general and respiratory care in the specific.1 In addition, the second conference defined a series of competencies in 7 major areas (diagnostics, chronic and acute disease management, evidence-based medicine and protocols, patient assessment, leadership, emergency and critical care, therapeutics and therapeutic applications) that the participants expected the respiratory therapist (RT) in 2015 and beyond to have established competency in by the time students graduated from a Committee on Accreditation for Respiratory Care (CoARC) accredited respiratory therapy program. These same competencies defined the minimal practicing capabilities of RTs working in the field.2 The goal of the third 2015 and Beyond conference3 was to determine the educational, credentialing, and accreditation needs of the profession of respiratory care to assure that graduate and practicing RTs obtain the competencies identified in the second conference.2 In order for the participants of the third conference to have as much information as possible on which to base their recommendations, the planning committee for the 2015 and Beyond conferences developed a survey and distributed it to directors of respiratory therapy departments located in the United States, and who were identified as members of the AARC.
The intent of this survey was to quantify department directors' opinions on the need for graduating and practicing RTs to obtain the 66 competencies that were identified during the second conference as necessary for practice in 2015 and beyond.2 In addition, department directors were asked to provide their opinions on the optimal length of respiratory care education programs in 2015 and beyond, the essential educational needs of practicing therapists beyond entry into practice, the appropriate credential needed by graduating therapists in 2015 and beyond, and current and projected future workforce positions.
The committee hypothesized that department directors would not expect all graduate and practicing therapists to achieve all of the 66 competencies in the year 2015. It was believed that department directors, based on their specific work environment, would identify competencies that were most important to their individual workplace. However, the committee did believe that department directors would consider the National Board for Respiratory Care (NBRC) Registered Respiratory Therapist (RRT) credential as the required credential for entry into the profession in 2015 and beyond.
QUICK LOOK
Current knowledge
Respiratory therapists in acute care hospitals have a wide range of educational backgrounds, holding associate, baccalaureate, and master's degrees. The current entry level for clinical practice is the Certified Respiratory Therapist (CRT) credential.
What this paper contributes to our knowledge
A majority of respiratory care department managers favor the Registered Respiratory Therapist (RRT) credential as the entry level credential, beginning in 2015. A baccalaureate degree is the preferred degree for the respiratory therapist of the future. Acute care hospitals predict a 10% increase in the number of respiratory therapists over the next decade.
Methods
Questionnaire Development and Pilot Testing
This study was conducted by the 2015 Research Group (See Appendix 1 in the supplementary materials at http://www.rcjournal.com) of the AARC. Survey questions (Appendix 2 in the supplementary materials to this paper at http://www.rcjournal.com) related to respiratory therapy practice in 2015 and beyond were developed based on outcomes from 2015 conferences 1 and 2,1,2 and information believed helpful for the third conference.3 The questions were organized, reviewed, and discussed by group members, who have broad experience in RT practice, education, accreditation, certification, and licensure. The survey gathered general demographic information about the responding institutions' characteristics (eg, location, bed size, number of full-time equivalent [FTE] RTs employed). The respiratory care department directors were also asked to select which of 66 competencies identified by the second 2015 conference2 would be expected of a new graduate and other staff therapists in 2015. A section of the questionnaire asked how many FTE RTs are employed or are expected to be employed now and in the future for all positions that require graduation from an accredited respiratory therapy program. Also, the directors were asked about preferences for educational preparation of new graduates employed, the length of time needed to orient them to the hospital, and the amount of time allowed for earning the RRT credential. Several questions assessed the institution's capacity to accept additional students for clinical rotations. The current and future RT staff manpower needs of the hospital were assessed by asking about the number of unfilled positions and projected need for new positions. The survey ended by asking what academic degree and credential should be required to enter practice and to continue as an RT in 2015 and beyond (see Appendix 2 in the supplementary materials at http://www.rcjournal.com).
The survey was pilot-tested on 3 directors of respiratory care departments. These individuals were asked to comment on the following aspects of the survey:
Time. How many minutes were required for you to complete the survey?
Clarity. Are any questions ambiguous?
Invitation. Was the survey invitation letter easily understood and appropriate?
Connection. Did the link provided connect you to the online survey easily? Were you able to submit the survey easily?
Progression. Were you able to easily move forward and backwards between survey questions?
Overall. What general comments do you have regarding the survey?
The survey was revised according to the pilot-testing feedback and approved by the 2015 Research Group. The study protocol was approved by the institutional review board of Northeastern University.
Data Collection
The survey population included 2,368 directors/managers of respiratory care departments located in the United States, who were AARC members as of May 2010. The AARC President sent an invitation, via e-mail, to the managers, asking that they complete the survey. The e-mail addresses for these directors were obtained from the AARC membership database. The Internet-based survey was self-administered. To improve response rate, three e-mail follow-up reminders were sent to all non-respondents.
