

Abstract
BACKGROUND: After pediatric cardiac surgery, ventilation with high airway pressures can be detrimental to right ventricular function and pulmonary blood flow. Neurally adjusted ventilatory assist (NAVA) improves patient–ventilator interactions, helping maintain spontaneous ventilation. This study reports our experience with the use of NAVA in children after a cardiac surgery. We hypothesize that using NAVA in this population is feasible and allows for lower ventilation pressures.
METHODS: We retrospectively studied all children ventilated with NAVA (invasively or noninvasively) after undergoing cardiac surgery between January 2013 and May 2015 in our pediatric intensive care unit. The number and duration of NAVA episodes were described. For the first period of invasive NAVA in each subject, detailed clinical and ventilator data in the 4 h before and after the start of NAVA were extracted.
RESULTS: 33 postoperative courses were included in 28 subjects with a median age of 3 [interquartile range (IQR) 1–12] months. NAVA was used invasively in 27 courses for a total duration of 87 (IQR 15–334) h per course. Peak inspiratory pressures and mean airway pressures decreased significantly after the start of NAVA (mean differences of 5.8 cm H2O (95% CI 4.1–7.5) and 2.0 cm H2O (95% CI 1.2–2.8), respectively, P < .001 for both). There was no significant difference in vital signs or blood gas values. NAVA was used noninvasively in 14 subjects, over 79 (IQR 25–137) h.
CONCLUSIONS: NAVA could be used in pediatric subjects after cardiac surgery. The significant decrease in airway pressures observed after transition to NAVA could have a beneficial impact in this specific population, which should be investigated in future interventional studies.
- respiratory support
- noninvasive ventilation
- mechanical ventilation
- patient-ventilator interaction
- cardio-respiratory interaction
- patient-ventilator asynchrony
- pediatric
- cardiac surgery
Introduction
Assisted ventilation is essential to the care of children after cardiac surgery, sometimes for prolonged periods of time. Although positive-pressure ventilation can reduce the work of breathing and decrease afterload of the left ventricle, intrathoracic pressures can also reduce venous return and increase the afterload of the right ventricle.1–3 In the management of patients at risk for right ventricle failure or with a passive pulmonary blood flow, minimizing the ventilatory pressure is therefore crucial. In addition, support that is excessive or asynchronous can exacerbate the known complications of mechanical ventilation.4–6 Neurally adjusted ventilatory assist (NAVA) is a ventilation mode that provides ventilatory support that is synchronous and proportional to the electrical activity of the diaphragm (EAdi), allowing variation in tidal volume and inspiratory time between breaths.7 Many studies have shown that NAVA improves patient–ventilator interactions in children thereby permitting more spontaneous ventilation.8–14 The use of NAVA after pediatric cardiac surgery has been rarely reported in the literature,15,16 but it is regularly used in our pediatric intensive care unit (PICU) because of its theoretical advantages in this specific population.
In this article, we describe and analyze this experience. The main objective is to assess the feasibility of invasive NAVA in children admitted to PICU after heart surgery and its impact on ventilation pressures. The secondary objectives are to evaluate its effect on clinical and paraclinical parameters and to describe the use of noninvasive NAVA after extubation in this population. We hypothesize that using NAVA in this population is feasible and allows for lower ventilation pressures.
QUICK LOOK
Current knowledge
High positive airway pressure can be detrimental after pediatric cardiac surgery. Neurally adjusted ventilatory assist (NAVA) improves patient–ventilator interactions and facilitates the maintenance of the patient's own ventilation.
What this paper contributes to our knowledge
NAVA was feasible and well tolerated in our experience after pediatric cardiac surgery. The transition to NAVA was followed by a marked decrease in ventilation pressures, while adequate ventilation support was maintained.
Methods
Study Design
This retrospective study was conducted in the PICU of CHU Sainte-Justine Hospital, in Montreal, Quebec, from January 8, 2013, to May 31, 2015. Local ethics board approval was obtained with a waiver of consent (#4175).
Population
All subjects under 18 y of age who were admitted to the PICU following heart surgery and who were ventilated using NAVA (invasively or not) at least once during their PICU stay were included. Eligible patients were identified by automatically extracting all NAVA settings from the PICU electronic medical record system. When a subject underwent multiple cardiac surgeries during the same hospitalization, each postoperative course was considered independently. For each postoperative course, the duration of the different ventilation periods in each mode was noted.
