

Abstract
BACKGROUND: Even though it is not a common practice, an external filter to the expiratory limb of the breathing circuit may protect the expiratory valve from water saturation in case of nebulization, or from the environment in case of lung infection with multi-drug-resistant micro-organisms or H1N1 influenza.
METHODS: We added an external filter to the expiratory limb and measured tidal volume (VT) from 6 ICU ventilators: 2 with built-in expiratory filter (Avea, Puritan Bennett 840), and 4 without (Engström Carestation, Evita XL, Evita V500, and Servo-i), set in volume controlled mode, at BTPS (body temperature and pressure saturated) condition, with a heated humidifier and a lung model (compliance 16 mL/cm H2O, resistance 20 cm H2O/L/s) placed inside a neonatal incubator. The temperature was targeted at 37°C for both the heated humidifier and the incubator. The setup was run continuously for 24 hours. In the latter 4 ICU ventilators, a Hygrobac or Sterivent S external filter was placed upstream from the expiratory valve for an additional 24-hour period for each. At the end of this period, VT was measured at 4 nominal VT values (300, 400, 500, and 800 mL) with a pneumotachograph. The volume error computed from the ratio of set to measured VT (% set VT) was the primary end point.
RESULTS: In these warm and wet conditions, volume error averaged 96 ± 3% for Avea, 100 ± 7% for Puritan Bennett 840, 90 ± 2% for Evita XL, 100 ± 7% for Evita V500, 105 ± 2% for Servo-i, and 108 ± 4% for Engström Carestation (P < .001). With the Hygrobac the values were 93 ± 1% for Evita XL, 94 ± 4% for Evita V500, 110 ± 4% for Servo-i, and 99 ± 2% for Engström Carestation (P < .001). With the Sterivent the corresponding values were 95 ± 2%, 105 ± 2%, 112 ± 5%, and 98 ± 2%, respectively (P < .001).
CONCLUSIONS: In BTPS condition, volume error differed substantially across ICU ventilators for VT delivery, with further significant changes occurring after addition of a filter at the distal expiratory limb.
Introduction
During invasive mechanical ventilation in the ICU, a filter may be placed at the distal end of the expiratory limb of the ventilator circuit, upstream from the expiratory valve, while a heated humidifier is used, for 2 purposes. The first purpose is to protect the expiratory valve from humidity in case of nebulization of medication into the inspiratory limb.1–3 A recent survey of ICUs in France, Switzerland, and Belgium has shown that two thirds of those intensivists would use a filter at the expiratory limb of the circuit during nebulization.4 The second purpose is to protect the environment and the healthcare providers from 2 risks: that of airborne contamination in case of lung infection due tomulti-drug resistant microorganisms such as Mycobacterium tuberculosis5,6 or H1N1 influenza,7 and that of toxicity of medications such as ribavirin and pentamidine,8 administered using a nebulizer. Under these circumstances, the filter may become waterlogged while the heated humidifier is running in the ventilator circuit. However, in those ventilator circuits equipped with internal wire heating of the expiratory limb this risk should be minimized. Some ICU ventilators, such as Avea (CareFusion, San Diego, California) and Puritan Bennett 840 (PB840, Covidien, Mansfield, Massachusetts), have such a built-in exhalation reusable filter encompassing the expiratory valve designed to work for a long period of time without the risk of water saturation. Indeed, the filter, which is maintained at an elevated temperature, maximizes the vapor phase of the exhaled humidity and reduces the condensate from the gas.
We wanted to assess whether in BTPS (body temperature and pressure saturated) condition (ie, warmed to 37°C and fully saturated with water vapor by using a heated humidifier switched on) the addition of a filter at the expiratory limb end would result in impairment in ventilator functioning. We raised 3 specific questions. First, does the filter resistance (Rf) increase after 24 hours of heated humidification? Second, if present, was this increase, different between the 2 categories of filters, namely built-in or external? Third, could the delivery of tidal volume (VT) be impaired from this situation? Impairment in VT delivery from the ventilator might occur if the ventilator algorithm that maintains VT constant irrespective of change in humidity, temperature, and ventilatory circuit compliance, is challenged by the new physical environment. Our hypothesis for the first 2 questions was that Rf would increase with humidification and that the magnitude of this would be higher with external than with built-in filters. Our hypothesis for the third question was that VT delivery was impaired to a greater extent with an external than with an built-in filter. Therefore, we investigated these questions on the bench.