Data Analysis
Responses were stratified by hospital size, as determined by the number of beds. Groups of responses representing different size hospitals were compared. The number of responses by geographic region was also tabulated. Comments were categorized by content area or concern and reviewed. Percentages, frequency distribution, and differences between different size hospitals were determined with cross tabulation and Pearson chi-square analysis, using software (SPSS version 18.0, SPSS, Chicago, Illinois). A 2-tailed P < .05 was considered statistically significant.
Results
There were 663 (28.0%) valid responses received from directors or managers of 2,368 hospital respiratory care departments. The response rate by region ranged from 27.2% in the West to 29.9% in the Northeast. Directors of departments located in the South (37.7%) and Midwest (26.4%) had the most responders to the survey (Table 1). A summary of the level of agreement on competencies necessary for respiratory therapy graduates and the existing workforce can be found in Table 2. To simplify further analysis of teaching resources and projecting staffing needs, responses were evenly stratified by hospital size, as determined by the number of beds, into 3 groups (ie, 221 responses from directors of small hospitals [14–138 beds], 221 responses from medium size hospitals [139–344 beds], and 221 from large hospitals [345–1,533 beds]).
Distribution of Respondents by Region
Summary of the Level of Agreement on Competencies Necessary for Respiratory Therapy Graduates and the Existing Workforce
Greater than 90% agreement was seen by respondents on 37 competencies, between 50% and 90% agreement on 25 competencies, and < 50% agreement in only 4 competencies (Tables 2–Table 4).
Which of the Following Competencies Do You Expect a New Graduate and Other Staff Therapists to Need in 2015? Select All That Apply
Which of the Following Competencies Do You Expect a New Graduate and Other Staff Therapists to Need in 2015? Select All That Apply
In addition to the competencies needed by new graduate therapists and other staff in 2015, several other survey questions elicited information on current and future workforce issues.