During the study period, a limited number of ventilators in the PICU had NAVA capability (2 machines until June 2013, then 4 machines). Use of NAVA and the choice of settings were at the discretion of the medical team, depending on ventilator availability. Although no written protocol for the choice of ventilation mode was used in the PICU during this period, a written protocol was available to guide the management of NAVA. This protocol suggested to first estimate the level of EAdi that would be expected under NAVA, based on the EAdi observed before the switch, the change that was expected or desired (eg, if the patient seemed to be over-assisted with low EAdi, an increase in EAdi would be expected), and the consideration that normal EAdi in critically ill children is usually between 5 and 20 μV.17 Subsequently, the initial NAVA level was calculated as the ratio between expected driving pressure (usually the one observed in conventional ventilation) divided by the expected EAdi. Most importantly, the NAVA level was reassessed after the transition to NAVA and adjusted based on the observed EAdi, the subject's respiratory efforts and breathing frequency, the tidal volume (usual target, 5–8 mL/kg), and minute ventilation. The weaning procedure was at the discretion of the treating team and was not protocolized.
Data Collection
Data were collected retrospectively through a review of the electronic charts. Baseline data points included demographics, history of chronic pulmonary disease, duration of cardiopulmonary bypass, duration of aortic cross-clamping, and length of PICU stay. The type of cardiac surgery was recorded, in particular regarding the risk of right ventricular failure or low pulmonary flow (eg, Glenn, Fontan, Blalock–Taussig shunt, or other surgery), which was assessed by 2 investigators (GE and