QUICK LOOK
Current knowledge
The hallmark of lung-protective ventilation is low tidal volume (VT) based on the patient's predicted body weight. Ventilators deliver VT with different algorithms, and expired VT is calculated with different correction factors.
What this paper contributes to our knowledge
There were significant differences in the set VT and measured VT between ventilators. The addition of a breathing circuit filter to the expiratory limb worsened the volume error.
Methods
Experimental Setup
We implemented the following setup to replicate the hygrometric conditions of clinical practice as close as possible. Six ICU ventilators were tested: Avea, PB840, Engström Carestation (GE Healthcare, Madison, Wisconsin), Servo-i (Maquet, Wayne, New Jersey), Evita XL (Dräger, Lübeck, Germany), and V500 (Dräger, Lübeck, Germany). They were provided with and fully checked by the manufacturers before the investigation.
The following external filters were used: the hydrophobic Sterivent S (Cardinal Health/CareFusion, San Diego, California), and the hygroscopic/hydrophobic Hygrobac (Mallinckrodt/Covidien, Mansfield, Massachusetts) heat and moisture exchanger (HME). With both filters, the bacterial/viral filtration efficiency is greater than 99.999%. The filtration is mechanical with the former and electrostatic with the latter. The pressure drop at 1 L/s flow (V̇) given by the manufacturer for each filter is 1.9 and 2.1 cm H2O, respectively. For the disposable filters designed for use with the PB840 and Avea, the bacterial/viral filtration efficiency is greater than 99.999%, and the pressure drop is < 2.5 cm H2O and 4 cm H2O at 1.7 L/s V̇, respectively.
Specifications regarding ICU ventilators and filters provided by the manufacturers are shown in Table 1. The present ICU ventilators were equipped with a double heated-wire hot water circuit (RT200 dual heated circuit with MR290, Fisher & Paykel, Auckland, New Zealand) and a heated humidifier (MR850, Fisher & Paykel, Auckland, New Zealand). The ventilator was attached to a lung model (Test Lung 190, Maquet, Wayne, New Jersey) whose compliance was 16 mL/cm H2O and resistance was 20 cm H2O/L/s. The lung model was placed vertically in a neonatal incubator (Isis MP4, Médipréma, Tauxigny, France) (Fig. 1) during some parts of the experiment (see below). Both the lung model and the incubator were tightly linked to avoid any leak (see Fig. 1).
Features of the Tested Ventilators
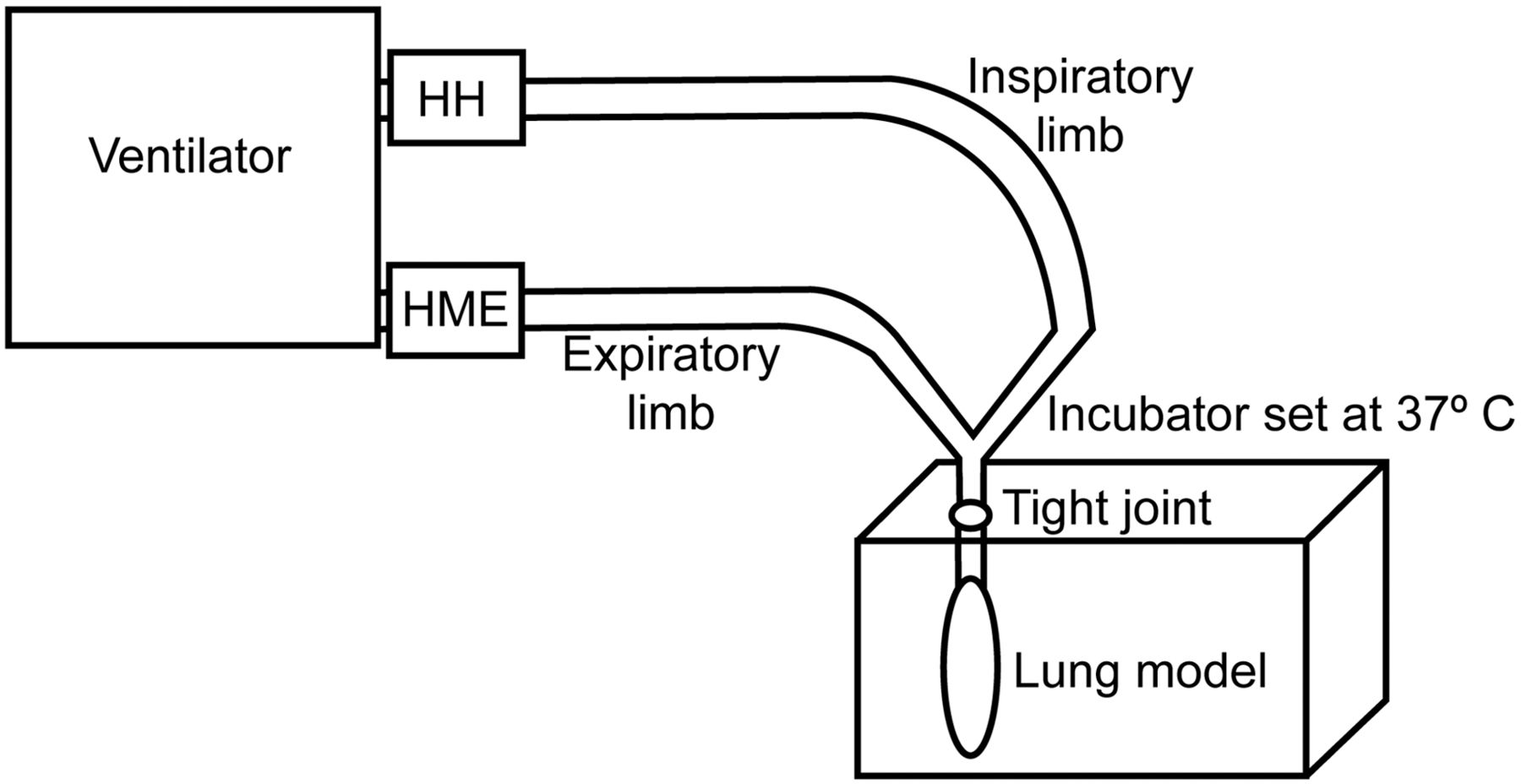
In vitro experimental setup. HH = heated humidifier. HME = heat and moisture exchanger.