This report shows that the RT departments represented by this survey currently employ FTE RTs that vary by institutional size (Table 5). The average number of FTE RTs employed over the next decade overall is projected to increase from 32.8/hospital (2010) to 36.4/hospital (2020), and varies by hospital size (see Table 5). The largest growth in average size is projected to be 20.8% (increase of 2.0 FTEs) for small hospitals, 12.8% (increase of 3.7 FTEs) for medium size hospitals, and 12.5% (increase of 8.9 FTEs) for large hospitals. The average staff therapist FTE vacancy rate per hospital overall was 0.81, and varied by hospital size (Table 6).
Full-Time Equivalent Respiratory Therapists Employed 2010 to 2020
How Many Full-Time Equivalent Unfilled Staff Respiratory Therapist Positions Do You Have? Do Not Include Supervisory Positions and Use Only Whole Numbers
Most respiratory care department directors (92.3%) in large hospitals indicated that they take students on clinical rotation, and this percentage decreased in smaller hospitals (Table 7). Overall, the average annual capacity for students on clinical rotation was 12 per hospital. The annual range of students on rotation varied from 2 to 150 per hospital, with 143 (21.6%) department directors indicating that they do not take students on clinical rotations.
What is the Maximum Number of Students You Can Take on Clinical Rotation During the Academic Year?
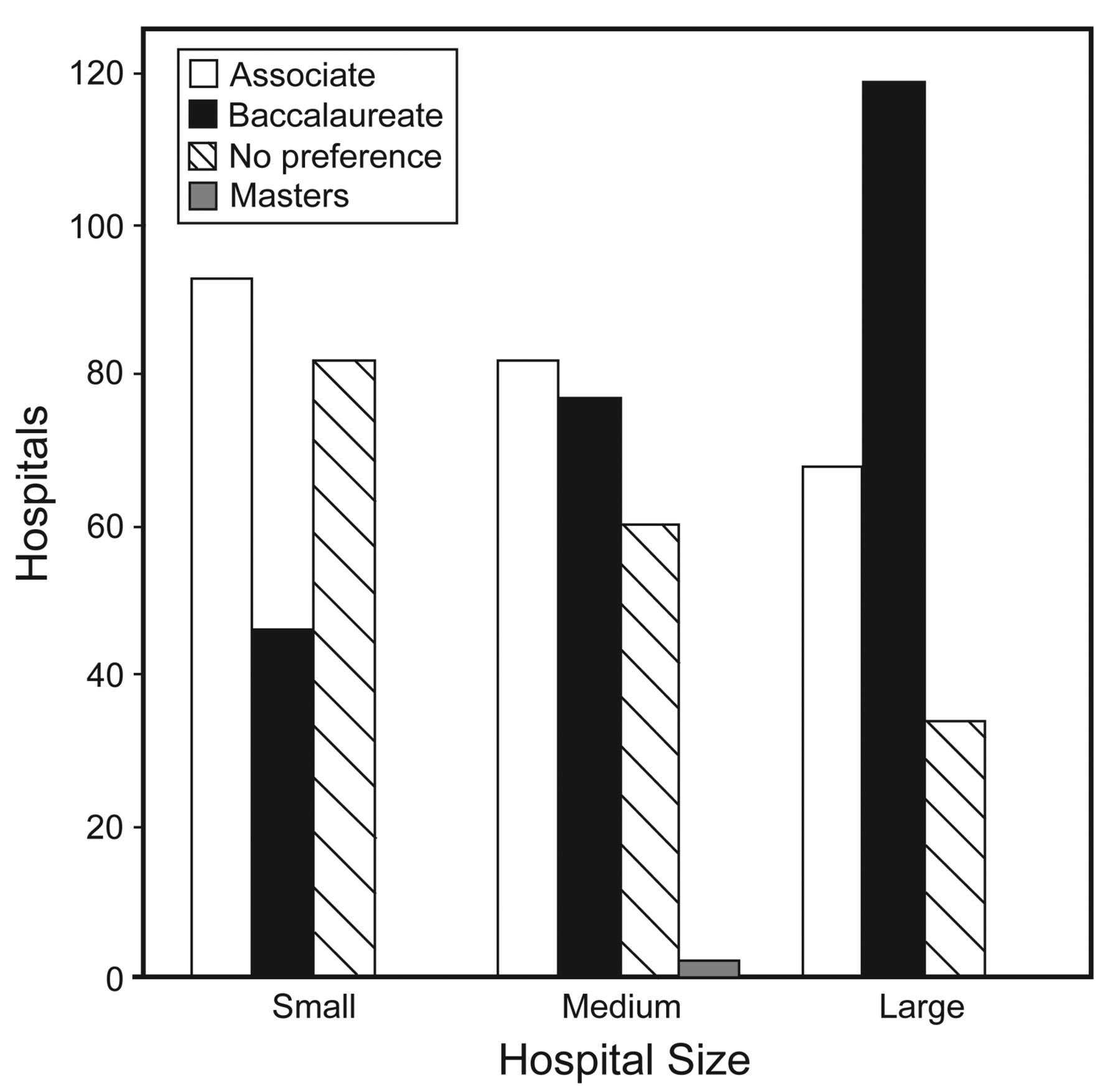
There was no consensus among directors on the academic preparation of new graduates, with 245 (36.8%) indicating a preference for a baccalaureate or master's degree, 243 (36.7%) indicating a preference for an associate degree, and 176 (26.5%) indicating no preference (Fig. 1). Directors were divided on whether to require new graduates to earn the RRT credential within a fixed number of months (Fig. 2). The average orientation time was 6.6 ± 5.6 weeks (585 directors) for new baccalaureate degree graduates, and 7.1 ± 6.5 weeks (662 directors) for new associate degree graduates. The reported time for orientation ranged from 0 to 52 weeks, with a median orientation time of 4.0 weeks for baccalaureate and 6.0 weeks for associate degree graduates. Most directors indicated that graduates met or exceeded their expectations.

Employment preference for education of new graduates, Small = 14–138 beds, medium = 139–344 beds, large = 345–1,533 beds. Number of respondents for each bed size = 221. Total n = 663.
