

Abstract
The aim of this systematic review is to examine the benefit/risk ratio of the use of mechanical insufflation-exsufflation (MI-E) devices for airway clearance in patients with neuromuscular diseases. A search was conducted for relevant studies in MEDLINE, the Cochrane Library, and the Health Technology Assessment Database using the main key words: cough, airway clearance, in-exsufflation. The search limits were studies published in English and French between 1970 and 2014 (literature watch until December 2015). The methodological quality of the studies was assessed using (1) the Cochrane Collaboration's risk of bias tool for randomized controlled trials and (2) the Institute of Health Economics' 20-item checklist for comparative and observational studies. Data were extracted into an evidence table according to (1) study design, (2) population characteristics (including age and type of diseases) and intervention (MI-E associated or not with other interventions), (3) outcome measures, and (4) key findings. Twelve studies met the inclusion criteria (4 randomized controlled trials, 3 comparative studies, and 5 observational studies). The quality of the selected studies was poor. None of the studies reported survival outcome. All studies evaluated change of pulmonary function parameters, such as peak expiratory flow. This review underlines the lack of robust data on mechanical medical devices used for airway clearance. The current scientific evidence does not support the use of MI-E for cough augmentation in patients with neuromuscular diseases, but health-care professionals are faced with the reality of medical practice and the absence of alternatives. Most European and American guidelines recommend the use of MI-E despite low-level evidence. However, even if performing comparative trials in a specific population is difficult, the medical device industry should provide reliable data to assist health-care professionals, providers, and payers in the decision-making process. This is the only way to ensure the best treatment for patients.
Introduction
Over 90% of respiratory failure episodes in patients with neuromuscular disease are caused by ineffective coughing during concurrent chest colds.1 In these patients, the unstretched chest wall muscles become shorter and stiffer due to the disease process.2–5 When peak expiratory flow (PEF) falls below 160 L/min, it indicates an ineffective cough, and airway clearance becomes inefficient.6 The combination of loss of respiratory muscle strength, ineffective cough, and decreased ventilation leads to a high risk of developing pneumonia, atelectasis, and respiratory insufficiency and failure.7,8 It represents the primary cause of mortality and morbidity in patients with neuromuscular diseases.9 The deterioration of respiratory muscle function in these diseases, besides affecting lung function, also affects functional capacity, limits activities of daily living, and reduces quality of life.10
When intercostal and abdominal muscles are too weak to generate sufficient thoracoabdominal pressures,4,11,12 cough assistance may be achieved by manual and/or mechanical methods. Both methods provide inspiratory and/or expiratory assistance to improve cough efficiency.13 However, these methods must be adapted to each patient, because advanced neuromuscular diseases make patients unable to stand or mobilize.14,15 Manual methods include postural drainage, active cycle of breathing technique, or chest physical therapy, but respiratory muscle weakness limits a patient's ability to perform breathing exercises. Mechanical methods include high-frequency chest wall compression, intrapulmonary percussive ventilation, positive expiratory pressure, and mechanical insufflation-exsufflation (MI-E).16 These nonpharmacologic airway clearance techniques, excluding MI-E, have been studied by Andrews et al17 in hospitalized subjects. Based on this systematic review, the American Association for Respiratory Care recommended that cough assist techniques should be used in patients with neuromuscular diseases, particularly when PEF is <270 L/min, because their PEF can fall below 160 L/min during respiratory infection. However, the American Association for Respiratory Care cannot recommend chest physiotherapy, positive expiratory pressure, intrapulmonary percussive ventilation, and high-frequency chest wall compression in these patients due to insufficient evidence.18
As many physiotherapy treatments available become impractical in patients with advanced neuromuscular disease, MI-E could represent an alternative.19,20 MI-E devices deliver a positive pressure to the airway (insufflation) and then rapidly shift to negative pressure (exsufflation).21 They can be used with an oronasal interface or with an endotracheal or tracheostomy tube. The objective of MI-E devices is to evacuate bronchopulmonary secretion deposits.22,23 This technique was developed in the 1950s.24 It has been used in the United States since the 1990s. The availability of MI-E devices in Europe since 2002 has increased the number of studies initiated.25,26 The first team that performed a systematic review on MI-E was Anderson et al27 in 2005. Their systematic review included 4 controlled trials, with a total of 98 subjects with neuromuscular disease. They concluded that evidence to support the use of MI-E for airway secretion management in patients with neuromuscular diseases was evolving.