BT). The number, timing, and duration of all NAVA episodes were documented. The first period of invasive NAVA in each postoperative course was looked at in more detail; during the 4-h periods preceding and following the transition to NAVA, ventilation settings and measured values [peak inspiratory pressure (PIP), mean airway pressure (̄Paw), tidal volume], vital signs (average breathing frequency, average heart rate, average mean arterial blood pressure, SpO2), and available arterial or capillary blood gas data (pH, PaCO2, PaO2, lactates) were recorded.
Outcome Measures
The primary outcome measure was the hourly evolution of PIP and ̄Paw surrounding the start of NAVA. Secondarily, the change in clinical status after the transition to NAVA (pre-post comparison) was studied. As an indirect correlate for the feasibility of NAVA in clinical practice, NAVA episodes that were rapidly terminated (after < 2 h) were accounted for.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics 23 (IBM). Categorical variables are reported with absolute numbers and percentages. For continuous variables, we tested the normality of their distribution using the Shapiro-Wilk test. Continuous variables are reported using means ± SD or medians with interquartile range (IQR, ie, 25th–75th percentile), depending on the distribution. With regard to the primary outcome (hourly PIP and ̄Paw), a one-way repeated measures analysis of variance test was performed to determine whether there was a significant difference between the 8 time points, with post hoc complex contrasts allowing for comparison between the different time points. A P value <.05 was considered significant. Other secondary clinical values were compared with paired sample t tests when the variables were normally distributed, and with Wilcoxon signed rank tests otherwise.
Results
