

Abstract
It has been shown that mechanical ventilation by itself can cause lung injury and affect outcomes. Ventilator-induced lung injury is associated with high tidal volumes in lungs afflicted with ARDS. However, the question is: Do high tidal volumes have this same effect in normal lungs or lungs that have respiratory compromise stemming from something other than ARDS? Many clinicians believe that a tidal volume strategy of 6 mL/kg predicted body weight should be standard practice in all patients receiving mechanical ventilation. There is a growing body of evidence related to this issue, and this is the debate that will be tackled in this paper from both pro and con perspectives.
- tidal volume
- predicted body weight
- mechanical ventilation
- lung-protective ventilation
- time constant
- ARDS
- stress
- strain
- hypercapnia
Introduction
It is well known that the use of mechanical ventilation has the potential to aggravate pulmonary injury, but emerging evidence indicates that it may also precipitate lung injury in patients with no previous injury. Lung-protective ventilation has evolved over the past couple of decades to the point that it has become standard of care for patients with ARDS. The use of lower tidal volume (VT) values, 4–8 mL/kg predicted body weight (PBW) is part of this lung-protective strategy for mechanical ventilation (mechanical ventilation) along with limiting the plateau pressure to a maximum of 30 cm H2O and prudent use of PEEP to prevent atelectasis. Since we now know that the use of lower VT strategies (more specifically 6 mL/kg PBW) helps to limit the pulmonary damage during ARDS, the question now is: Should we be using this strategy in all mechanically ventilated patients? Anatomically speaking, it makes sense to, since the normal physiologic VT for humans is approximately 6 mL/kg PBW.1 There is a growing body of evidence that points toward the use of lower VT values leading to improved outcomes in patients suffering from other forms and degrees of respiratory failure. The aim of this paper is to examine the evidence relating to the use of lower VT values in conditions other than ARDS in which mechanical ventilation is required. This will be done with viewpoints from both the pro and con positions.
Early Studies
There is a plethora of preclinical evidence from animal studies supporting the fact that the use of high VT values can directly cause injury to normal lungs. Animal studies have shown that high VT ventilation increases levels of pro-inflammatory mediators, leads to pulmonary edema, and causes increased alveolar-capillary permeability and structural abnormalities.2–8 With the emergence of these animal data, clinicians began to question the traditional use of VT values in the range of 10–15 mL/kg PBW in humans. Several small human studies were reported in the mid- to late 1990s that produced conflicting results.9–11 These studies were hampered by several factors, including higher than predicted mortality in the control group, a relatively small difference in VT between the groups, insufficient statistical difference to detect a signal, and uncorrected acidosis in the low VT group. However, in 2000, a landmark study comparing lower VT values (6 mL/kg PBW) with higher VT values (12 mL/kg PBW) in ARDS was undertaken by the ARDS Net group. It was a large multi-center prospective randomized trial with >800 subjects enrolled. The study was stopped early after an interim analysis revealed a survival advantage of 22% in the lower VT group.12 Since the publication of this study, there has been a growing body of evidence that suggests that the use of lower VT values may also improve clinical outcomes in patients without ARDS.
Ventilation of Patients Who Do Not Have ARDS
Although mechanical ventilation strategies are slowly gravitating toward the use of lung-protective ventilation, many clinicians have not adopted the practice in all patients. The use of high VT values in patients with ARDS clearly appears to be detrimental in that it rapidly results in pulmonary changes that mimic and amplify the ARDS inflammatory process.2,12 The biophysical injury in ARDS lungs consists of overdistention of recruited alveoli, direct cell damage due to cyclical opening and closing of unstable alveoli, and loss of surfactant function.13 What we do not know for sure is whether higher VT values have this on effect on normal lungs.
Shortly after the ARDS Net study in 2000, Gajic et al14 conducted a retrospective cohort study of 332 medical-surgical subjects receiving mechanical ventilation for >48 h who did not have acute lung injury (ALI) at the onset of mechanical ventilation. They found that 80 subjects (24%) developed ALI within the first 5 d and, on average, within the first 3 d.14 They concluded that there existed 2 important risk factors for the development of ALI: large VT values and the administration of blood products. Figure 1 illustrates that, as VT increased, the ALI rate also increased.14 The same group then followed up with an analysis of a large international mechanical ventilation database of subjects who received mechanical ventilation for >48 h but did not have ARDS at the outset. Of 3,261 subjects, 205 (6.2%) developed ARDS. The initial ventilator settings, in particular the VT, were associated with the development of ARDS.15 Of note, as was the case with the ARDSNet study, the initial static respiratory system compliance was better in the group that went on to develop ARDS (higher VT group). Thus, it is important to keep in mind that the use of surrogate end points, such as compliance, do not necessarily correlate to mortality.

Proportion of acute lung injury (ALI) with respect to tidal volume (VT). VT <9 mL/kg predicted body weight (PBW) (n = 66), VT = 9–12 mL/kg PBW (n = 160), and VT >12 mL/kg PBW (n =100). Adjusted P value from a multiple logistic regression model; VT was treated as a continuous variable. From Reference 14, with permission.
Mascia et al16 conducted a prospective, observational study of 82 mechanically ventilated subjects with severe brain injury but with otherwise healthy lungs. In this population, 18 subjects (22%) developed ALI. The subjects with ALI were initially ventilated with a significantly higher VT (10.4 mL/kg) compared with subjects without ALI. Risk factors for ALI were VT, breathing frequency, and expiratory minute volume. Later, the same group examined 118 subjects who were deemed potential organ donors. This was a randomized controlled trial in 12 European ICUs that compared conventional ventilation (VT = 10–12 mL/kg and 3–5-cm H2O PEEP) with protective ventilation (VT = 6–8 mL/kg and 8–10-cm H2O PEEP). The results revealed an dramatic increase in the number of eligible lung donors: 32 (54%) versus only 16 (27%, P = .004) in the conventional group, suggesting that lower VT values may have a role in lung preservation.17
In a large prospective randomized controlled trial, Determann et al18 compared the use of 6 mL/kg PBW VT with 10 mL/kg PBW VT in 150 mechanically ventilated intensive care subjects. The trial was stopped early because the rate of lung injury development was 13.5% in the 10 mL/kg VT group compared with only 2.6% in the 6 mL/kg VT group. The investigators also found significantly higher lavage fluid cytokine levels in the 10 mL/kg VT group. Also, the 6 mL/kg PBW group did not require additional sedation or hemodynamic support.18 In a smaller randomized controlled trial of 20 subjects without lung disease, the subjects received either VT values of 5–7 mL/kg PBW or 10–12 mL/kg PBW in the ICU setting. Tumor necrosis factor alpha and interleukin 8 were measured in both the serum and bronchoalveolar lavage fluid at admission and then again at 12 h. Whereas levels of both tumor necrosis factor alpha and interleukin 8 increased initially, the pulmonary inflammatory response in the low VT group became attenuated at 12 h.19
A secondary analysis of 3 prospective observational multi-center studies from 1998, 2004, and 2010 looked at ventilator management and complications over that span. A total of 812 subjects who received mechanical ventilation after cardiac arrest were studied. The group found that the use of protective ventilation increased from 1998 to 2010, and pulmonary complications decreased in that time span.20 The investigators concluded that the use of higher VT was a potential risk factor for developing pneumonia and ARDS.20
In 2012, Serpa Neto et al21 performed a meta-analysis of 20 studies, 15 of which were randomized controlled trials (2,822 subjects receiving mechanical ventilation who did not have ARDS initially). They found evidence that the use of lower VT was associated with a lower risk of developing ARDS, lower mortality rate, fewer pulmonary infections, and a shorter hospital stay. The same group followed up with a patient-specific meta-analysis of mechanically ventilated subjects without ARDS at the onset of ventilation. The meta-analysis included 5 randomized controlled trials and 5 observational studies. The subjects were stratified into 3 groups: (1) VT ≤6 mL/kg PBW, (2) VT = 6–10 mL/kg PBW, and (3) VT ≥10 mL/kg PBW. The findings of this study were that VT values ≤6 mL/kg PBW were associated with more subjects breathing without assistance at day 28 and more ventilator-free days.22 The Serpa Neto group then went on to perform a third meta-analysis in 201523 with the primary outcome being pulmonary complications (ARDS and pneumonia) in subjects without ARDS at the time of intubation. As in the previous meta-analysis, they stratified the subjects into 3 groups: (1) VT ≥10 mL/kg PBW, (2) VT >7 and <10 mL/kg PBW, and (3) VT ≤7 mL/kg PBW) during the first 2 d of mechanical ventilation. The results are depicted in Table 1. The results suggested a strong correlation for protective ventilation and low VT values in that the risk of pulmonary complications decreased by 28% in the low VT group compared with the high VT group (P = .042).23 The development of pulmonary complications was associated with a lower number of ICU-free and hospital-free days (10.0 ± 10.9 d vs 13.8 + 11.6 d, P < .001) and increases in hospital mortality (49.5 vs 35.6, P < .001).23 The results also suggested a dose-response relationship between the size of the VT and the development of pulmonary complications.23
Pulmonary Complication Rate for Each Tidal Volume Range
The evidence presented above is suggestive of the fact that larger VT values lead to increases in pulmonary pro-inflammatory mediators and pulmonary complications in ICU patients who do not initially present with ARDS. However, large randomized controlled trials are needed to better establish the use of low VT values in this patient population. More liberal use of low VT values certainly, however, seems warranted for those patients who have risk factors for the development of ARDS.