In this context, we decided to perform a systematic review to update the available evidence. The aim of this systematic review is to assess the benefit/risk ratio of the use of MI-E devices for airway clearance in patients with neuromuscular disease. Considering that observational studies might be of interest to collect safety data, we decided to include them in addition to randomized controlled trials and comparative trials and evaluated the literature available since 1970.
Methods
Search Strategy
We searched for relevant studies in 3 bibliographic databases (MEDLINE, the Cochrane Library, and the Health Technology Assessment Database), covering a period from 1970 to October 2014 and combining the main key words: cough OR airway clearance OR in-exsufflation OR randomized controlled trials OR observational studies using the Boolean operator AND. Our full search strategy can be found in the supplementary material at http://www.rcjournal.com. Additional manual searches were conducted on professional societies' websites. We checked the reference lists of selected studies to retrieve any missing articles. A literature watch was performed until December 2015 on the websites listed in the supplementary material and in the MEDLINE database.
Selection Criteria
According to the PICO process, we defined the population, the intervention (or exposure in the case of observational studies), the appropriate control or comparator, and the outcomes of interest.28 Describing the inclusion criteria ensures reproducibility and transparency and guides the determination of study eligibility, data extraction, analysis, and interpretation of results. To be included in this review, studies were identified based on the following PICO criteria: P, subjects with neuromuscular diseases; I, MI-E devices (in-patient and out-patient); C, comparison with manual techniques (in case of comparative trial); O, efficacy and/or safety (mortality, hospitalization rate/length of hospital stay, respiratory exacerbations [pneumonia, tracheotomy, etc], pulmonary function parameters [cough peak flow (CPF), SpO2, PtcO2, etc], and adverse events of MI-E devices). Subject quality of life (comfort, distress, and fatigue parameters assessed with a visual analog scale or level of convenience based on subject or caregiver statements) was also taken into consideration.
Study Selection
We selected randomized, controlled trials and comparative and observational studies. Studies were excluded when they included subjects with cystic fibrosis or if they were only available in abstracts for communication or meetings. Papers without an abstract or written in languages other than English or French were also excluded. In the case of dual publications from the same study, the most recent publication was selected. Two reviewers (VH and CA) independently screened titles and abstracts for possible inclusion in the review. Any discrepancies were resolved by discussion. When one reviewer concluded that the article could be eligible for the review based on the abstract, we retained it for full-text assessment. One reviewer assessed the full text of each included study and extracted data into the evidence table. The second reviewer double-checked the data.
Quality Assessment of Individual Studies
To avoid biases, each selected study was analyzed, and its quality was assessed by 2 independent reviewers using reading grids. For randomized, controlled trials, a grid adapted from the Cochrane Collaboration's risk of bias tool was used (adequacy of the randomization, baseline comparability, blinding, withdrawals, and intent-to-treat analysis).29 It includes an assessment for each entry in a risk-of-bias table, where each entry addresses a specific feature of the study. The judgment for each entry involves rating the risk of bias as low risk, high risk, or unclear risk. For comparative and observational studies, a grid adapted from the Institute of Health Economics' 20-item checklist was used (eligibility criteria, sources and methods of selection of participants, outcomes clearly defined, and description of follow-up methods).30 A modified Delphi process was used to develop this checklist. It resulted in a 20-criterion checklist for assessing the internal validity of comparative and observational studies. A study with a score of >14 is considered to have an acceptable methodological level.
Data Collection
Data were extracted into an evidence table according to (1) study design, (2) population characteristics (including age and type of diseases) and intervention (MI-E associated or not with other interventions), (3) outcome measures, and (4) key findings. We performed a narrative synthesis of evidence.