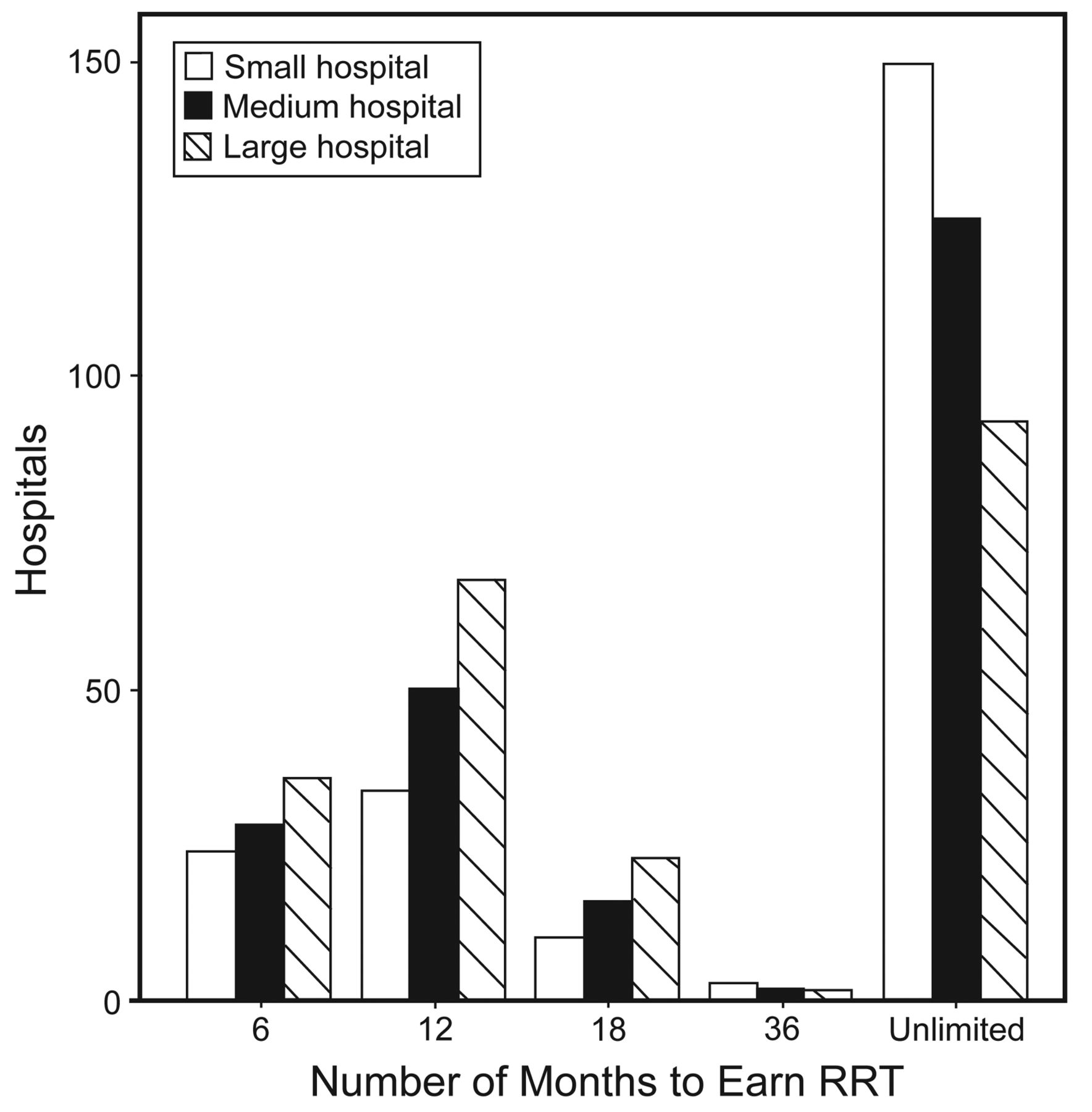
The number of months new graduates are given to earn the Registered Respiratory Therapist (RRT) credential. Unlimited = new graduate is not required to earn the RRT credential. Number of respondents for each bed size = 221. Total n = 663.
There were 270 (41.8%) respondents that indicated that a baccalaureate or master's degree in respiratory therapy should be required to qualify for a license to deliver respiratory care in 2015 and beyond. However, 375 (58.2%) thought the associate degree was all that should be needed to begin practice as an RT (Fig. 3). More agreement on the education level after licensure was observed, with 461 (72.0%) of directors in favor of a baccalaureate or graduate degree to progress in practice (Fig. 4).
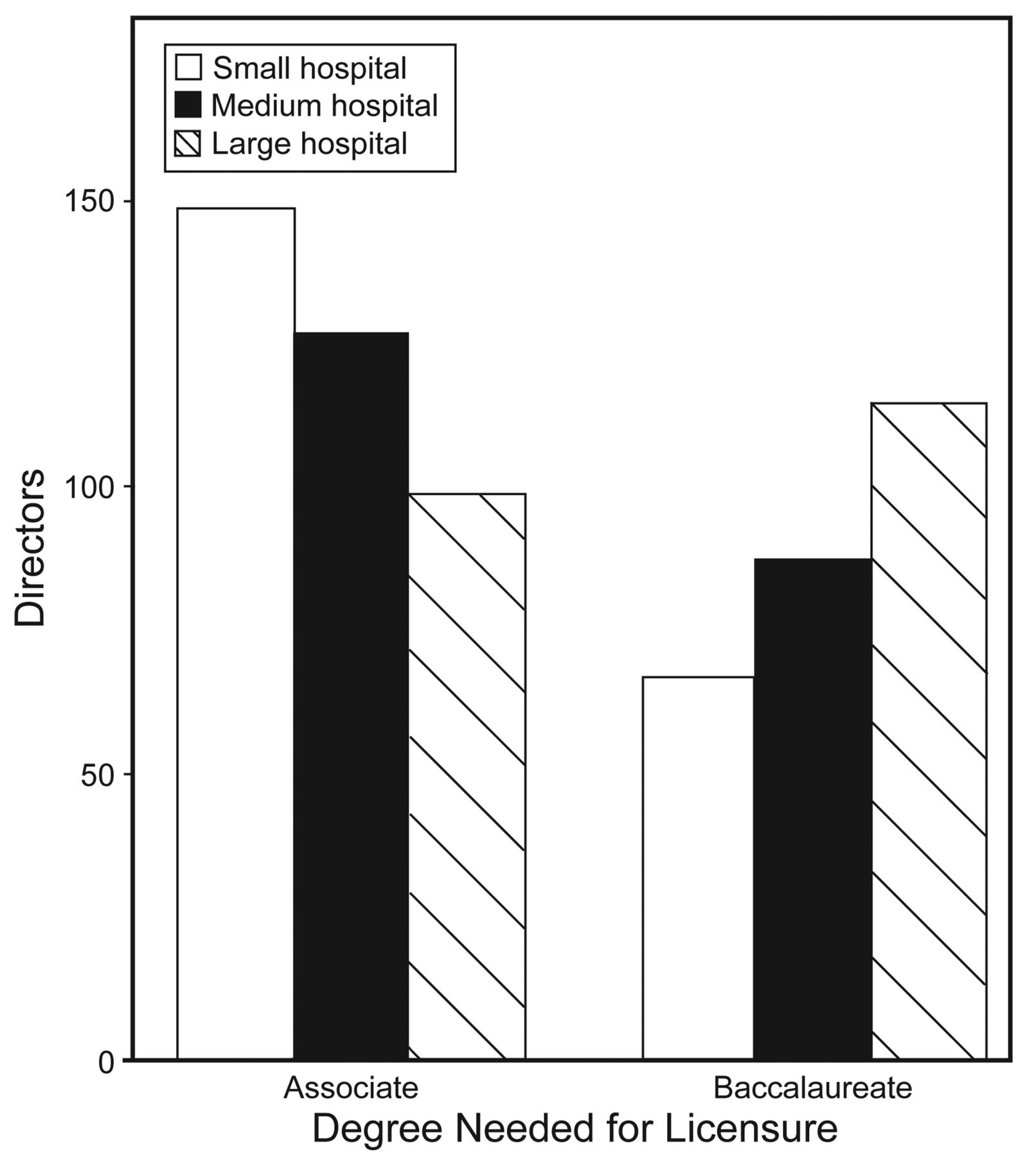
What degree should future graduates be required to earn to be eligible for the examination they take to become licensed and enter practice as a respiratory therapist? Number of respondents for each bed size = 221. Total n = 644.

What degree should future graduates be recommended to earn for continued practice beyond licensure and entry into practice as a respiratory therapist? Number of respondents for each bed size = 221. Total n = 640.
The survey indicates that 523 (81.2%) directors are in favor of the RRT credential being required to practice in 2015 and beyond (Fig. 5). Overall, 518 directors (81.1%) indicated on the survey that future RT graduates should be required to maintain an active Certified Respiratory Therapist (CRT) or RRT credential to renew their state license to practice respiratory care (Fig. 6).

Should future graduates be required to maintain an active Certified Respiratory Therapist (CRT) or Registered Respiratory Therapist (RRT) credential to document competency for renewal of their license to practice in your state? Number of respondents for each bed size = 221. Total n = 640.