Ventilation of Surgical Patients
Postoperative pulmonary complications have been associated with increases in morbidity and mortality in patients undergoing major surgery.24 Postoperative ARDS represents the worst pulmonary complication, and its occurrence has been estimated as high as 25%.25–27 Increases in morbidity and mortality may be, at least somewhat, attributable to the practice of historically using high VT in the range of 10–15 mL/kg PBW and no PEEP. This practice of using high VT without PEEP in the operating room was introduced back in 1963 as a means of improving oxygenation and avoiding atelectasis and remains as a strategy still being used by many today.28 Despite the publication of the ARDSNet landmark paper in 2000 showing that lower VT resulted in a mortality benefit as compared with the traditional VT of 12 m/kg PBW, this strategy has been slow to be employed in the surgical arena.29 However, over the past decade, there have been encouraging indications that lung-protective ventilation is being used more frequently in the operating room.30
Since many surgical procedures are of relatively short duration, the focus on lung-protective ventilation is placed on the back burner by many anesthesiologists. However, it has been shown that pulmonary inflammatory damage can occur after only a few hours.31 Although information about the pulmonary side effects of mechanical ventilation in the operating room has historically been limited, there are a growing number of studies showing that the use of high VT values in surgical patients has deleterious effects. Schilling et al32 studied 32 subjects undergoing open thoracic surgery and compared the use of low VT (5 mL/kg PBW) versus high VT (10 mL/kg PBW) strategies. They found that in all subjects, there was an increase in pro-inflammatory mediators. However, several of the pro-inflammatory markers (tumor necrosis factor alpha and soluble intercellular adhesion molecule 1) were significantly decreased in the low VT group over time. The authors concluded that the use of mechanical ventilation may promote the production and release of pro-inflammatory substances in the alveoli, resulting in epithelial damage. They further concluded that the use of lower VT values may aid in decreasing some of the pro-inflammatory mediators.32 Michelet et al33 prospectively investigated 52 subjects who underwent an esophagectomy, comparing high (9 mL/kg PBW) and low VT (5 mL/kg PBW) strategies. As was the case in the study by Schilling et al,32 the lower VT group had lower blood levels of pro-inflammatory mediators, improved PaO2/FIO2, and a reduction in the duration of intubation. Another study also examined the relationship between the size of the VT and the pro-inflammatory response in subjects undergoing various surgical procedures lasting ≥5 h. Wolthuis et al34 compared high VT (12 mL/kg) and no PEEP with protective ventilation of 6 mL/kg and 10-cm H2O PEEP and found that the use of lower VT attenuated the increase of pulmonary levels of pro-inflammatory mediators.
It certainly appears from the above mentioned studies that there is an increase in pulmonary inflammation that is associated with mechanical ventilation and that using lower VT values seems to have the potential to attenuate this inflammatory response. Whether this translates into a mortality outcome benefit remains to be seen.
Several investigators have studied the association between VT size and the development of postoperative respiratory complications. Futier et al35 studied 400 subjects undergoing abdominal surgery who were at risk of developing postoperative pulmonary complications and assigned the subjects to receive either non-protective ventilation (VT = 10–12 mL/kg PBW and no PEEP) or lung-protective ventilation (VT = 6–8 mL/kg PBW and PEEP = 6–8 cm H2O along with recruitment maneuvers). They found that pulmonary complications occurred in 27.5% of the subjects in the non-protective group compared with only 10.5% in the protective group (P < .001). In addition, the lung-protective strategy resulted in a 69% reduction in the number of subjects requiring ventilator support within the first 7 days after surgery. Severgnini et al36 compared the use of a traditional ventilation strategy (VT = 9 mL/kg PBW and no PEEP) with a lung-protective strategy (VT = 7 mL/kg PBW with PEEP = 10 cm H2O and recruitment maneuvers) in 56 subjects scheduled to undergo elective open abdominal surgery lasting >2 h and found that subjects in the lung-protective group had better pulmonary function tests up to day 5, fewer alterations in chest radiographs up to day 3, better oxygenation, and a lower clinical pulmonary infection score. Ladha et al37 performed a large (69,265 subjects) hospital-based registry study in 3 Massachusetts hospitals from January 2007 to August 2014. They compared subjects who received protective mechanical ventilation (VT <10 mL/kg PBW, PEEP ≥5 cm H2O, and plateau pressure <30 cm H2O) with subjects who received non-protective mechanical ventilation in terms of postoperative respiratory complications during non-cardiac surgery. They found that using protective mechanical ventilation intra-operatively was associated with a significantly lower risk of postoperative respiratory complications and that it was the VT (as opposed to PEEP and plateau pressure) that had the most beneficial effect difference. Fernandez-Perez et al38 performed a retrospective analysis of 170 subjects who underwent pneumonectomies. The results showed that 18% of the subjects developed respiratory failure and 50% developed ALI. These subjects had higher VT values than those who did not develop respiratory failure (8.3 vs 6.7 mL/kg PBW, P < .001).
There are a couple of recent meta-analyses that examined the effects low VT strategies during mechanical ventilation in surgery. Zhang et al39 performed a systematic review of 22 studies of subjects undergoing general anesthesia during major surgery and the development of ALI. They found that lower VT ventilation was associated with a protective effect against the development of ALI. Likewise, Gu et al40 performed a recent meta-analysis that included 19 randomized controlled trials in 1,348 subjects undergoing surgery and compared the subjects who received lung-protective ventilation (5–8 mL/kg PBW) with those who received traditional mechanical ventilation. There was a decreased incidence of lung injury and pulmonary infections in the lung-protective mechanical ventilation group (Fig. 2).33,35,40–46

Effect of lung protective ventilation with lower tidal volumes (VT) on lung injury and pulmonary infection. From Reference 40, with permission.
Cardiac surgery with cardiopulmonary bypass in and of itself is associated with a systemic and pulmonary inflammation.47 Cardiopulmonary bypass-related systemic inflammatory response syndrome represents an important first hit for lung injury, and the use of high VT values during the surgery may act as the second hit that worsens lung damage. Two studies looked at the effect of low VT strategy on pulmonary pro-inflammatory mediators in this patient population. Zupancich et al31 studied the effect of VT on interleukin 6 and 8 levels in the bronchoalveolar lavage fluid and plasma in 40 subjects undergoing elective coronary artery bypass. They found that, whereas the levels of interleukin 6 and 8 increased in both the low and high VT groups, they leveled off in the low VT group while they kept increasing in the high VT group (Fig. 3). Miranda et al48 also looked at the effect of VT on pro-inflammatory mediators in 62 subjects undergoing coronary artery bypass. Their results mirrored those of Zupancich in that there was an initial increase in levels of pro-inflammatory mediators in all subjects, but it became attenuated in the low VT group.28 In a large study Lellouche et al49 examined consecutively 3,434 subjects who underwent cardiopulmonary bypass and the immediate postoperative VT values. A multivariate analysis revealed that larger VT values were associated with longer time on mechanical ventilation and prolonged times in the ICU (Table 2) as well as hemodynamic instability.