Results
Study Selection
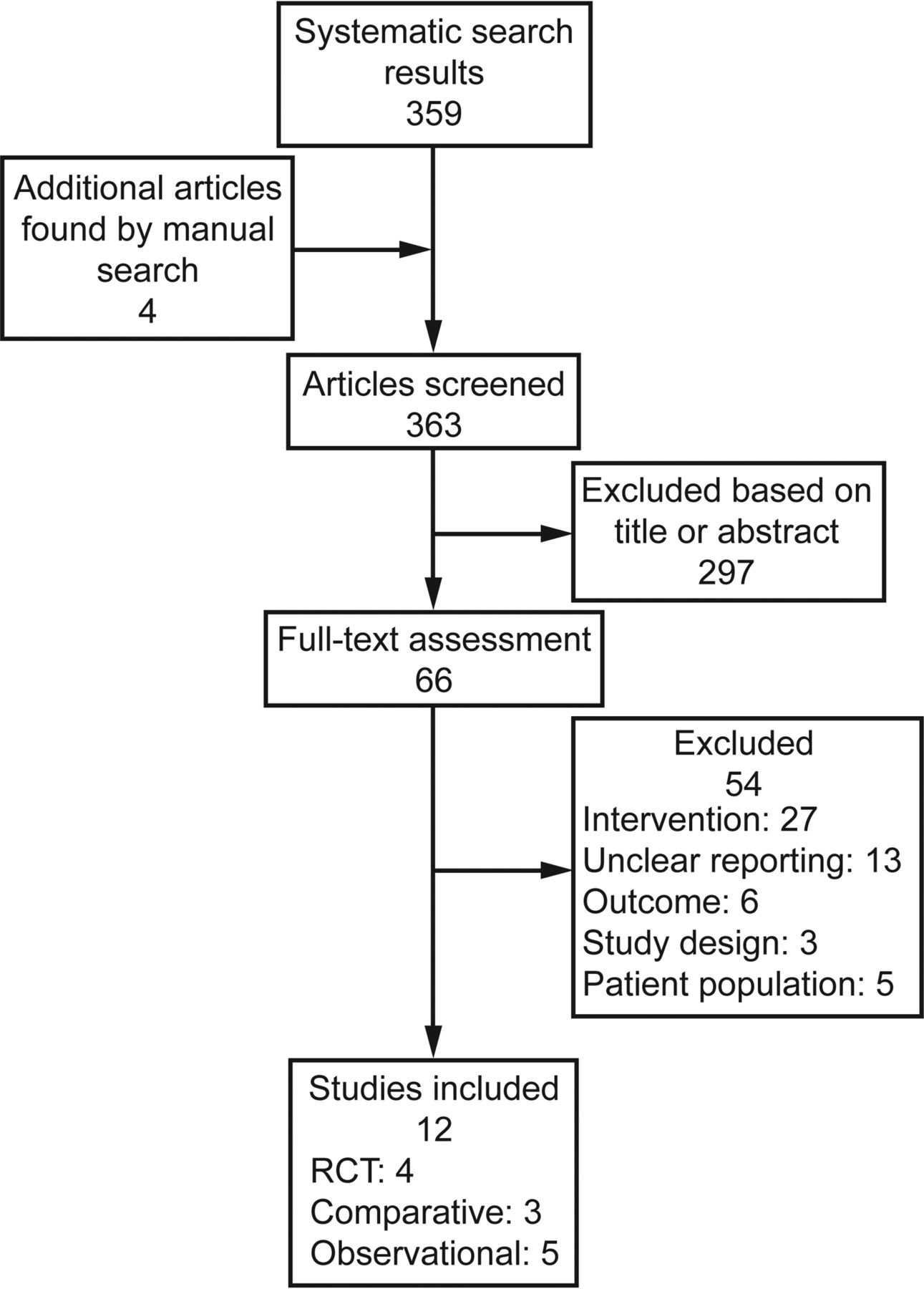
We reviewed 363 abstracts and 66 full-text papers. Of the 66 full-text papers assessed, 12 met the inclusion criteria (Fig. 1). The 12 studies that met the inclusion criteria were 4 randomized controlled trials,31–34 3 comparative studies,35–37 and 5 observational studies.38–42 The excluded studies are listed in the supplementary materials at http://www.rcjournal.com.

Flow chart. RCT = randomized controlled trial. Note that one of the comparative studies was a historical comparison.
Quality Assessment
The quality of the 4 selected randomized controlled trials was poor (Table 1). No details regarding the method of randomization and allocation concealment were available in the 4 studies. All studies were unblinded. Considering the nature of the treatment, blinding of subjects and clinicians was difficult, but it could have been discussed in the methodology. The selected observational and comparative studies had multiple biases, and their methodological quality was poor (Table 2). There was no comparison group or power calculation. Most of them were case series. The number of subjects was small, which decreases the power of statistical analysis. Some conclusions based on subgroup analysis should be considered with caution. The internal validity was rated between 13 and 15 for 4 studies35–37,41 and between 10 and 12 for 3 studies,39,40,42 and one study had a score of 9.38 Although most studies had scores <14, we decided to include them in our analysis to examine safety data, notably pneumothorax events.