V̇ was measured by using a pneumotachograph (3830/4830, Hans-Rudolph, Shawnee, Kansas), which was linear over ± 10 L/s V̇ range. V̇ ports were connected to piezoresistive transducers (BD Gabarith, Vogt Medical Vertrieb, Karlsruhe, Germany). Pressure at the airway opening (Pao) was measured by using a straight connector (VBM Medizintechnik, Sulz am Neckar, Germany). The signals were amplified, sent to analog-digital hardware (MP150, Biopac Systems, Goleta, California), and recorded at 400 Hz (Acqknowledge, Biopac Systems, Goleta, California).
Protocol
The piezoresistive transducers were calibrated before the measurements were taken, using a rotameter flow meter (Martin Médical, Lyon, France) for V̇ and manometer (717 1G, Fluke Biomedical, Everett, Washington) for Pao. The protocol was as follows (Table 2).
Investigation Steps Summary
First Step: Assessment of Filter Air-Flow Resistance in ATPD Condition (dry gas at ambient temperature and pressure).
Each built-in or external filter was attached at the Y-piece of a ventilatory circuit (breathing circuit, Mallinckrodt/Covidien, Mansfield, Massachusetts) connected to a ventilator (Xtend, Taema, France). V̇ was varied from 0.2 L/s to 2 L/s, by steps of 0.2 L/s, while V̇ and Pao signals were recorded.
Second Step: Measurement of Delivered VT and Comparison With Set VT in ATPD Condition With Ventilator Set in BTPS.
After complete check, the ICU ventilator under investigation was set in BTPS. Four nominal values of set VT were defined as 300, 400, 500, and 800 mL. Each nominal VT was applied for 1 min, while V̇ and Pao signals were recorded.
Third Step: Measurement of Delivered VT and Comparison With Set VT in BTPS Condition (gas at 37°C and fully saturated with water vapor) Maintained During 24 Hours Without External Filter.
The ICU ventilator set in BTPS was connected to the incubator, with both heated humidifier and incubator switched on, and 37°C temperature targeted. The heated humidifier was filled with 500 mL sterile water vial, after we had verified that this amount supplied the chamber for 24 hours. Once the targeted temperature was reached, the setup was run for 24 consecutive hours. A probe was inserted every 6 hours into the incubator to check for temperature to ensure maintenance at the desired level. At the end of this period, the measurement setup was attached. VT was changed to 300, 400, 500, and 800 mL for 1 min each with heated humidifier in use while V̇ and Pao signals were recorded.
Fourth Step: Measurement of Delivered VT and Comparison With Set VT in BTPS Condition Maintained During 24 Hours With External Filter Added.