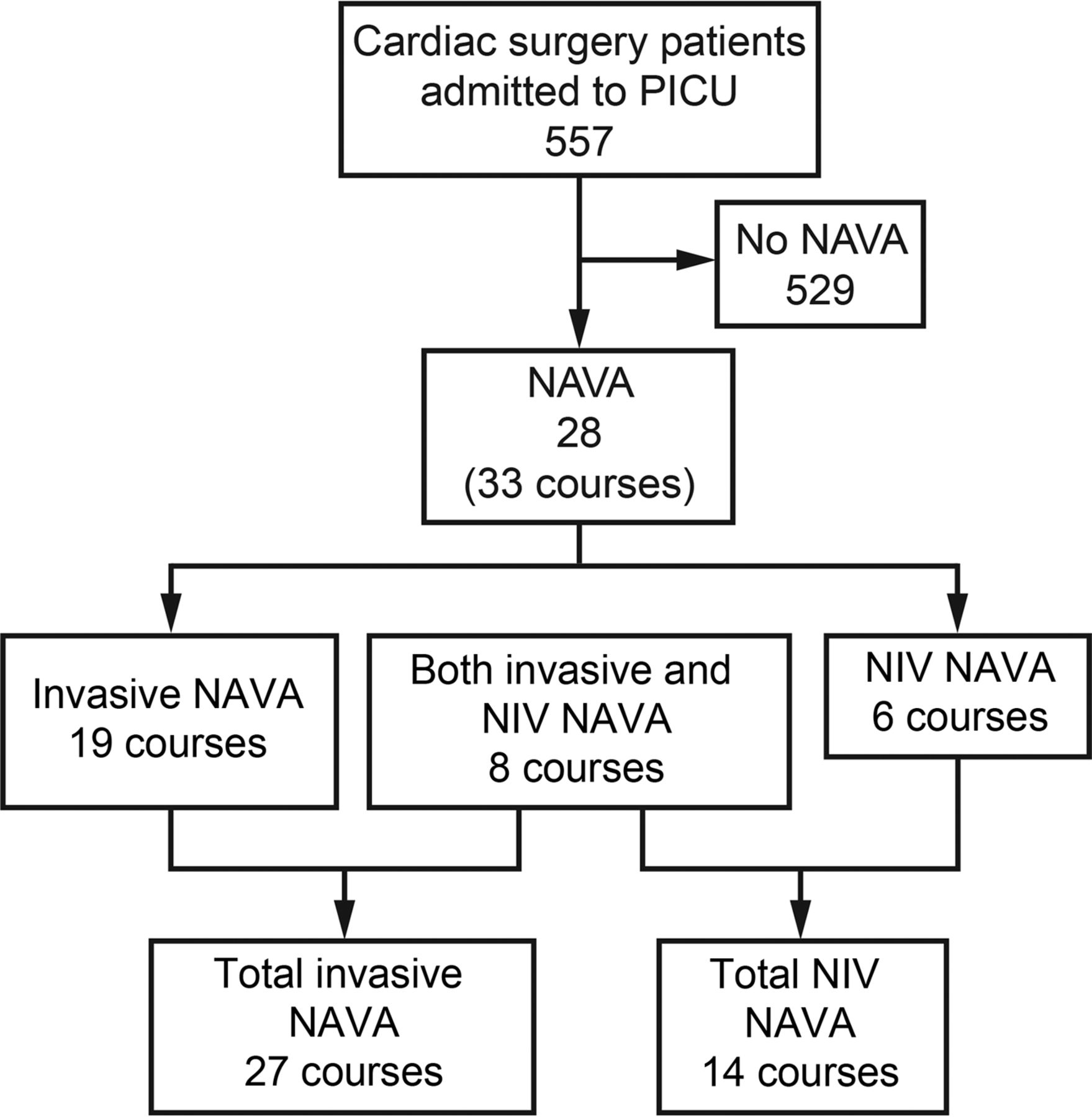
During the study period, 557 patients underwent cardiac surgery in our center. Twenty-eight subjects were ventilated using NAVA over 33 postoperative courses (Fig. 1) and were included in the analysis. Of these, NAVA was used during invasive ventilation only in 19 courses, during noninvasive ventilation only in 6 courses, and during both invasive and noninvasive ventilation in 8 courses.
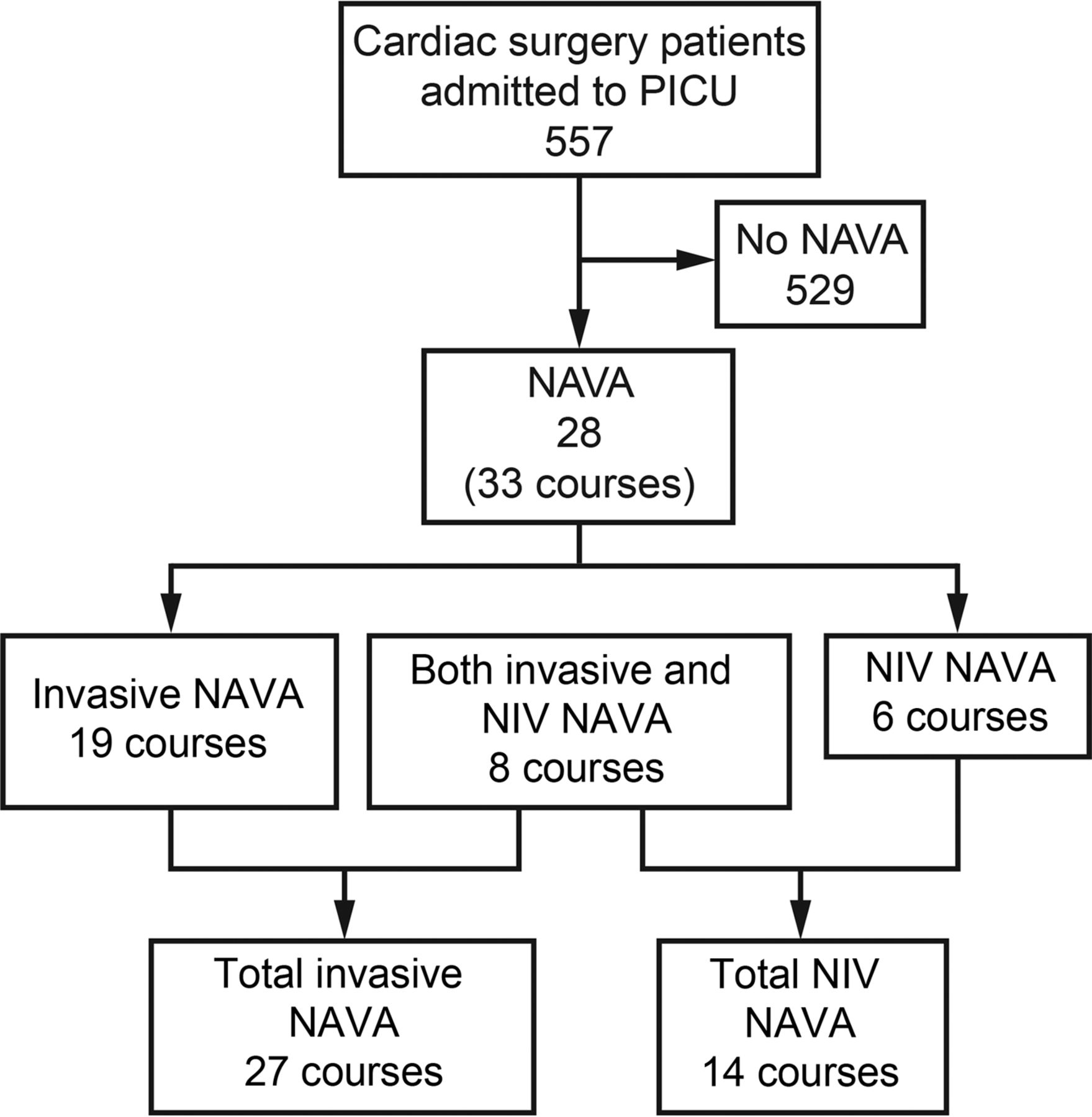
Flow chart. PICU = pediatric intensive care unit, NAVA = neurally adjusted ventilatory assist, NIV = noninvasive ventilation.
Characteristics of NAVA Episodes
As described in Table 1, subjects had a median age of 3 (IQR 1–12) months and stayed in intensive care for a median duration of 38 (IQR 23–76) d. Forty-three percent of the courses followed surgery considered at high risk for right-sided heart failure or low pulmonary flow. Various characteristics of the NAVA episodes are described in Table 2. The subjects underwent a median number of 2 (IQR 1–2) episodes of invasive NAVA within their postoperative course, with the first episode starting 8.3 (IQR 2.6–13.7) d after surgery. Before switching to NAVA, 17 subjects (63%) were ventilated using pressure-control ventilation, 8 subjects (30%) using volume-control ventilation, and 2 subjects (7%) using pressure support ventilation. The NAVA level, initially set at 1.4 ± 0.6 cm H2O/μV, was at 1.3 ± 0.6 cm H2O/μV after 4 h. One subject was treated with NAVA for < 2 h in total.
Subject Characteristics
Characteristics of NAVA Episodes
Noninvasive NAVA was used, on average, 12.8 ± 10.0 d after surgery, for a duration equivalent to 53% (IQR 30−100%) of the total noninvasive ventilation period. Noninvasive NAVA resulted in successful weaning of ventilation (ie, no need for re-intubation) in 71% of cases.