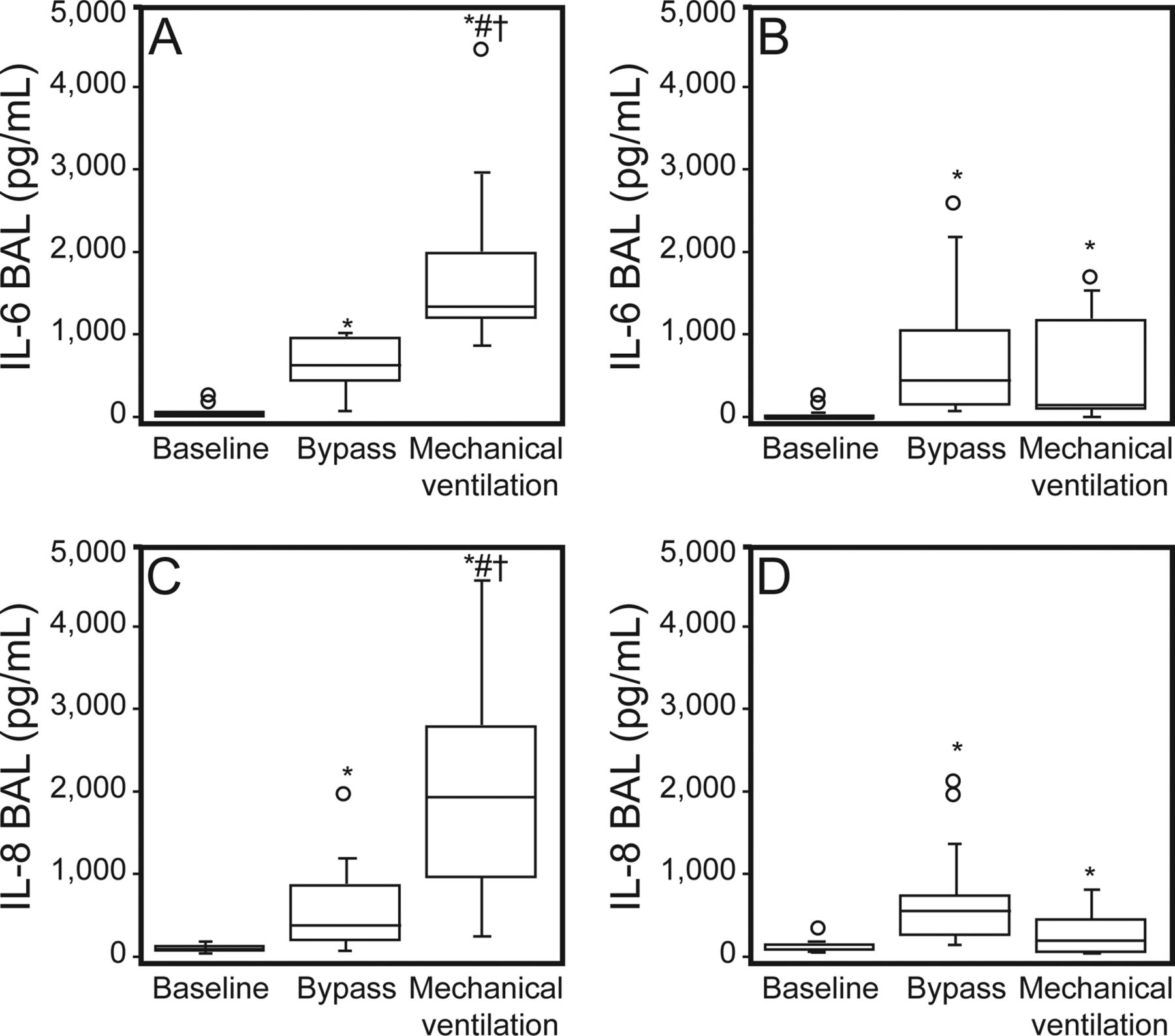
Effect of different ventilatory strategies (A and C: high VT/low PEEP; B and D: low VT/high PEEP) on plasma interleukin 6 and interleukin 8 before sternotomy (baseline), start of cardiopulmonary bypass (bypass), and 6 h after re-establishment of mechanical ventilation (mechanical ventilation). BAL = bronchoalveolar lavage. *, P < .001 versus baseline; #, P < .001 versus time bypass; †, P < .001, high VT/low PEEP versus low VT/high PEEP. Points denote outliers. From Reference 31, with permission.
Organ Failure, Duration of Mechanical Ventilation, and ICU Length of Stay
Other outcome measurements have been used in comparing high versus low VT during cardiac surgery. Sundar et al50 examined the time to extubation for cardiac surgical subjects receiving either 6 mL/kg or 10 mL/kg PBW. They found that, although the time to extubation did not significantly decrease, significantly more subjects in the lower VT group were extubated and breathing without assistance 6–8 h after surgery. They also noted that the lower VT group had a lower incidence of re-intubation.
Although the above studies make a convincing argument for the use of lower VT values in the operating room, well-powered randomized controlled trials are still needed to better establish the clinical effect of intra-operative lung-protective ventilation. However, until this occurs, physiologic data strongly suggest that the low VT strategy is safer and more protective than traditional VT values.
Concerns About Using Low VT
Indeed, there are concerns about using lower VT values during mechanical ventilation. Among them are the potential for hypercapnia, patient-ventilator asynchrony, and increased sedation use. Hypercapnia is a real possibility when clinicians use a low VT strategy. However, increases in set breathing frequency can offset this as long as auto-PEEP is not created. There are a number of studies that have actually shown beneficial effects of permissive hypercapnia in that it may have the potential to attenuate lung injury.51–54 Some have even suggested that hypercapneic acidosis could be therapeutic as opposed to permissive.55 However, the degree of permissive hypercapnia that can be used safely during low VT ventilation is unclear, but it may be that a mild acidosis should be tolerated to enable the use of lower VT values. Patient-ventilator asynchrony is also a potential issue with the use of lower VT values, especially in volume assist control with a fixed flow. The smaller VT values may result in shorter inspiratory times, which may create a mismatch with the patient's neural timing. However, with technological advances, today's mechanical ventilators now have advanced graphic packages that depict the waveforms in great detail. This equips the clinician to be better able to identity patient-ventilator asynchrony and act to minimize it through ventilator manipulation. Concerns have been raised that low VT ventilation may increase patient discomfort, leading to increased sedative use.56 However, there are a number of studies that refute this claim.22,57–59
Summary of the Pro Position
There is very strong evidence from randomized controlled trials that the use of a 6 mL/kg VT strategy affects mortality outcome in ARDS. The routine use of a low VT strategy in all patients receiving mechanical ventilation is not yet an “official” recommendation, but evidence is mounting that the use of low VT values in patients without ARDS may add additional protection against the injurious effects of mechanical ventilation, leading to a paradigm shift from treating ARDS to the prevention of ARDS. There is convincing evidence that the use of low VT values during intra-operative ventilation protects against postoperative pulmonary complications. The role of low VT strategy in other ventilated patients without ARDS is less certain, but the evidence so far is suggestive that these patients will also derive a protective benefit from VT reduction in terms of reduction of pulmonary complication rate and improvements in outcomes. Should 6 mL/kg be the “standard” VT to be used in all patients? The answer to this is yes, keeping in mind that there may be exceptions to this standard. Although the evidence to this point in time supports the use of 6 mL/kg PBW, it is unknown whether 4 mL/kg PBW is better than 6 mL/kg PBW. All we know is that 6 mL/kg PBW is more protective than 10–12 mL/kg PBW. However, in the absence of more elaborate measurements and with the evidence we have to this point, it makes sense to at least start ventilation with the target of 6 mL/kg PBW at the bedside. Given the unpredictability of developing ARDS during mechanical ventilation, a low VT ventilation strategy in all mechanically ventilated patients makes sense and should be used at the initiation of mechanical ventilation. The use of 6 mL/kg PBW at the onset of mechanical ventilation will help to ensure the early delivery of lung protection in patients at risk (whether it is known by the bedside clinician or not) of developing ARDS. The evidence also suggests that this practice is safe in the majority of mechanically ventilated patients.
Introduction of the Con Position
The premise that one prescription is good for all patients and conditions is, on its own, difficult to sustain. It is possible that one size fits most and that the ill effects of such a decision are so small in comparison with the benefits that it warrants blanket application. However, there are enough reasons (clinical and physiological) for why the general application of VT = 6 mL/kg PBW could lead to adverse events. Not only are there conditions (eg, COPD and acidosis) where using a standard “low” VT could be deleterious, but we must remember that the only reason to scale the VT to PBW is to prevent ventilator-induced lung injury (VILI). Reconsideration of a generic VT dosage of 6 mL/kg is of particular importance in light of recent literature suggesting that scaling the VT to PBW is, not a predictor of lung injury.60
Effect of a VT of 6 mL/kg PBW on Gas Exchange
There are several determinants of gas exchange, including the partial pressures of oxygen and carbon dioxide, lung perfusion, alveolar surface and thickness, hemoglobin levels, VT, breathing frequency, and dead space. To better understand the effect of VT, let's assume normal alveolar and blood gas partial pressures, lung perfusion, alveolar surface, and thickness. The effect of VT on gas exchange is then described by the equation for alveolar minute ventilation, V̇E = (VT − VD) × f, where V̇A is minute alveolar ventilation, VD is the dead space volume, and f is breathing frequency. It becomes evident that to keep a constant V̇E, in the presence of a constant VT and VD, the only variable that can change is breathing frequency. Now consider that we prescribe a VT of 6 mL/kg PBW for a patient in which all physiological values (alveolar surface, perfusion, and dead space = 2 mL/kg) are within normal limits.61 The alveolar minute ventilation range within the normal to highest limits of set ventilator breathing frequency will be as follows: V̇E = (VT − VD) × f; V̇E = (6 mL/kg − 2 mL/kg) × 10–35 breaths/min; V̇E = 40–140 mL/kg/min; V̇E for a 70-kg man = 2.8–9.8 L/min.62
Now, consider COPD or even acute lung injury where VD is elevated or sepsis and metabolic acidosis, where the metabolic demand requires a higher V̇E.63,64 If we increase the dead space, just by 1 mL/kg, the maximum minute ventilation that the ventilator can safely deliver decreases by 25%: V̇E = (6 mL/kg − 3 mL/kg) × 10–35 breaths/min; V̇E = 30–105 mL/kg/min; V̇E for a 70-kg man = 2.1–7.4 L/min. Using conventional ventilation, attempting to ventilate with small VT values will lead to higher breathing frequencies and development of hypoventilation, intrinsic PEEP, hemodynamic compromise, and higher work of breathing.62,65
Hypoventilation
As described above, the use of lower VT values frequently leads to some degree of hypercapnia (due to the restriction of breathing frequency to <∼35 breaths/min using conventional modes of ventilation). Clinicians have adopted the practice of permissive hypercapnia to avoid lung injury. This was accepted as a consequence because the effects of mild to moderate hypercapnia on various organ systems seem to be of no clinical relevance in the majority of critically ill patients.66–68 However, the clinician must remember the effect of carbon dioxide in different organs and systems, which are of much relevance in specific conditions. For example, the central nervous system is extremely sensitive to carbon dioxide levels. Hypercapnia leads to an increase in cerebral blood flow, which in the setting of intracranial hypertension may be deleterious. In specific settings, such as increased intracranial pressure or ischemia, a low VT strategy could be injurious for the brain.