Quality of Randomized Controlled Trials Included, Using the Cochrane Tool
Quality of Observational and Comparative Studies Included, Using the Institute of Health Economics 20-Item Checklist
Study Characteristics
The characteristics of the studies are described in Table 3. The studies had different designs and included retrospective series,39,42 observational cohorts with no control group,38,41 comparative studies,35–37,40 and randomized controlled trials.31–34 The studies ranged from 8 to 62 subjects and included altogether around 325 subjects. The sample size for out-patient studies ranged from 10 to 62 subjects (mean = 30), whereas it ranged from 8 to 57 subjects (mean = 26) for in-patient studies. Five studies of 12 included adults,31,34,36–38 3 included children,39,41,42 and 3 included both adults and children33,35,40 (unknown for one study).32 Twelve studies included subjects with neuromuscular diseases. Among them, 2 studies included mixed populations31,36 (subjects with neuromuscular disease or COPD).
Overview of Included Studies
Synthesis of the Results
The following sections summarize the results of the selected studies categorized by outcomes: survival, hospitalization rate, respiratory exacerbation, pulmonary function parameters, adverse events, and quality of life. Key information from the studies is detailed in supplemental Table 1 (see online supplementary material).
Survival Outcome.
None of the 12 studies included survival outcome.
Hospitalization Rate or Length of Hospital Stay Outcomes.
These outcomes were evaluated in a total of 21 subjects with neuromuscular diseases. The retrospective study of Moran et al42 investigated the impact of home MI-E on hospital admissions and lifestyle. Ten children with neuromuscular diseases were included. In these subjects, home MI-E reduced the number of hospitalization days (mean difference at 6 months = 29.7 d [95% CI 2.8–56.6 d], P = .04 and mean difference at 12 months = 30.4 d [95% CI 4.7–56.2 d], P = .03). Results showed no reduction in hospitalization rate. The authors highlighted that home MI-E use by children with neuromuscular disease can reduce the length of hospital stays and benefit families by keeping their child at home. Vianello et al40 prospectively studied 11 adults with neuromuscular disease during episodes of upper respiratory tract infection. A comparison was performed with a historical group of 16 subjects who had received chest physical treatments alone. Length of hospital stay was evaluated as a secondary end point. No difference was observed between the 2 groups studied (20.5 ± 20 d vs 19.8 ± 17 d, P = .93).
Respiratory Exacerbation Outcome.
In a retrospective medical record review, Miske et al39 studied the safety, tolerance, and effectiveness of MI-E. This case series included 62 subjects with neuromuscular diseases (4 months to 29 y old). A decreased frequency of pneumonia was observed in 5 subjects, and an improvement in chronic atelectasis was observed in 4 subjects. Vianello et al40 found that treatment failure (defined as the need for cricothyroid minitracheostomy and endotracheal intubation despite treatment) was lower in the MI-E group than in the conventional chest physical treatment group (2 of 11 vs 10 of 16, P = .047).
Pulmonary Function Parameter Outcome.
All trials evaluated change of pulmonary function parameters, such as CPF. In a prospective cohort, Bach et al38 compared CPF during 3 interventions (unassisted cough, manually assisted cough, and mechanical insufflation-exsufflation sessions) in 21 ventilator users (each subject was his/her own control). These subjects used noninvasive ventilator support methods for a mean of 22.3 h/d. They relied on MI-E during periods of productive airway secretions. No difference was observed in mean CPF values before and after MI-E (mean value: 104.4 ± 54 L/min before vs 109.2 ± 52.2 L/min after mechanical in-exsufflation, P = .09). The CPFs during MI-E exceeded those produced by manually assisted cough, which exceeded those during coughing following insufflation alone, which significantly surpassed unassisted CPF (108.6 ± 61.8 L/min [unassisted] vs 202.2 ± 64.2 L/min [air-stacking] versus 256.2 ± 77.4 L/min [manually assisted] versus 448.2 ± 61.2 L/min [MI-E], P < .001). The authors concluded that MI-E was an effective and safe method for facilitating airway secretion clearance in subjects with neuromuscular diseases.