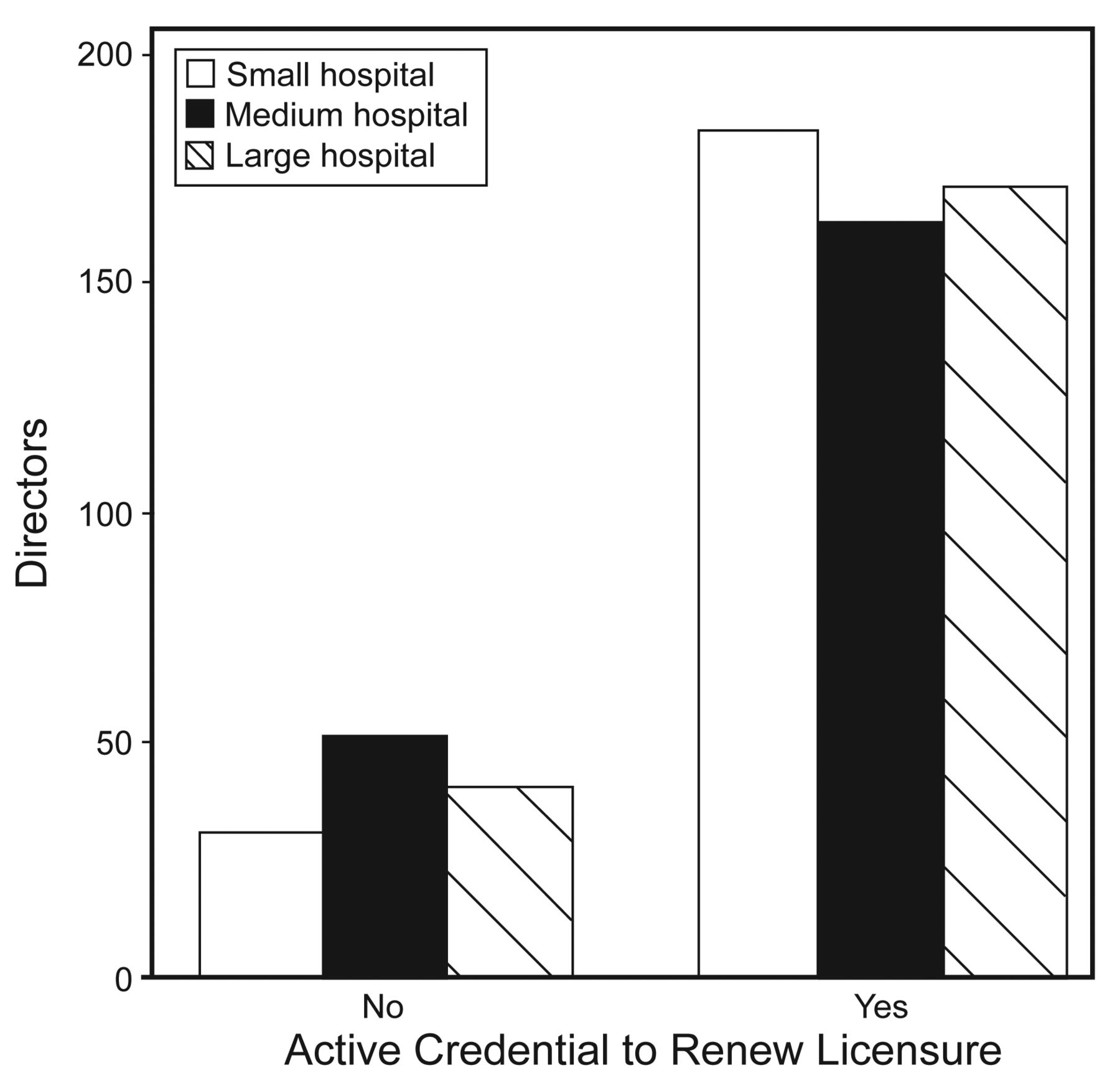
Should future graduates be required to maintain an active Certified Respiratory Therapist (CRT) or Registered Respiratory Therapist (RRT) credential to document competency for renewal of their license to practice in your state? Number of respondents for each bed size = 221. Total n = 639.
Discussion
The major findings of this national survey are:
Greater than 90% agreement was seen by respondents on 37 of 66 competencies that new graduates and existing staff RT will need in 2015.
Between 50% and 90% agreement was indicated on 25 competencies, and less than 50% agreement on only 4 competencies (see Table 2).
The average number of RT staff is projected to increase by 9.9% over the next decade.
While there was no consensus among directors on the academic preparation of new graduates, a vast majority (70.1%) are in favor of a baccalaureate or graduate degree to progress in practice.
Eighty-one percent of directors are in favor of the RRT credential being required to practice in 2015 and beyond. There was no consensus among directors on the academic preparation of new graduates; the majority (71%) were in favor of a baccalaureate (60%) or graduate degree (11%) to progress in practice.