Another clinically relevant example is the effect on the cardiovascular system. Acute hypercapnia leads to an increase in cardiac output secondary to an increase in cardiac contractility, increased heart rate, and a reduction in systemic vascular resistance. This leads to an increase in oxygen delivery, which is further enhanced by a deviation of the oxyhemoglobin dissociation curve. In contrast, the effect of hypercapnia on the pulmonary vasculature is different. Hypercapnia causes an increase in pulmonary vascular resistance and pulmonary artery pressures by enhancing the effects of hypoxic vasoconstriction.69,70 With this knowledge, patients with underlying pulmonary hypertension or right heart failure may not benefit or may even be harmed when exposed to hypercapneic conditions. In summary, the implementation of strategies that may lead to hypercapnia on all critically ill patients may have deleterious effects.
Time Constant and Auto-PEEP
The time constant (s) is obtained by multiplying compliance (mL/cm H2O) and resistance (mL/cm H2O/s). The time constant describes the time required to achieve a 63% change in pressure, volume, or flow in response to a step change in inspiratory pressure under passive conditions. Figure 4 demonstrates that the lung will inflate or deflate at the same proportion for a time interval (the time constant), and in consequence, it takes 5 constants to essentially empty or fill the lung. Table 3 demonstrates this concept. In a patient with ARDS, the compliance and resistance are low; thus, the time constant is short, and the lung inflates rapidly. However, in an emphysematous lung, the time constant is prolonged (both compliance and resistance are higher); thus, a longer time is needed to empty. In table 5 you can note that at 5 constants the lung has achieved full deflation or inflation. In ARDS this would take 2.7 s vs 5.5 s in COPD.
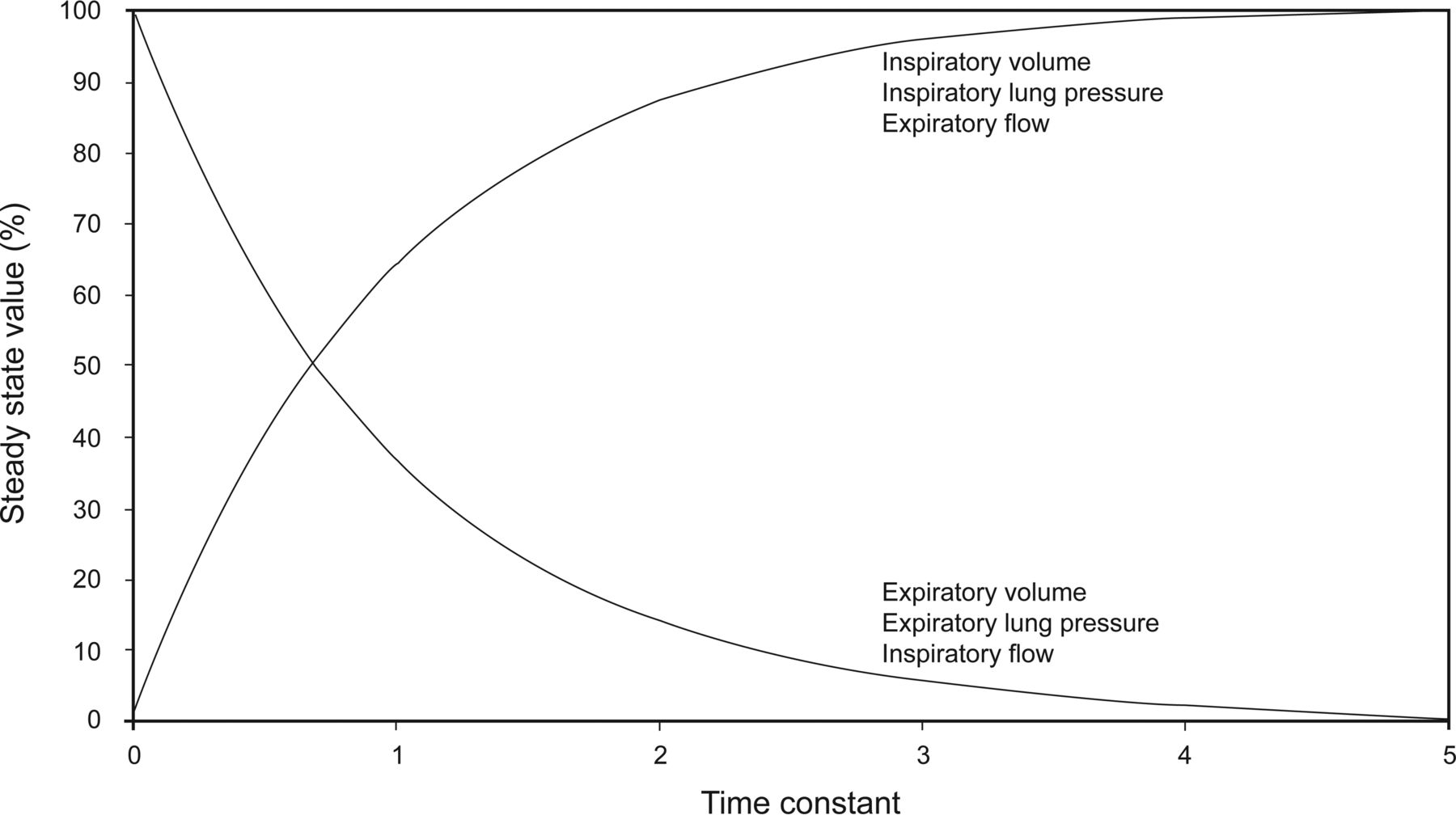
Time constant.
Time Constants for Common Clinical Conditions. The time (s) for normal lungs, ARDS, and COPD are given.
As the VT becomes smaller, all else being equal, the breathing frequency must increase to maintain the target minute alveolar ventilation. Patients with longer time constants who are exposed to higher breathing frequencies (mandatory or spontaneous) will develop air trapping. In fact, in obstructive disorders, the recognition and avoidance of auto-PEEP (the pressure associated with air trapping) leading to lung hyperinflation is the cornerstone in management. Tuxen et al72 described a strategy where decreasing the amount of hyperinflation by creating hypoventilation leads to improved outcomes. This trial emphasized the importance of the time constant and allowing adequate time for expiration. In that report, the initial VT values were 10 mL/kg actual body weight (ranging from 700 to 900 mL) and respiratory the breathing frequency was limited to avoid air trapping. Interestingly, since the advent of the ARDSNet trial, guidelines and reviews for mechanical ventilation in obstructive lung disorders have been gradually decreasing VT values, despite the absence of any new work in the management of COPD.73–75 We must not forget that air trapping and auto-PEEP leading to hemodynamic consequences occurs also in ARDS, where the time constant is considerably shorter.76,77
Work of Breathing
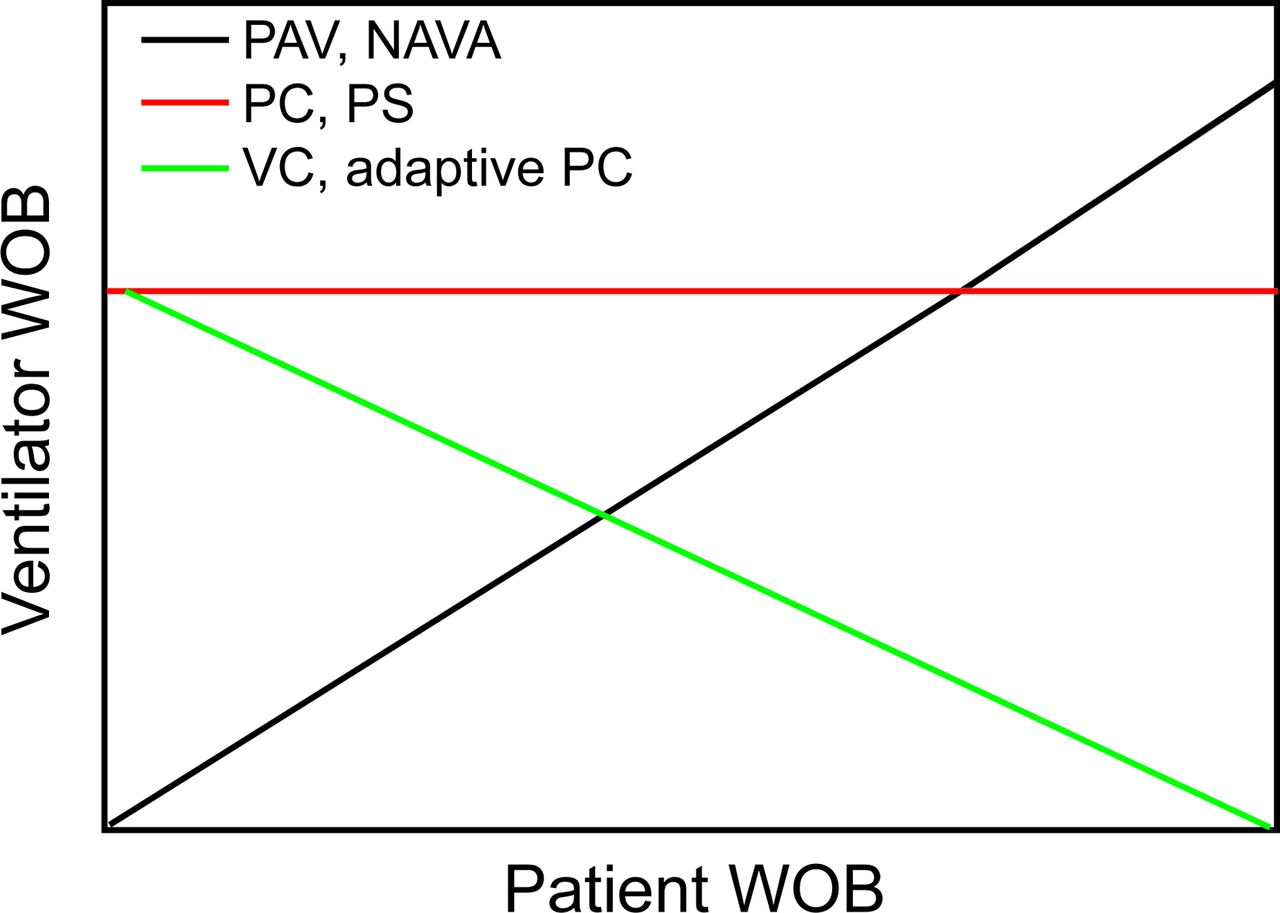
Figure 5 depicts the relationship between the ventilator and the patient work of breathing according to the mode of mechanical ventilation.78 This relationship is essential to understanding the effects of decreasing VT on the patient's work of breathing. The ventilator work of breathing will depend on the driving pressure required to achieve the desired target. When the target is volume, in the presence of patient effort, the ventilator will require less driving pressure to deliver a given VT. It follows that when lower VT values are set, the driving pressure will be lower, resulting in a shift of work toward the patient (ie, the ventilator will do less work to deliver the volume). In volume control ventilation, when the patient effort is high enough, the patient may actually breathe against the ventilator (which will not deliver more flow/volume) (see Fig. 6). In modes that use pressure control, in the presence of respiratory effort, the operator or the ventilator will need to decrease the inspiratory pressure to maintain the target VT.79