The prospective study of Sivasothy et al31 evaluated the efficacy of manually assisted cough, mechanical insufflation alone, and both combined. The studied population comprised healthy subjects (n = 9), subjects with respiratory muscle weakness with or without scoliosis (n = 12), and subjects with COPD (n = 8). In this study, treatment allocation was randomized for each subject. In subjects with neuromuscular diseases without scoliosis, CPF increased significantly compared with the baseline value (104 L/min, 43–188 L/min), with manually assisted cough (185 L/min, 93–355 L/min, P < .01), and with a combination of manual and mechanical in-exsufflation techniques (248 L/min, 110–343 L/min, P < .01). In these subjects, CPF did not increase significantly with MI-E alone. Similar results were observed in subjects with COPD. Subjects with neuromuscular diseases associated with scoliosis reported no improvement with the studied interventions.
Mustfa et al32 conducted a prospective trial to investigate the effect of manually assisted cough (maximal unaided cough or manually assisted cough performed by an experienced respiratory physiotherapist applying pressure to the abdomen) and MI-E techniques (exsufflations delivered by the MI-E device, insufflations delivered by the MI-E device, or in-exsufflation coordinated with the subject's cough effort). These 5 techniques were performed in a random order. A total of 10 healthy volunteers, 21 bulbar and 26 non-bulbar amyotrophic lateral sclerosis subjects were included. Manual assistance increased CPF by 11% in bulbar (P < .01) and by 13% in non-bulbar subjects (P < .001). The exsufflations delivered by the MI-E device and manually initiated just before coughing increased CPF by 17% in healthy subjects (591 ± 135 L/min) (P < .05), 26% (P < .001) in bulbar subjects (225 ± 46 L/min), and 28% in non-bulbar subjects (279 ± 87 L/min) (P < .001).
Chatwin et al35 conducted a prospective trial. Their hypothesis was that MI-E would produce a greater increase in CPF than 4 other cough augmentation techniques (unassisted cough, physiotherapy-assisted cough, noninvasive ventilator-assisted cough, exsufflation-assisted cough) in subjects with neuromuscular weakness. This study included 22 subjects (8 children and 14 adults) and 19 age-matched controls (historical group). Results indicated that the greatest increase in CPF from baseline was observed with MI-E at 297 L/min (95% CI 246–350 L/min, P < .001). In the historical control group, an increase in CPF from baseline (unassisted cough, 578 L/min [95% CI 508–648 L/min]) with exsufflation-assisted cough (633 L/min [95% CI 570–695 L/min], P < .001) and in-exsufflation-assisted cough (629 L/min [95% CI 565–603 L/min], P < .001) was observed. Analysis of variance for the interventions revealed significant differences in both groups. Chatwin et al33 also conducted a randomized controlled trial in respiratory physiotherapy practice with or without the addition of MI-E. The studied pulmonary function parameters included SpO2, PtcO2, and heart rate. The study was conducted in 8 subjects with neuromuscular disease. Subjects were randomized into 2 groups. Subjects in group 1 received on day 1 a morning treatment without MI-E and an afternoon treatment with MI-E and received on day 2 a morning treatment with MI-E and an afternoon treatment without MI-E. Subjects in group 2 received the same treatment in the reverse order. In this study, no difference in measured pulmonary function variables was observed between the 2 interventions (without MI-E and with MI-E).
In a prospective clinical trial, Winck et al36 studied different pressures of MI-E in a clinically stable mixed population of subjects (13 subjects with amyotrophic lateral sclerosis, 7 subjects with other neuromuscular diseases, and 9 subjects with severe COPD). The objective was to evaluate the tolerance and effect of MI-E in these subjects. Subgroup analysis showed improvement in CPF after MI-E, with pressures set at 40 cm H2O for insufflation and −40 cm H2O for exsufflation. Although CPF significantly improved, the mean value did not exceed the 270 L/min threshold. In a prospective cohort, Fauroux et al41 investigated the pulmonary function parameters to analyze the physiologic effects and tolerance of MI-E. They included 17 children with neuromuscular diseases (5–18 y old). They observed an improvement in CPF after MI-E (162 ± 97 L/min at baseline vs 192 ± 99 L/min after MI-E 40 cm H2O, P = .02).