For the 4 ventilators with no built-in expiratory filter (Engström Carestation, Evita XL, Evita V500, and Servo-i), external filters were inserted at the ventilator circuit expiratory end, upstream of the expiratory valve. Each filter was applied in a random order and the setup ran for 24 hours. At the end of each 24-hour period, VT was changed to 300, 400, 500, and 800 mL for 1 min each, with heated humidifier in use while V̇ and Pao signals were recorded.
Fifth Step: Measurement of Rf in BTPS Condition.
At the end of each 24-hour running out period, the built-in reusable filters and external filters were removed from the setup and attached at the Y-piece of a ventilator circuit (breathing circuit, Mallinckrodt/Covidien, Mansfield, Massachusetts) connected to a ventilator (Xtend, Taema, France). V̇ was varied from 0.2 L/s to 2 L/s, by steps of 0.2 L/s, while V̇ and Pao signals were recorded.
Data Analysis
Pao and V′ were fitted to the following equation:
Inspiratory VT was obtained by numerical integration of the V̇ signal. VT was measured in the 3 last consecutive breaths.
Statistical Analysis
The primary end point was determination of the ratio of set to measured VT (expressed as percentage of set VT) and named volume error. For the statistical analysis we used analysis of variance to compare the volume error between ventilators in BTPS condition without an external filter at each level of nominal VT. We also compared the difference in volume error between absence and presence of external filter across the ventilators at each level of nominal VT and kind of external filter. When the overall effect was statistically significant, we performed post hoc pairwise comparisons to Avea or PB840 taken as control, by using the Dunnett test, where an overall statistically significant effect of the ventilator was found. The difference in volume error between absence and presence of external filter was negative if volume error was greater with than without external filter for Evita XL, Evita V500, Engström Carestation, and Servo-i. This difference was equal to zero for Avea and PB840. Therefore, comparing volume error for Evita XL, Evita V500, Engström Carestation, and Servo-i to Avea or PB840 as control pertained to comparing volume error to zero.
The difference in volume error between ATPD and BTPS conditions for each ventilator set in BTPS was tested by using paired t tests at each nominal VT. Bonferroni correction was applied. The constants K1 and K2 were obtained by using linear regression.
The values are expressed as mean ± 1 SD unless otherwise stated. The statistical analysis was carried out using statistics software (SPSS 17.0, SPSS, Chicago, Illinois). P < .05 was set as the threshold for statistical significance.
Results
Resistance of Filters
Under ATPD condition both external filters exhibited similar ΔP-V̇ relationships and higher Rf than built-in filters (Fig. 2). The coefficient of determination was greater than 0.98 in all instances (P < .001). Under BTPS condition, Rf became greater for Sterivent than Hygrobac. In BTPS condition, Rf increased for PB840 and did not change for Avea, so that Rf of both built-in filters were similar and markedly lower than Rf of external filters (see Fig. 2). Rf computed at 1 L/s from constants K1 and K2 (see Fig. 2) were 0.56 and 0.66 for Avea, 0.43 and 0.77 for PB840, 1.57 and 1.71 for Hygrobac, and 1.64 and 2.53 cm H2O/L/s for Sterivent in ATPD and BTPS conditions, respectively.

Pressure drop (ΔP) versus air flow for built-in expiratory filters and external filters in ATPD (ambient temperature and pressure dry) and BTPS (body temperature and pressure saturated [wet]) conditions.
Volume Error Under BTPS Condition Without External Filter
After 24 hours working at 37°C, there was a significant effect of the ventilator, the set VT, and their interaction on volume error (Fig. 3). Volume error was within 10% limits of set VT in all instances but for the following exceptions: Evita XL at VT 300 and 400 mL, PB840 at VT 800 mL, and Servo-i at VT 300 mL. Volume error ranged from 86% to 113% across all VT for all ventilators. It averaged 96 ± 3% for Avea, 100 ± 7% for PB840, 90 ± 2% for Evita XL, 100 ± 7% for Evita V500, 108 ± 4% for Engström Carestation, and 105 ± 2% for Servo-i (P < .001). At each nominal VT, volume error was statistically significantly different from each control (see Fig. 3). In all ventilators but Evita XL, volume error decreased with increased nominal set VT.

Mean volume error (% of set tidal volume [VT]) with 6 ventilators during BTPS (body temperature and pressure saturated) conditions without external filter. The error bars indicate the standard deviations. * P < .05 versus Puritan Bennett 840 (PB840). † P < .05 versus Avea.