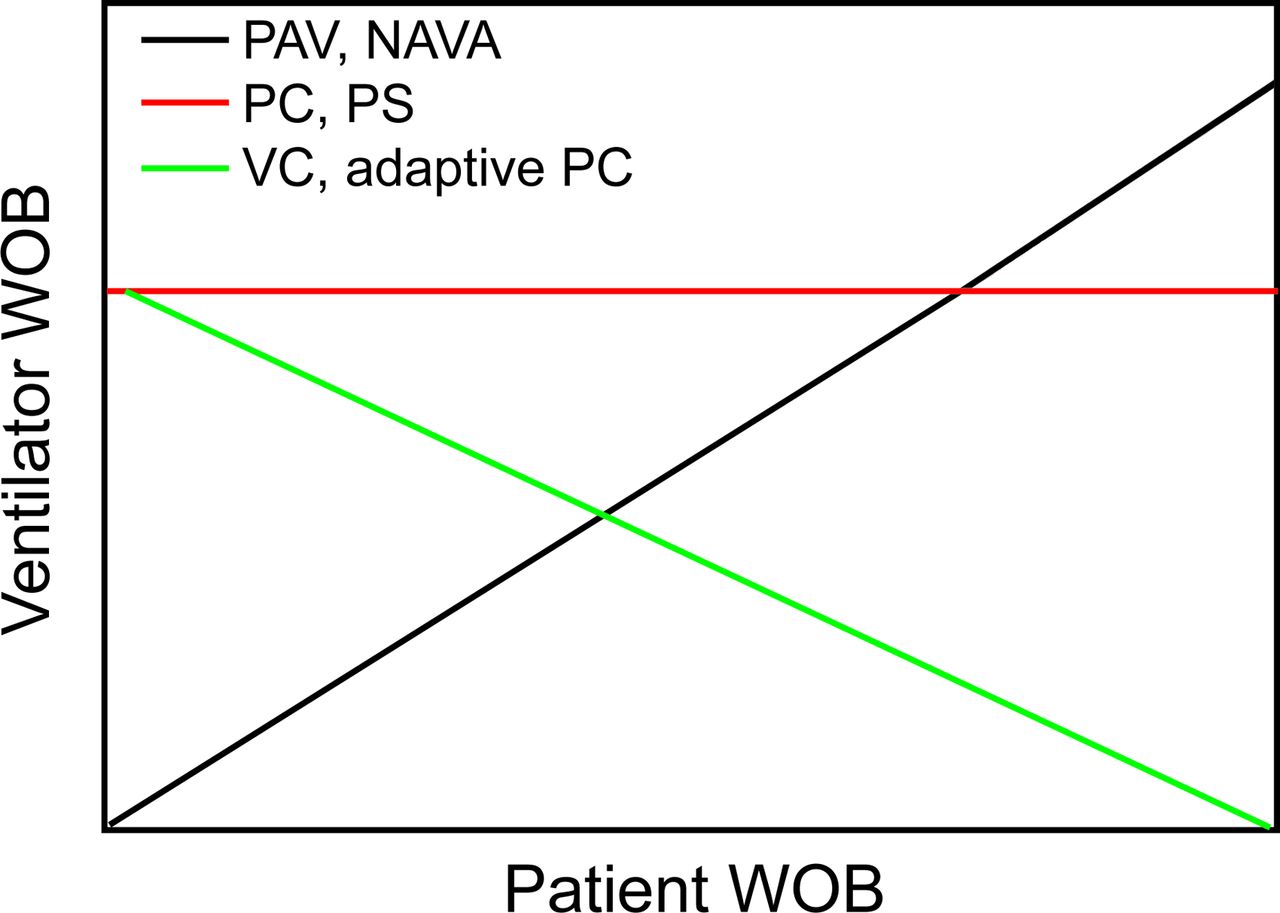
Patient versus ventilator work of breathing (WOB) in relation to the mode of mechanical ventilation; PAV = proportional assist ventilation; NAVA = neurally adjusted ventilatory assist; PC = pressure control; PS = pressure support; VC = volume control.

Simulated screenshot of flow starvation in volume control continuous mandatory ventilation. Shown is a graphical representation of a volume-controlled breath in the presence of a simulated patient respiratory effort. The green line represents airway pressure at the mouth opening. When the airway pressure drops below baseline (PEEP) a mismatch between patient's flow needs and the ventilator flow delivery is present. The drop in pressure below baseline is interpreted as no work of breathing support by the ventilator.
As we can see, decreasing the VT size may lead to unmatched patient work of breathing. This results in increased work of breathing and asynchrony. The resolution of this has due to low VT; with the use of higher VT in ARDS have been well described by Kallet et al.65 In clinical practice, the presence of asynchrony related to high respiratory drive (double triggering, flow asynchrony in volume control, or excessive VT values in pressure control) may lead to use of sedation or paralysis to allow limitation of the VT and synchrony. Indeed, the analysis of studies evaluating the ARDSNet studies revealed no increase in sedation and paralytics.57–59 However, in the context of a broad population, some with normal lungs, COPD, or severe acidosis, the utilization of sedation may be different. This poses a particular clinical challenge and may lead to prolongation of mechanical ventilation and the inherent adverse effects of oversedation and paralytics.80–82
VILI
In terms of VILI, an excessive VT is a well-recognized cause of alveolar overdistention (stretch injury), alveolar wall rupture (disruption), and cyclic recruitment.83 The ARDSNet trial was a culminating point in our understanding of VILI and led to a change in practice.12 After the trial was published, controversy ensued regarding what component (VT or plateau pressure) was the driver of the results. Trials by Stewart et al,11 Brochard et al,9 and Brower et al84 found no difference between low and high VT ventilation in subjects with ARDS. The trial by Amato et al10 and ARMA found a lower mortality in favor of lower VT. Eichacker et al85 pointed out that the 3 “non-beneficial” trials used VT closer to 10 mL/kg in the higher VT group, and the plateau pressures were <28–32 cm H2O, whereas in the 2 “beneficial trials,” the higher VT of 12 mL/kg was associated with high airway pressures (>34 cm H2O), and this would explain the mortality difference.9–12,84,85 Petrucci and Iacovelli86 reported similar findings and showed that clinical outcome of high VT ventilation was not different from that of low VT ventilation when plateau pressure was maintained at 31 cm H2O or less; however, the sample size between the groups was very different (lower plateau pressure 288 subjects vs higher plateau pressure 1,009 subjects), so the results should be interpreted with caution. Guidelines and protocols suggest limiting VT at 6 mL/kg PBW and plateau pressure <30 cm H2O to prevent VILI. However, more recent evidence reveals that neither VT scaled to PBW nor plateau pressure are adequate surrogates for predicting outcomes.87 How do we reconcile this with the available evidence?