Primary Outcome
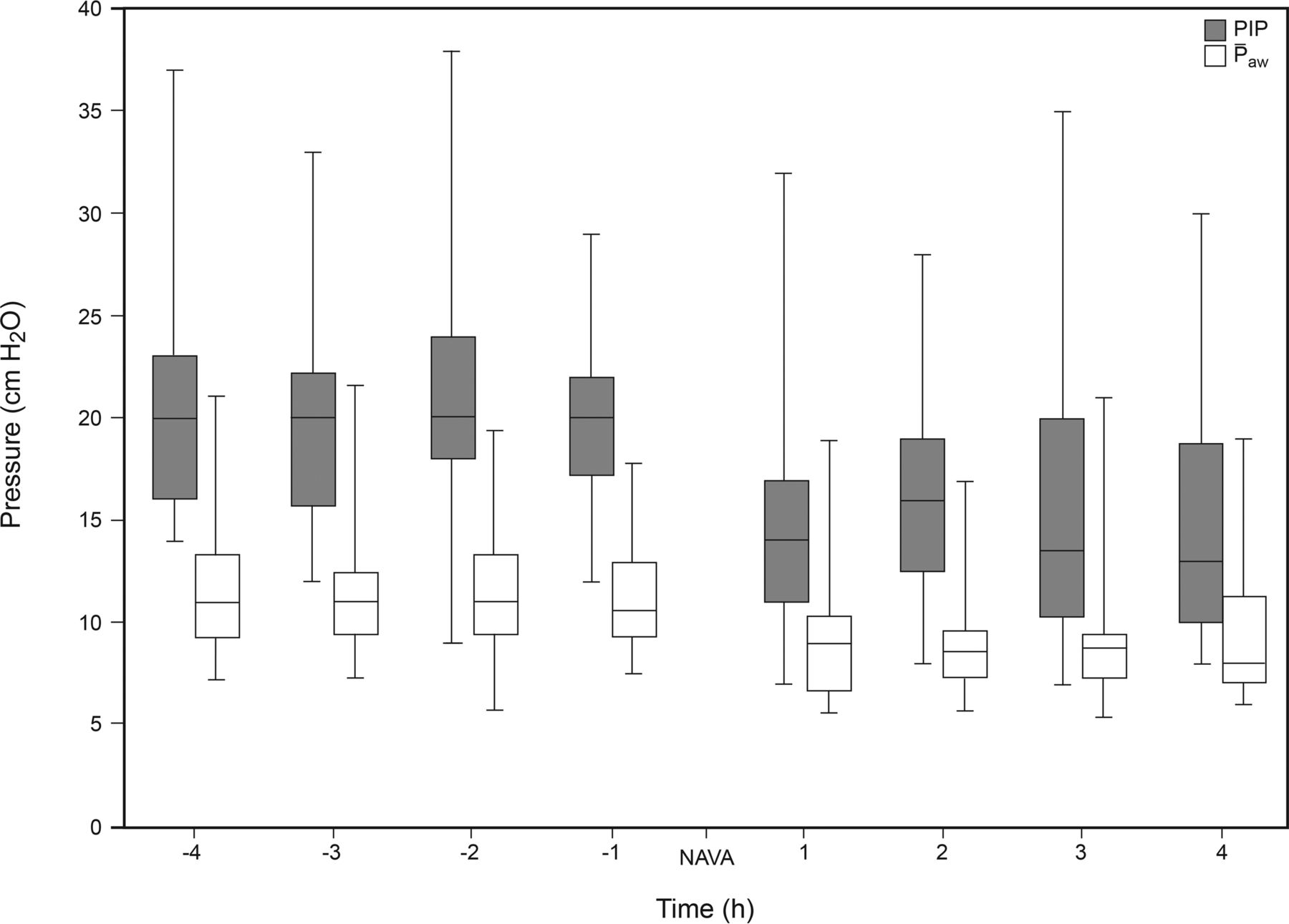
The evolution of ventilation pressures (PIP and ̄Paw) after the start of NAVA is depicted in Figure 2. A significant change of PIP and ̄Paw over time was observed (P < .001 for both, one-way repeated measures ANOVA). No change of pressure was observed among the 4-h periods in each mode (all P > .99, during both conventional ventilation and NAVA). Conversely, the 4-h average of PIP pre-NAVA (20.9 ± 5.2 cm H2O) was significantly higher than the average observed during the 4-h NAVA period (15.1 ± 4.9 cm H2O), with a mean difference of 5.8 cm H2O (95% CI 4.1–7.5; P < .001). A similar difference was observed for ̄Paw, from 11.3 ± 2.9 cm H2O during the pre-NAVA period to 9.3 ± 2.8 cm H2O during NAVA, with a mean difference of 2.0 cm H2O (95% CI 1.2–2.8; P < .001).

Evolution of peak inspiratory pressure (PIP) and mean airway pressure (̄Paw) in the 4 h preceding and following the start of neurally adjusted ventilatory assist (NAVA). Box plots illustrate the median values, interquartile range, and spread.