Effect of External Filter on Volume Error
With external filter, volume error further changed from the baseline (without external filter) (Fig. 4). Except for Evita XL at 800 mL, all differences were significantly different from zero, and henceforth from Avea or PB840 (see Fig. 4). There was a negative difference in volume error (ie, volume error increased between the 2 conditions, without and with the external filter, with Evita XL and Evita V500, while the difference was positive with the 2 others). Adding an external filter shifted volume error with Evita XL toward 100% (Figs. 3 and 4), and largely above 100% (above 120% at VT 300 mL) with Evita V500 (Figs. 3 and 4). Volume error was close to 100% for Engström Carestation, and between 100% and 108% with Servo-i (Figs. 3 and 4).

Mean differences in volume error (% of set tidal volume [VT]) between absence and presence of an external filter (Sterivent or Hygrobac). A negative difference means greater volume error with than without external filter, and the opposite is true for a positive difference. For the Avea and Puritan Bennett 840 (PB840) the difference was zero (no difference between with and without external filter). The error bars indicate the standard deviations. * P < .05 versus zero.
The magnitude of change in volume error was significantly greater with Hygrobac than Sterivent for Servo-i at the 4 nominal set VT, for Engström Carestation at VT 800 mL, and for Evita V500 at VT 500 mL. The volume error range in the 4 ICU ventilators was 90–117% with Hygrobac and 92–122% with Sterivent. With Hygrobac the volume error averaged 93 ± 1% for Evita XL, 94 ± 4% for Evita V500, 99 ± 2% for Engström Carestation, and 110 ± 4% for Servo-i (P < .001). With Sterivent, the corresponding values were 95 ± 2%, 105 ± 2%, 98 ± 2%, and 112 ± 5% (P < .001).
ATPD Versus BTPS Condition While the Ventilator Is Set in BTPS
Volume error was systematically greater, except for Evita XL at VT 300 mL (Fig. 5), in BTPS condition without external filter than in ATPD condition with the ventilators set in BTPS, in both instances. The level of statistical significance was reached in some instances (see Fig. 5).

Mean volume error (% of set tidal volume [VT]) at 4 nominal set VT in BTPS (body temperature and pressure saturated) (black bars) and ATPD (ambient temperature and pressure dry) (white bars) conditions with 6 ICU ventilators on which BTPS was set. * P < .05 versus dry.
Discussion
In this bench study performed in BTPS condition, we found significant differences in volume error across ventilators, further significant changes in volume error by adding external filters in 4 ICU ventilators, and lower Rf for built-in than for external filters.
One strength of the present study was to investigate the volume error in VT from ICU ventilators while temperature and humidity conditions were maintained close to those in the clinical setting for 24 hours. It should be stressed that in the present study the term BTPS refers to both a setting on the ventilator and a condition with which the ventilator is being tested. Bench studies are commonly done by using ICU ventilators fed by cold and dry air and set in ATPD. Such design may not reflect in vivo hygrometric conditions. When correction for BTPS condition is applied, the VT measured in ATPD condition has unexpectedly been found markedly different across ICU ventilators.9 This may be due to the fact that the algorithms that work for the ICU ventilators to deliver VT as close as possible to set VT differ across the ventilators once BTPS conditions are present. Facing heated inspired air, the algorithm should decrease the amount of gas that exits from the ventilator, because heating expands the gas. At the same time, the algorithms should increase the amount of gas expelled from the ventilator to compensate for the gas compression into the inspiratory limb in relation with the compliance of the latter and the inspiratory pressure. In the bench study quoted above,9 the measurements were performed under ATPD conditions and VT was derived to BTPS conditions from computation. The present study was done in actual BTPS conditions with algorithms activated.