Scaling
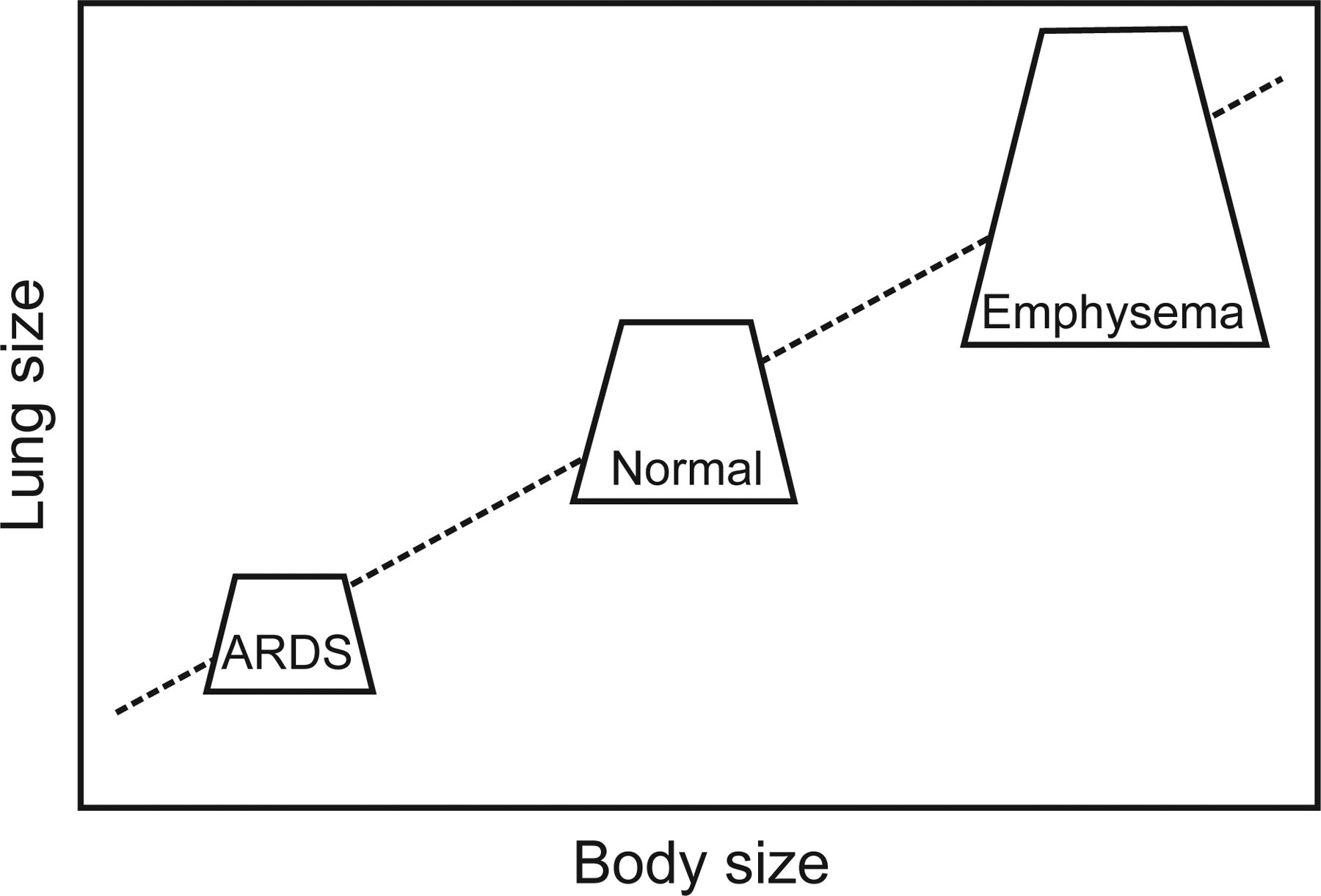
The current method to select VT dosage is to scale (normalize) it to the PBW (using height and sex), similar to the way drug dosages are calculated. This was an important contribution from the VT trials, which helped to standardize interventions across centers and made clear to everyone the VT used.12,84 The rationale to normalize the VT was that the lung size is defined by height rather than by weight (ie, an adult will have the same size lungs regardless of his weight). This concept makes sense in health, but the VT scaled to the height may not reflect the actual size of the lungs in disease. Gattinoni88 made the case that in patients with acute lung injury, the normally aerated tissue was closer to the size of a “baby lung.” On the opposite side of the spectrum are lungs that are larger than expected for the height due to a pathologic process. The classic example would be emphysema, in which the lungs are larger than expected for the height of the patient (ie, the aerated tissue is closer to the size of a giant's lung) (Fig. 7). Under these circumstances, scaling VT to PBW could lead to inappropriate settings. In the case of the ARDS lung, 6 mL/kg could be too large a VT, which would lead to injury. In the case of emphysema, a 6 mL/kg would be too small, leading to increased percentage of dead space ventilation, tachypnea, and auto-PEEP.
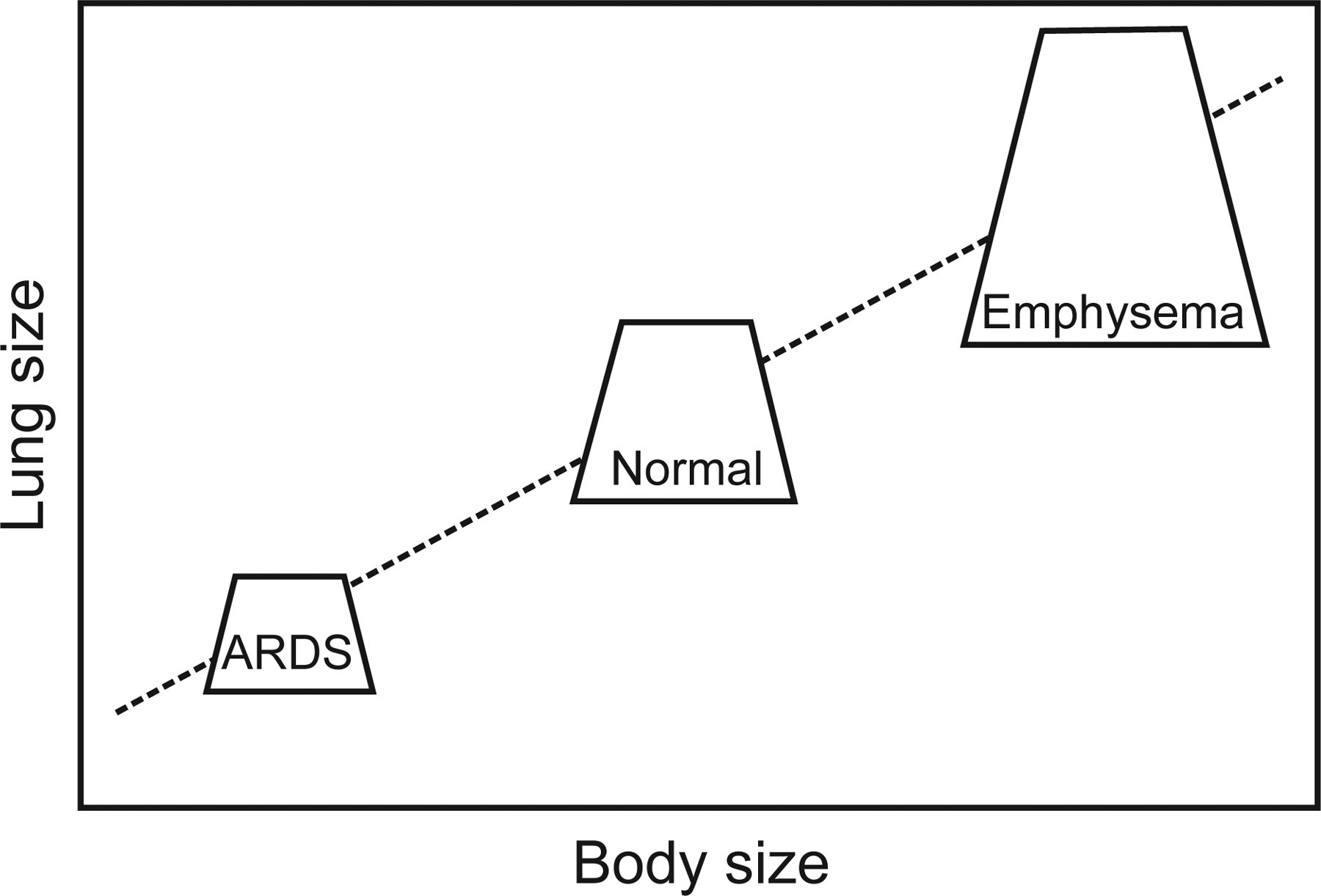
Relative size of the lung according to body size. In a patient with ARDS, the lung volume will shift down, such that for the same body size, the lungs will be smaller (as if they were from a smaller person). In a patient who develops emphysema, the lung volume shifts up, so that for the same body size, the lungs will be larger (as if they were from a larger person).