As illustrated in Figure 3, the pattern of ventilation pressure change was similar whether the subjects were at risk of right ventricular dysfunction or low pulmonary flow, and whether NAVA was used in the first 3 d after surgery or later in the PICU course.
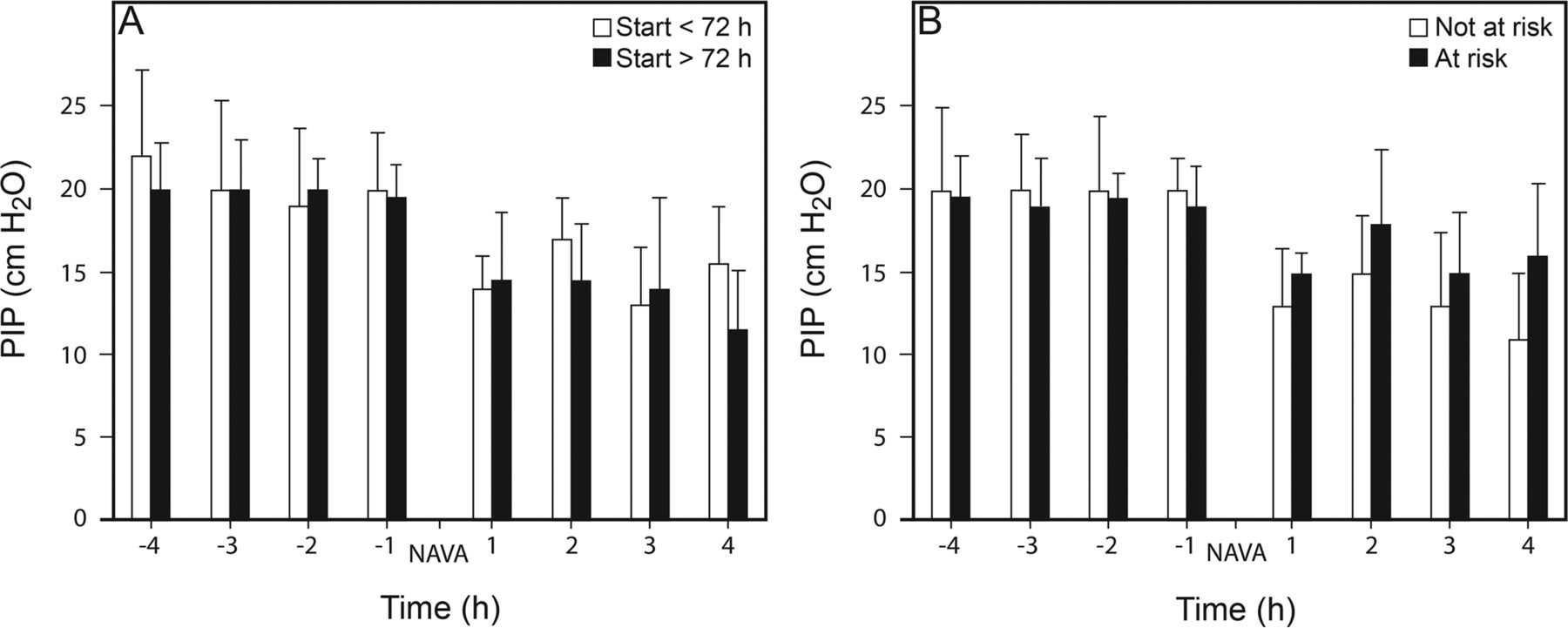
Evolution of peak inspiratory pressure (PIP) in the 4 h preceding and following the start of neurally adjusted ventilatory assist (NAVA) depending on the timing of NAVA initiation (before or after 72 h postadmission, A) or the presence of risk of right ventricular failure or low pulmonary flow (B). Data are presented as median with interquartile ranges.
Secondary Outcomes
As shown in Table 3, vital signs and blood lactate concentration did not change significantly after the switch to NAVA in subjects ventilated invasively. Breathing frequencies, tidal volumes, blood pH, and PaCO2 were not significantly different during the 4 h preceding NAVA than in the 4 h after the change in mode. Oxygenation was also stable, as indicated by the similarity of the SpO2/FIO2 and PaO2/FIO2 ratios (in subjects with blood gas values available both before and during NAVA). During NAVA, data were available in 24 subjects (89%), exhibiting an average pH of 7.39 ± 0.04, a PaCO2 of 45.1 ± 6.2 mm Hg, and a PaO2 of 123 ± 63 mm Hg.