Let us compare the values of volume error BTPS computed (see Fig. 2 in Lyazidi et al9) or BTPS measured (see Fig. 3 in the present work) in those 5 ICU ventilators investigated in both studies. In the Lyazidi et al9 study, at nominal set VT of 300, 500, and 800 mL the volume error was in the range 100–105% for PB840 and Evita XL, and in the range 105–115% for Avea, Servo-i, and Engström Carestation. The present findings do not confirm these results except for Servo-i. As an example, the volume error under BTPS condition in the present study was largely < 100%, as for PB840 and Engström Carestation at VT 800 mL. Several reasons may explain these discrepant results. First of all, the measurements in the study by Lyazidi et al9 were done in ATPD and extrapolated to BTPS by using a computation. The present results were obtained with the ICU ventilators' set BTPS algorithms turned on, and with heated humidifiers switched on. The comparison of volume error between ATPD condition and BTPD condition without filter with the ICU ventilator set in BTPS in both instances can shed light on this apparent discrepancy (see Fig. 5). The actual BTPS condition was systematically, with one exception, associated with greater volume error than the ATPD condition, whereas the BTPS algorithm was activated in the ventilator. This would suggest that the actual condition plays a major role and may even impair the function of the algorithm. Second, the ICU ventilators presently tested may be equipped with more recent algorithms than those tested by Lyazidi et al.9 Indeed, manufacturers take into account the results of bench testing to regularly improve the algorithms.
Some findings in the present study were not clearly explained. It was a unique feature for Evita XL that volume error increased with increasing nominal set VT. The other ventilator from the same manufacturer did not exhibit this behavior. Volume error was greater without than with filters in 2 ventilators, and the opposite was true for the other 2 ventilators (see Fig. 4). Both ICU ventilators of the same manufacturer behaved similarly with each filter. These results suggest that the delivery of VT was different in all ventilators with this additional filter.
Others measured Rf, as we did, over time on the bench. Pelosi et al10 measured Hygrobac's Rf after 24 and 48 hours of mechanical ventilation with heated humidifier. They found baseline Rf values very close to the present ones. They also found, as in the present study, a slight increase of Rf over time. Lucato et al11 investigated, among other filters, Hygrobac S, which has both hygroscopic and hydrophobic properties. They found greater Rf values than in the present study and a significant increase from 2 to 3.8 cm H2O/L/s after water saturation. It should be noted that Rf was measured in the bench, set in spontaneous or in pressure support ventilation. Furthermore, the saturation was induced by manual saline instillation inside the external filter, which is clearly not the same process as heating and humidifying. High Rf value has been also reported for Hygrobac S by others.12 Lellouche et al13 found that the pressure drop measured at 1 L/s was 2 cm H2O for Hygrobac and 1.9 cm H2O for Sterivent after a 3-hour exposure to a wet environment. This latter value was lower than that presently found, a discrepancy that can be explained by difference in time frame.
Clinical Implications
According to the present results, for a preset VT of 6 mL/kg predicted body weight, delivered VT would be in the range of 5.2–6.8 mL/kg in BTPS condition without external filter, and 5.4–7.3 mL/kg in BTPS condition with external filter. Therefore, the errors are in the range of 1–2 mL/kg. The addition of external filter at the expiratory limb to protect the expiratory valve or environment had a significant effect on the delivery of VT, which was different across ICU ventilators. This effect was not related to Rf, but, rather, to the internal structure of the filter.
Limitations
First of all, we added filters at the expiratory limb of the ventilator circuit. HMEs are not to be used as a filtering device on the expiratory limb, as they are not designed for it. Even though this statement is sound, in the most recent American Association for Respiratory Care clinical practice guideline on humidification during mechanical ventilation, no specific contraindication to locating an HME at the expiratory limb of the ventilator circuit was mentioned.14 It could be argued that heating the expiratory limb, as done by the kind of ventilator circuit we used, may prevent the filter from water saturation.
By study design we had to use a lung model that imposed on the ventilators severe respiratory mechanics impairment. Different results might have been obtained with other mechanical conditions. A longer period than the 24 hours used might have disclosed findings of different amplitude. Few ICU ventilators were tested. Finally, we did not assess the reproducibility of measurements across external filters.
Conclusions
In actual BTPS condition, volume error in VT delivery differed substantially across ICU ventilators, with further significant changes occurring after addition of an external filter at the expiratory limb.
Acknowledgments
The authors wish to thank Daniel Gouzou, bioengineering technician, and Jean-Loup Carraz-Billat, medical bioengineer, both at Croix Rousse Hospital, Lyon, France, for their help in fixing the experimental setup and Jérôme Girard, Sebac, France, for feedback and support.
Footnotes
- Correspondence: Claude Guérin MD PhD, Service de Réanimation Médicale et d'Assistance Respiratoire, Hôpital de la Croix Rousse, 103 Grande Rue de la Croix Rousse, 69004 Lyon, France. E-mail claude.guerin{at}chu-lyon.fr.
The authors have disclosed relationships with CareFusion, Covidien, GE Healthcare, Maquet, and Dräger, which provided the ventilators for this study.
- Copyright © 2013 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}