Several groups have come to recognize that the alternative is to scale the VT to the respiratory system characteristics (compliance or elastance) rather than PBW. A pioneer in this field, Mead et al89 described the concept of relative stress as the change in volume relative to resting size. They then elegantly studied the concept of regional stress multipliers as a source of lung injury. This concept demonstrated that under heterogeneous lung conditions, areas of alveolar collapse would generate multiplication of the wall stress in the neighboring areas. Using this rationale, current research groups have evaluated the effect of stress and strain on the lung, recognizing that scaling VT to the respiratory system characteristics may be a better predictor or marker of injurious mechanical ventilation.13,60,90 Gattinoni90 interpreted strain as the change in volume (change in size) over the functional residual capacity (resting size).
Lung injury can then be explained by excessive application of global or local stress and/or strain. Chiumello et al87 tested this theory in an animal model of ARDS. They found that strain values in the range of 1.5–2, which corresponds to a transpulmonary pressure (stress) of 10 cm H2O, were the critical threshold for injury. In this study, neither VT/PBW nor plateau pressure was a marker of lung injury. More importantly, prolonged application of very large VT (27 ± 3 mL/kg) without any PEEP for 2.5 d did not cause any lung injury as long as the strain was below the threshold.
A recent study by Amato et al60 used data from 9 randomized trials evaluating mechanical ventilation in ARDS to assess whether VT normalized to the respiratory system compliance was a better predictor of injury. They used the definition of compliance (the inverse of elastance), CRS = VT/Δ P, where CRS is the compliance of the respiratory system (which includes the lung and chest wall components), VT is the tidal volume delivered above PEEP, and ΔP is the difference between plateau pressure and set PEEP. ΔP or driving pressure was then defined as VT/CRS.
As such, ΔP is normalizing or scaling the VT to the respiratory system compliance. The advantage is that ΔP is an index of both high VT and low CRS, each of which is associated with VILI. In their thoughtful analysis, ΔP was the variable that best predicted survival. More to our point, neither VT/PBW nor plateau pressure had any predictive effect on survival or barotrauma. (eg, there was no difference in the relative risk of mortality at any level of VT/PBW from 4 to 10 mL/kg PBW).
Summary of the Con Position
In summary, limiting VT values to 6 mL/kg PBW for all patients receiving mechanical ventilation has the potential to cause harm. The blanket application could lead to increased breathing frequencies, auto-PEEP, hypoventilation, increased sedation, and unmatched work of breathing. All of these issues may be worth the price to prevent lung injury; however, new evidence on the understanding of lung injury suggests that the scaling of VT to PBW is not an accurate way of predicting risk in the first place. Thus, the concept of limiting VT to 6 mL/kg PBW needs to be reexamined in the face of the patient's condition, disease, and physiological characteristics. A simple VT dosage for all patients may not be appropriate and may lead to harm in specific cases. The risk of developing side effects is higher in patients with severe lung disease, increased respiratory drive (neurological or metabolic), increased dead space, and prolonged time constants (Tables 4 and 5).
Conditions Where Higher Tidal Volume May Be Beneficial
Conditions Where Lower Tidal Volume May Be Beneficial
Conclusions
The use of low VT strategies has been well validated in ARDS and has led to a paradigm shift in our thinking and ventilation management for these patients. We have learned that mechanical ventilation and the knobs we manipulate therein significantly affect our patients and can be injurious. This frame of mind has expanded to the realm of non-ARDS patients. There is emerging evidence that using lower VT values in surgical and non-ARDS mechanically ventilated patients may improve clinical outcomes and prevent the incidence of ARDS in high risk patients, which begs the question: Why not employ the use of VT of 6 mL/kg PBW for all patients, including those without ARDS? We must exercise some caution in taking this to the bedside. First, new evidence suggests that there may be a better way to adjust our VT values; however, more studies are needed before we should incorporate it into practice. We must keep in mind the physiology and the multiple conditions often found in the ICU, also keeping in mind that there may yet be situations where 6 mL/kg PBW may not be optimal. Also, the use of 6 mL/kg PBW does have the potential to induce hypercapnia, auto-PEEP, and patient-ventilator synchrony. However these conditions are manageable at the bedside in the majority of cases. There are a couple of reasons to strongly consider the use of 6 mL/kg PBW in all patients at the initiation of mechanical ventilation. The first is that pulmonary damage can happen in only a few hours after the initiation of mechanical ventilation with inappropriate settings. The second is that ARDS is frequently recognized after a delay in onset of the inflammatory process. Therefore, early use of 6 mL/kg PBW can be considered a preventive measure as opposed to a therapeutic modality. This may be especially protective in at-risk conditions, such as sepsis, trauma, transfusions, or high-risk surgeries. Considering the evidence to date, it does seem prudent to use 6 mL/kg at the initiation of mechanical ventilation. This has the potential to change, however, with emerging new evidence. At present, 2 large randomized control trials are being conducted. The first is a Dutch multi-center randomized control trial titled PReVENT-NL comparing a low VT strategy (4–6 mL/kg PBW) with conventional VT use (8–10 mL/kg PBW) in critically ill patients without ARDS with the end point being the number of ventilator-free days and mortality at day 28 (available at http://clinicaltrials.gov; NLM Identifier NCT02153294). The second is EPALI, being conducted in Spain. This study is comparing a low VT strategy of ≤6 mL/kg PBW with 8 mL/kg PBW in critically ill patients at risk for developing ARDS with the end point being the development of ARDS (available at http://clinicaltrials.gov; NLM Identifier NCT02070666).
Discussion
Kallet:
Great presentation by both of you. I think this is still an important topic with unresolved issues. When we look at VT of 6 mL/kg and compare it to other mammals, this obviously has to be done in a singular context—at rest. Otherwise, there's no way to compare anything. So how we breathe sitting here nodding off after lunch is different than what we do in activity. In evolutionary terms, your demand goes up, your minute ventilation goes up, and your VT goes up. I think irrespective of whether it's an activity like hunting or some athletic activity or you're massively septic, your VT is not going to stay at 6 mL/kg. In terms of the sedation/VT issue, it's an issue of proprioception. When you control VT and demand goes up, the work of breathing (WOB) goes up because during volume control, the ventilator fights the patient. Or you put them on pressure control or proportional assist ventilation (PAV) where the ventilator augments increased breathing efforts. It decreases the sense of dyspnea, but the damage goes up. And there's no good solution to this. The issues of sedation are the negative effects of that. When you look at studies that say there's no difference in sedation, I have a hard time believing that because the issue is: How are asynchrony and need for sedation being assessed? What are they using as criteria? During the ARDSNet trial, I saw data from a few centers where some subjects were breathing 60 breaths/min and that was tolerated, because sedation was not protocolized in that study, and that was the strategy chosen by the clinicians managing the patient (unpublished observations). I couldn't personally deal with that; I would ask physicians to increase the sedation to keep the subjects in sync. Asynchrony has some very negative effects. Yet, I don't think patients need to be perfectly synchronous with the ventilator. I think a modest or even moderate amount of asynchrony is allowable if the person doesn't seem to be suffering. Bob [Kacmarek] may offer another opinion on that, and I think he has some justification to do so. But in the context of patients who are extremely ill and we have trouble ventilating, oxygenating, and are hemodynamically unstable, we have to take them out of the picture. If someone has a little bit of schmutz here or there on their chest x-ray, their P/F ratio is a little funky, I don't think there's any way I could justify keeping them deeply sedated to keep them in sync versus liberalizing their VT. Generally around 8 mL/kg with a good flow, you'd have pretty decent luck with that. Obviously it's a hard nut to crack and the nice thing about the study by Amato1 is it's reassuring to know that maybe it's the stress-strain, so we don't need to be as worried. Patients who have relatively minor injury with only a modestly decreased functional residual capacity (FRC) can tolerate that volume without increasing lung injury.
Kacmarek:
I think we scale VT already; I mean the range is 4-8 mL/kg. If you look at Marcelo Amato's data,1 the majority of patients who we ventilate, if we appropriately set PEEP and use a reasonable VT in that range, it is very unusual for your driving pressure to be significantly beyond 15. Where you get into trouble, particularly with ARDS patients, is when you have not appropriately recruited the patient and not appropriately set PEEP. The way I interpret driving pressure is it's added to the 2 other factors. He makes a point in the paper saying it's only driving pressure; I don't buy that. All the data that have been accumulated that he analyzed, some of those subjects had huge VT values. They were from previous studies using 12-15 mL/kg VT values. I think it is the driving pressure, plateau pressure (Pplat), and VT that all have to be considered, and I don't think we can leave any of those 3 out of the equation. Most patients if you've gone from pressure-targeted ventilation or volume-targeted ventilation to PAV or neurally adjusted ventilatory assist (NAVA) they tend to choose small VT values; they don't choose large VT values. Critically ill patients don't like big VT values; they breathe rapidly and shallowly unless they have a neurologic or pharmacologic reason why they should breathe deeply. They just don't, not on a regular basis.
Kallet:
I would say patients who are very acidotic don't. Or mechanically they can, but the drive from the brain might be different. Patients who are extremely acidotic do not target 8 mL/kg; their brain is telling them to be hyperpneic, whether they can achieve that mechanically or not. That's the only caveat I would add.
Kacmarek:
OK.