Senent et al37 designed a prospective study to compare CPF produced by a range of manual (unassisted cough and coached unassisted cough) and mechanical techniques (coaching with abdominal thrust, abdominal thrust associated with air-stacking, abdominal thrust associated with subject's bi-level pressure ventilator, abdominal thrust associated with patient ventilator or MI-E). Of the 28 included subjects with amyotrophic lateral sclerosis, 16 subjects were analyzed. All of the investigated instrumental techniques were statistically better than the manual techniques. A subgroup analysis of subjects with bulbar disease versus non-bulbar disease indicated no statistically significant difference in all coughing techniques (manual or mechanical) in both subject groups. Lacombe et al34 conducted a randomized, open, single-center, crossover study. They aimed to compare the effects of MI-E alone, MI-E associated with manually assisted cough, and intermittent positive-pressure breathing associated with manually assisted cough. Eighteen subjects with neuromuscular diseases requiring cough assistance were included. Results indicated a higher CPF with intermittent positive-pressure breathing associated with manually assisted cough than with MI-E associated with manually assisted cough or MI-E alone. According to the authors, adding MI-E to manually assisted cough may be deleterious or inefficient in subjects with neuromuscular disease, who can generate high CPF values with combined intermittent positive-pressure breathing and manually assisted cough.
Safety Outcomes.
Stomach distention episodes were reported in 2 studies (Bach38 and Vianello et al40). In the first one, the rate was not detailed. The adverse event disappeared after insufflation volumes and pressures were reduced to optimal levels. In the second study, one subject of the 11 included reported stomach distention but did not discontinue therapy. In the study by Miske et al,39 2 subjects complained about chronic abdominal pain and chest discomfort and decided to discontinue the treatment. One subject with acute respiratory failure experienced premature ventricular contractions on the initial use of MI-E and continued the treatment without difficulty after resolution of his acute respiratory failure episode. MI-E sessions were reported as well-tolerated in 3 studies (Chatwin et al,35 Winck et al,36 and Fauroux et al41). No subject complained about abdominal distention or vomiting, blood-streaked sputum, gastroesophageal reflux, chest pain, or discomfort, and no pulmonary hemorrhage was reported. Adverse events were not detailed or reported in 5 studies (Sivasothy et al,31 Mustfa et al,32 Chatwin et al,35 Senent et al,37 and Moran et al42).
Subject Quality of Life Outcome.
Fatigue was evaluated with a visual analog scale in one study (Chatwin et al33). The acceptability of each treatment was measured on a visual analog scale. The visual analog scale was evaluated 1–2 min before treatment and 1–2 min after treatment. Scores for fatigue following treatment in the “with MI-E” group were higher (3.2 ± 2.2 before vs 5.1 ± 2.6 after, P < .001), indicating a higher sensation of fatigue after MI-E sessions. Subject distress and comfort were also rated on a visual analog scale in their previous study.35 There was no change from baseline in results for comfort or distress of intervention on the visual analog scale. In the study by Moran et al,42 9 subjects reported that MI-E enhanced or improved their child's quality of life. A positive lifestyle effect expressed was the ability to keep their child at home during respiratory exacerbations. It should be noted that these were declarative data. Miske et al39 reported in their study that 3 subjects chose not to continue MI-E therapy. Subjects reported that the device was ineffective or unpleasant.
Discussion
This is the first systematic review including observational studies and the first literature update available on MI-E devices used for airway clearance in patients with neuromuscular disease since the work of Anderson et al27 in 2005. Our review underlines the lack of robust data on MI-E use for airway clearance in neuromuscular disease. Available evidence focuses on pulmonary function parameters, most often the PEF value. Even if PEF is widely considered to predict cough efficiency, it is not a validated surrogate end point. These pulmonary function parameters do not enable the impact of these techniques on patient morbidity, mortality, or quality of life to be proven. Most studies displayed short-term results. The few studies with long-term results reported some tolerance data but were of poor statistical quality due to retrospective designs or small numbers of subjects. It is also unclear whether adverse effects were systematically investigated. This observed variability limited the interpretation of the evidence in the literature and did not provide strong enough evidence. In fact, the concurrent review of Morrow et al43 performed during the same period also failed to reach a conclusion on the potential benefit of MI-E in patients with neuromuscular disease. Available clinical data did not enable them to conduct a meta-analysis.