Strong evidence supports the need by 2015 and beyond for graduate RTs to master 66 competencies in 7 major areas.2 The RT in 2015 will have to be able to understand the scientific evidence to deliver healthcare driven by evidence-based medicine.1,4 However, less than a majority (< 44%) of directors indicated that new RT graduates and existing staff should know how to critique published research. Even fewer (< 40%) respondents thought that understanding the meaning of general statistical tests was a needed competency (see Table 4). Yet > 85% of directors expected staff to understand evidence-based medicine as the basis for therapist driven protocol, and an even greater number (> 90%) indicated that disease management was a major competency area needed in 2015 and beyond. However, the RT needs the ability to critique the literature or understand general statistical tests to understand the evidence supporting their roles. Contributing to the disease management model will be a challenge for RTs unless they increase their scope of knowledge and skills in evidence-based medicine. They will need to expand and refine their critical thinking and communication skills, receive training in finance, and increase their ability to analyze the literature.5
Leadership was one of 7 major competency areas identified by the second 2015 conference.2 A high proportion (> 81%) of directors indicated that new RT graduates and staff should lead groups in care planning and bedside decision making, and should collaborate with other healthcare professionals. Over half of the directors indicated that understanding the finances of healthcare and reimbursement and the organizational implications of healthcare regulation were needed competencies (see Table 4). Educational program directors reported in a recent survey that skills for serving as a member or leader of interdisciplinary clinical teams are taught more often by baccalaureate degree respiratory therapy programs than by programs that do not offer the degree.6 This presents a serious challenge for the next decade, based on national survey results that show that only one quarter of accredited RT programs offer a baccalaureate or graduate degree.6 The AARC 2009 Human Resource Study reported that 75% of RT faculty for accredited programs plan to retire by 2020.7 Seven years ago an AARC white paper identified the need for RT graduate programs to prepare RTs for faculty positions in accredited programs.8 However, despite regional accrediting group requirements for baccalaureate level allied health faculty to have a graduate degree in their specialty area, today there are only 4 master's degree and no doctorate programs with majors or concentrations in respiratory therapy.9
There was limited support (< 90%) from directors in 5 of 8 diagnostic competencies (see Table 2). Most of these low scoring competencies were related to sleep medicine. However, the AARC 2009 Human Resource Study Survey of Respiratory Therapists reported that 75.9% of the RT respondents assisted with sleep therapeutics.7 It appears that directors of RT departments in medium and large hospitals responding to our survey have a different opinion on the role of RTs in disease management of sleep disorders. This is inconsistent with the education of RTs, with both baccalaureate (75.9%) and associate degree in respiratory therapy (67.3%) programs teaching students how to apply the results of sleep studies to disease management. Both baccalaureate (92.6%) and associate (83.7%) programs teach students the contraindications and indications for sleep studies.6
Assisting with bronchoscopy is done by 75.3% of RTs responding to the AARC 2009 Human Resources Study Survey of Respiratory Therapists.7 Accordingly, the interest of RT department directors from different size hospitals (59.7% to 74.6%) in these 2 bronchoscopy competencies is consistent with their need (see Table 4). RT educators consider instruction on bronchoscopy to be important, with both baccalaureate (100%) and associate (93.9%) programs teaching this competency.6 Virtually all (> 98%) accredited RT programs teach students to interpret basic spirometry and have a knowledge of the indications and contraindications for advanced pulmonary function tests (baccalaureate 100%, associate 92.2%).6 Further, a high proportion of RT programs teach students to interpret lung volumes and diffusion studies (baccalaureate 98.1%, associate 94.2%).6 Yet < 60% of RT department directors expect existing staff and new graduates to have this competency (see Table 4). A majority of voting participants at the second AARC 2015 and Beyond conference approved these diagnostic competencies as needed in 2015 and beyond.2 Directors of RT departments (n = 662) report that the current FTE RT staff in May 2010 average ± SD per hospital is 32.8 ± 32.5, with a median of 22.0, and a range of 2–230. This is similar to the 2009 AARC Study Survey of Hospital Employers, which reported the FTEs that RT department directors (n = 701) were responsible for as an average ± SD of 32.7 ± 32.9, a mean of 22.0, and a range of 0–200. Our survey asked RT department directors to report FTEs as current staff who graduated from an accredited RT program. The RT workforce in acute care hospitals in 2010 is projected to be 117,222, if one assumes there are 3,583 acute care hospitals7 (defined as a hospital with at least one operating room and 25 beds) with an RT department.
It appears that the economic downturn has affected the future growth of RT departments (see Table 5). The mean ± SD number of open FTE positions reported by department directors for 2010 is only 0.81 ± 1.67, and differs by hospital size, with large hospitals having the most FTE openings (1.48 ± 2.40) and small hospitals the least (0.32 ± 0.48 (see Table 5). The 2009 AARC Study Survey of Hospital Employers reported similar open FTE positions mean ± SD of 1.08 ± 2.77.7 Directors projected an increase in RT department size over the next decade of 9.9% (see Table 5). Assuming that there are 3,583 respiratory care departments in acute care hospitals,7 the RT workforce will expand to 130,449 by 2020. However, it is important to realize that this calculation is based on the current shortage of RTs.