Marini:
Many good things came out in the talk, but I just want to emphasize a couple of them. What Rich mentioned is extremely important; in focusing on the events within the tidal cycle, we tend to forget about minute ventilation. A guy who has a minute ventilation of 14 L/min should not be equated with somebody with a minute ventilation of 5 or 6 L/min. Cumulative stretch forces are going to be much greater at the higher minute ventilation, and so will be the tendency for lung damage. The fascinating thing is we've been using the same equation in different ways for 40 y in trying to limit ventilator injury. What is driving pressure? Driving pressure is the quotient of VT and compliance. We've targeted best PEEP to compliance in the past—that's what Peter Suter did.2 Now we're twisting these same 3 factors (VT, compliance, and pressure) and saying, “OK, driving pressure is the real deal,” which I'm very happy to see because I think it refocuses appropriately upon the tensions that are really the damaging forces associated with VT. Indirectly, Deans and Natenson3 said in response to the original ARMA4 trial, “Look, there are going to be some people who are incorrectly treated with 6 mL/kg and others who will be fine with 12 mL/kg. It depends on the pressures and tensions developed by the VT.” These are really not new concepts, but I'm glad to see the refocusing. Whenever we talk about driving pressure, we're talking about a passive individual, and we should be looking at the trans-lung pressure. The lung itself is non-homogenous, and even a small number of damaged units can set in motion escalating problems. Understandably, we're trying to simplify things. A 6-mL/kg VT is a good starting point, but it's got to be assessed and adjusted to compliance and ventilation needs. I think driving pressure is useful—provided you know what you're looking at. Finally, I don't think lung injury due to ventilator management directly causes death; at the very least it's not the only contributing factor. If driving pressure and mortality are linked, you wonder, “Is this causal?” Is it really true that you either get driving pressure right or you get it wrong, and the patient lives or dies? It is a part of the issue, but it can't be the whole thing.
Kacmarek:
It's a manifestation of the severity of illness.
Branson:
I wanted to ask the question I get asked most often in SICU (surgical ICU): My patient comes out and is on 10-cm H2O PEEP, has a P/F ratio of 250, and is on nothing but pressure support, and the pressure support is 8 cm H2O, so the Ppeak is 18 cm H2O, and the VT is 12 mL/kg. Do I have to be concerned, or is that OK?
Kacmarek:
According to Amato,1 you don't have to be concerned.
Hess:
It depends. Getting back to what John [Marini] just said, if there is a pleural pressure change of −20 cm H2O on every breath, I would be concerned.
Mireles-Cabodevila:
The underlying condition too. The health of the lung. If the milieu is correct and you have injury to the lung, you will be more prone to injury. That's what we're seeing from the papers in the OR.
Kacmarek:
Amato's discussion of driving pressure is totally focused on controlled mechanical ventilation.1 It does not apply to patient-triggered ventilation because of what we're saying—we have no idea what the respiratory muscles are generating and what the true transpulmonary pressure (Ptp) and driving pressure is.
Branson:
So are we advocating for doing esophageal manometry on everybody?
Kacmarek:
No. But 12 mL/kg, a patient doing that voluntarily, I'd have to say what's going on? What is driving that patient to do that? Because you just don't see it. You might get to 8 or 10 mL/kg, but to sustain >12 mL/kg is not a normal response that you see with a pressure support of 8 cm H2O. Even in surgical patients, we don't see that on a regular basis.
Kallet:
I think the context is important. If this is a patient you're planning on keeping intubated for a short period of time, I wouldn't do anything. If this is someone coming back to the ICU from massive abdominal surgery with several risk factors for ARDS and will be intubated for several days, I think it's prudent to do something there. But again, it depends on the context.
Branson:
So, do what?
Kallet:
Extubate.
MacIntyre:
I think one thing you have to remember is that in the Amato paper,1 most of those data (I'll grant ARMA4 as an exception) came from the PEEP studies, where VT values were all kept in the 4-8 mL/kg range. The independent variable was adjustments of the PEEP and using different PEEP strategies. These were not random assignments of PEEP and VT values that occurred. You thus have to interpret these data a little more carefully. But the notion behind it I kind of like—thinking regional rather than global VT. Six mL/kg (IBW [ideal body weight]) in you and me gets distributed evenly because all of our alveoli are normal. But take out half my lung and put 6 mL/kg into me now, and lo and behold you're going to blow up the remaining normal lung. The idea of referencing VT to either CRS, as Amato1 does, or FRC or functional TLC like Gattinoni5 does make all kinds of sense. I'm not sure why we're considering this such a breakthrough. This notion of regional VT values and regional overinflation has been around for a long time. Lung-protective ventilation really isn't protecting the sick lung but the healthy lung. In all lung disease, there are regions that are reasonably healthy, and that's why I like the idea of smaller VT values for everybody, because that's what we're trying to do—protect healthier regions. I think using FRC or functional TLC as measures or CRS as surrogates to estimate what's going on regionally just makes sense to me. I'm not sure it's such a revolutionary idea. I'm more like John, I think it's nice to see an old idea being refocused upon.
Holets:
So one question then, and this may be beyond the scope of this discussion. If a patient is at risk for developing lung injury, where does noninvasive ventilation (NIV) come into this?
MacIntyre:
Or do you mean high-flow oxygen (>40 L/min).
Holets:
Yes, NIV and high flow devices.
Marini:
I review a lot of papers, and I've seen stuff that I cannot easily put a mechanism to. For example, in anesthetized patients without lung disease, it has been recently observed that in surgeries lasting 2-4 h, if the VT exceeds a certain volume, there will likely be postoperative complications attributable to the high VT. If that were true, then every person with normal lungs who goes out exercising should come back with ARDS. During exercise we generate—there was a paper in Chest6 in the late ‘90s that looked at this—esophageal pressures averaging about 40 cm H2O at peak treadmill exercise. Some healthy subjects went up to 60 cm H2O or more. You're talking here about a driving pressure across the lung that's 3 times what's supposed to be damaging for the lung and chest wall in ARDS. It's very critical (and Rich alluded to this) the substrate that you're dealing with. I can't understand the surgical operating theater as a venue in which to emphasize practicing tight lung protection for patients who have normal lungs.
Hurford:
John, but remember that those are very abnormal conditions in the OR. Classically, FRC is reduced by 50% very quickly; there's a lot of atelectasis that occurs within 10 min of inducing anesthesia. You have increases in intra-abdominal pressure, you have release of inflammatory mediators. It's a very short time and I share your suspicion, but I don't want people to walk away thinking that the lung of a supine person with a lot of surgeons inside their belly is a normal situation. Similar to pulmonary resection, if you're taking out one lung and that remaining lung is already diseased and you're having the release of inflammatory mediators, it's a more abnormal situation than you might believe. Admittedly, if you're having a knee arthroscopy, it's going to be really hard to screw up. We've ventilated people with 10-15 mL/kg for years and years, and those folks weren't ending up in the ICU. Our pneumonectomy patients were. And the mortality rate was dramatically reduced when we changed ventilator strategies.
Marini:
Bill, those are excellent points. Let's not forget the vascular side too. When you're dealing with a small lung like a single lung resection, you're pouring a lot of blood flow through that single lung and you're really upping the ante. You're absolutely right; in certain surgery patients, you have to be particularly careful. Do you measure the pressures in the anesthesia machines?
Hurford:
Yes.
Marini:
And keep them down?
Hurford:
We do. It's hard. There's a recent study that looked at our use of lower VT values in the OR, and there was a recent study7 from Vanderbilt looking at some academic institutions, Mayo Clinic, Partners, nearly 300,000 cases. And even in high-risk subjects, they were using >8 mL/kg about 40% of the time. It's one of these things to have very slow adoption. Everyone's confused. Normal patients probably don't need it, patients at high risk probably do; we really don't know who's at risk, so is there harm in using it on everybody? I don't know.
Footnotes
- Correspondence: John D Davies MA RRT FAARC, Respiratory Care Services, Duke University, Box 3911, Durham, NC, 27710. E-mail: john.davies{at}duke.edu. Eduardo Mireles-Cabodevila MD, Respiratory Institute, Cleveland Clinic, 9500 Euclid Avenue, A90, Cleveland, OH 44195. E-mail: mirelee{at}ccf.org.
Mr Davies and Dr Mireles-Cabodevila presented a version of this paper at the 54th Respiratory Care Journal Conference, “Respiratory Care Controversies III,” held June 5–6, 2015, in St Petersburg, Florida.
Mr Davies has disclosed a relationship with ResMed. Drs Senussi and Mireles-Cabodevila have no conflicts to disclose.
- Copyright © 2016 by Daedalus Enterprises
References
- 1.↵
- 2.↵
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.
- 27.↵
- 28.↵
- 29.↵
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.
- 42.
- 43.
- 44.
- 45.
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.
- 68.↵
- 69.↵
- 70.↵
- 71.
- 72.↵
- 73.↵
- 74.
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- Early Studies
- Ventilation of Patients Who Do Not Have ARDS
- Ventilation of Surgical Patients
- Concerns About Using Low VT
- Summary of the Pro Position
- Introduction of the Con Position
- Effect of a VT of 6 mL/kg PBW on Gas Exchange
- Hypoventilation
- Time Constant and Auto-PEEP
- Work of Breathing
- VILI
- Scaling
- Summary of the Con Position
- Conclusions
- Discussion
- Footnotes
- References
- References
- Figures & Data
- Info & Metrics
- References