The weakness of the available evidence contrasts with health-care practices. Health professionals assume that MI-E devices are effective for airway clearance in patients with neuromuscular diseases. The use of these devices in clinical practice despite poor clinical evidence may be related to the lack of available alternatives for these patients or to the possibility of using these noninvasive methods at home for out-patients.44 This is also illustrated by American and European guidelines.18 The American Association for Respiratory Care clinical practice guidelines, published in 2013, cautiously recommend MI-E for children with weak cough. The American Association for Respiratory Care clinical practice guidelines recommend, based on low-level evidence, cough assist techniques in patients with neuromuscular diseases when PEF is <270 L/min. For the European Federation of Neurological Associations,45 MI-E has been shown to be effective in patients with amyotrophic lateral sclerosis in uncontrolled trials. Even if there was a lack of robust evidence, the consensus determined a “Good Clinical Practice Point,” which concluded that the use of MI-E devices may be helpful, particularly in the setting of an acute respiratory infection. In 2011, the Canadian Thoracic Society46 recommended MI-E for patients unable to achieve PEFs >270 L/min with lung volume recruitment and/or manually assisted cough techniques, particularly during respiratory infections and in the absence of contraindications. These recommendations were supported by low-level evidence. In 2009, the British Thoracic Society recommended12 considering MI-E as a treatment option in patients with bulbar muscle involvement who are unable to do breath air-stacking or for any patient who remains unable to increase PEF to effective levels with other strategies. They also recommended combining MI-E with manually assisted cough where cough effectiveness remains inadequate with MI-E alone. These recommendations were supported by low-level evidence. For the American Academy of Neurology,47 MI-E may be considered to help clear secretions (Level C, possibly effective) in patients with lateral amyotrophic sclerosis. The American Thoracic Society48 strongly supports the use of MI-E in patients with Duchenne muscular dystrophy and also recommends further studies. The European Respiratory Society and the European Society of Intensive Care Medicine49 recommend that manually assisted cough techniques and/or MI-E should be applied in the management of non-intubated patients with retained secretions secondary to respiratory muscle weakness.
The results of our systematic review should be considered in light of the following limitations: All studies had different methodological designs and were not of a high quality level. However, we decided to look at observational studies to collect safety data. Subsequently, it would have been interesting to conduct a meta-analysis of the systematic review. A meta-analysis was not possible given the disparity of interventions and primary end points and the different follow-up durations in the included studies. We also cannot rule out a publication bias or selective reporting within the included studies.
Our review resulted in recommendations to help decision making regarding the reimbursement of devices by the French National Health Insurance Fund and to guide changes in care organization. It also encourages further research, in line with current international guidelines. The British Thoracic Society12 recommended a randomized controlled trial of MI-E compared with other methods of assisted cough used at home in children with neuromuscular diseases, to prevent acute respiratory deterioration; the European Neuromuscular Centre22 specifically highlighted the need for ongoing clinical research to test assumptions regarding management principles in neuromuscular diseases and to define a standard set of health-care goals, in particular for airway clearance.
Health professionals have also stressed the difficulty in conducting prospective studies to evaluate the efficacy of these medical devices in the long term. Designing a randomized study with a treated group versus an untreated group is also difficult to consider due to ethical considerations. The variety of the concerned pathologies, each covered by a specific primary end point, makes it difficult to construct such a study. Even if a survival end point is difficult to implement, end points such as the number of hospitalizations for bronchial congestion episodes or the assessment of patient quality of life could, for instance, be considered. Thus, even if comparative trials in a specific population50 are difficult to conduct, the medical devices industry should provide reliable data to assist health-care professionals, providers, and payers in the decision-making process.
Conclusions
Our work has raised the issue of the validity of the use of MI-E devices for cough augmentation in patients with neuromuscular diseases. The current scientific evidence is too weak to encourage their use, but health-care professionals are faced with the reality of medical practice and the absence of alternatives.
Further research is necessary to ensure the best treatment for patients with neuromuscular diseases.
Acknowledgment
We gratefully acknowledge Sophie Despeyroux, information scientist at the French National Authority for Health, who helped with research and document management, and Emmanuelle Fouteau, project manager at the French National Authority for Health, for valuable in-depth proofreading.
Footnotes
- Correspondence: Catherine Auger MSc, Medical Device Department, French National Authority for Health, 5 avenue du Stade de France, Saint-Denis La Plaine 93218, France. E-mail: c.auger{at}has-sante.fr.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}