Seventy-eight percent of directors allow students to rotate to their departments for clinical practice (see Table 7). The number of student rotations that can be accommodated in 2010 by 2,809 acute care hospital RT departments (78.4%) is projected (assuming a mean of 12.0 students/hospital) to be 33,708. In May 2010 there were 435 accredited (or seeking accreditation) RT programs.6 Accordingly, it is projected that in 2010 there were 77.5 student rotations available in acute care hospitals for each program. If programs offered 4 clinical courses each year that require clinical rotations, the average number of students that could be accommodated per course would be 19. This is consistent with the average ± SD RT graduating classes in 2009, which was 17.5 ± 12.9.7 Funding of RT educational programs, number of available clinical affiliates, and faculty shortage are reported to be the barriers to accepting more students.6
A high proportion (81.2%) of respiratory therapy department directors or managers surveyed were in favor of the RRT credential being required for licensure to practice as an RT in 2015 and beyond. Further, they can no longer see the rationale for the NBRC to require graduates to take 3 examinations to be awarded the RRT credential. Several survey respondents stated in the comments section that the CRT examination should no longer be offered by the NBRC after 2014. The primary reasons given for this proposed change in credentialing were:
Their departments only hire registered therapists based on the need for the therapist to be involved in research and advanced care.
Advanced knowledge and training are necessary to perform the therapist role, which increasingly involves evaluation, recommendation, and critical thinking skills.
All RT programs in their state are registry-eligible programs, and all graduates are eligible to take the RRT examinations.
The RRT credential is the best method to document that graduates have the necessary skills to perform the job expectations placed upon them.
RT programs prepare students for the RRT credential, and it is time to require it for practice of the profession.
The RRT credential is the recognized “professional” credential. It recognizes the higher level of knowledge and skill needed for today's healthcare changes and challenges.
Considering the competencies that will be required in 2015 and beyond, the RRT requirement for licensure would prepare graduates for their new responsibilities.
The graduate should be able to work as a “graduate therapist” but be required to take their RRT examinations within a specified period of time. If they do not pass the exam, they should not be allowed to provide respiratory care.
If the purpose of legal credentialing is truly to protect the public, basic entry level knowledge is no longer sufficient.
The RRT examinations require more education, and with ever increasing demands on our skills and knowledge, we will need RRT as our minimal standard.
Limitations
This study was limited by the response rate of 28.0%, with 72.0% of the cohort not completing the survey. This was also a limitation of the 2009 AARC Human Resource Survey of RT Department Directors, which only had a corrected response rate of 23.4% (n = 776).7 The response rate for the 2005 AARC Human Resource Survey of RT Department Directors was 22.7% (n = 681).10 The results and conclusions of this survey and the AARC Human Resource Surveys7,10 might have been different if the director response rate was higher. The RT profession needs to encourage directors to be more responsive to surveys that attempt to collect workforce data and the development of the profession in general. When asked about accepting students for clinical rotations, many directors skipped these questions, limiting the results about the number of students that could be taken in 2010 (22.0% skipped), how many hours of clinical practice were given (26.8% skipped), and what the barriers were to accepting students on clinical rotation (13.9% skipped). The number of skipped questions was < 4% in all other items on the survey. A serious concern is how to interpret this selective lack of response on the student clinical rotation data. Did the director simply overlook these items, or was the absence of a response an indication that students were not accepted for clinical rotations? Were the directors simply unable to determine the clinical rotation data? Is it possible that the lack of response was actually a statement that these RT departments do not accept students for clinical practice? If this is so, then the actual percentage of RT departments available for student rotations is much lower than these survey results indicate. The questionnaire did not collect personal characteristics of the respondent (eg, degree, credential, age and duration of practice). It is likely that responses and variation in responses may relate to the personal traits of the directors.
Conclusions
Our study provides important information from directors of RT departments in acute care hospitals regarding changes to the current educational infrastructure that would assure competent providers in the envisioned healthcare future, and on their current and future ability to ensure that graduating students could meet the necessary competencies identified during the 2015 conferences. Other major findings of this national survey are:
Greater than 90% agreement was seen by respondents on 37 of 66 competencies that new graduates and existing staff will need in 2015.
Eighty-one percent of department directors are in favor of the RRT credential being required to practice in 2015 and beyond.
The average number of RT staff in acute care hospitals is projected to increase by 9.9% over the next decade.
While there was no consensus among directors on the academic preparation of new graduates, a vast majority (70.1%) are in favor of a baccalaureate or graduate degree to progress in practice.
Clinical rotation resources need to increase to be able to educate the number of graduates projected for 2015 and beyond.
Footnotes
- Correspondence: Robert M Kacmarek PhD RRT FAARC, Respiratory Care, Warren 1225, Massachusetts General Hospital, 55 Fruit Street, Boston MA 01460. E-mail: rkacmarek{at}partners.org.
Supplementary material related to this paper is available at http://www.rcjournal.com.
Dr Kacmarek has disclosed relationships with Maquet, Newport Medical, Hamilton Medical, Bayer, KCI, and Hollester. Dr Barnes has disclosed a relationship with Mercury Medical. Dr Durbin has disclosed relationships with Kimberly Clark and Masimo. To avoid potential conflict of interest, Editor in Chief Dean Hess was blinded to the peer review process for this paper, which was managed by Deputy Editor Richard Branson.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}