Vital Signs and Laboratory Values Before and After Invasive NAVA Initiation
Discussion
This study illustrates the clinical feasibility of using NAVA in pediatric subjects after cardiac surgery. This ventilation mode was mostly well tolerated, although used in a small proportion of postoperative subjects, which likely represents those undergoing difficult ventilation weaning. When compared to the preceding conventional ventilation, invasive NAVA delivered a similarly effective ventilation with lower positive pressures. Noninvasive NAVA could also be used during ventilation weaning over a large proportion of the total noninvasive ventilation time.
There are few other studies describing the use of NAVA in this particular population. In a recent randomized cross-over study, short-term noninvasive NAVA (30 min) after extubation was shown to be effective in 10 infants who underwent cardiac surgery, with decreased work of breathing compared to nasal CPAP.15 Berger et al18 showed that NAVA had a smaller impact on right ventricular performance when compared with pressure support ventilation in 10 adults during the immediate postoperative cardiac course. Liet et al16 compared hemodynamic parameters in a physiologic pilot study of 6 children, finding lower inspiratory pressures and an increase in blood pressure when using NAVA compared to conventional ventilation. Although uncontrolled, our observational study reflects the use of NAVA in actual clinical practice in this specific population, and over longer periods of time. The study population characteristics suggest that invasive NAVA was not routinely used early in the postoperative course, but rather was used in a subset of subjects with protracted weaning and longer stay. One third of the courses, however, occurred in the first 3 d, with a similar impact on ventilation pressure. A more widespread use may have been limited by subjects receiving significant sedation or being extubated early in their postoperative course, as well as the limited availability of NAVA-compatible ventilators during the study period. Importantly, NAVA appeared feasible and well tolerated, with only one subject being ventilated with NAVA for < 2 h. The retrospective design of the study precluded exploring the reasons why NAVA was interrupted.
As we have observed, many previous studies have reported lower inspiratory pressures in children and infants ventilated with NAVA.9,10,19–23 The stability of vital signs and blood gas values in our study suggests that this decrease in ventilation pressures was not obtained at the cost of inadequate ventilation. The frequent decrease in positive Paw during NAVA while ventilation remains relatively stable is likely secondary to a greater contribution of the patient's own ventilation because of improved patient–ventilator interactions. This spontaneous ventilation induces patient-generated negative pleural pressure, thereby limiting the need for positive Paw. This mechanism has been confirmed by Doorduin et al,24 who showed that using NAVA in adults with ARDS resulted in lower Paw but relatively similar lung-distending pressure. Maintaining the patient's ventilatory efforts and thus negative pleural pressures is an important goal of postoperative care in cardiac subjects, unless significant left ventricle unloading is needed. Rapid extubation is frequently the objective,25 but is not always possible. In such cases, NAVA could be physiologically closer to spontaneous ventilation than other modes of assisted ventilation, as suggested by Berger et al,18 who observed improved right ventricular performance with NAVA as compared to pressure support ventilation in adults. Our study design did not allow for investigation of heart–lung interactions, and further studies are needed to confirm the positive impact of decreased positive Paw in pediatric cardiac patients.
In our study, NAVA was frequently used after several days of ventilation, and we hypothesize that it was specifically considered in subjects presenting protracted weaning. Many studies have shown that NAVA reduces patient–ventilator asynchrony, which is particularly frequent in pediatrics and is associated with adverse outcomes. Moreover, the continuous information provided by the EAdi signal enables more accurate adjustment of support to avoid over- or under-assist.17 This also allows care providers to titrate the level of support to the patient's own work of breathing and progressively lead to spontaneous ventilation. Although unilateral diaphragmatic paralysis can occur after phrenic nerve damage during cardiac surgery, it does not preclude recording an EAdi signal, and in a context where synchrony is important, NAVA could also be beneficial. In this perspective, we believe that NAVA has the potential to be a useful strategy for the weaning of patients with prolonged ventilation. Evidence of this benefit is still lacking, however. In a randomized, controlled trial involving 170 children, Kallio et al19 found that the length of PICU stay of subjects ventilated with NAVA was 23 h shorter (P = .10 in intention-to-treat analysis, P = .03 in per-protocol analysis).
Some limitations of our study should be addressed. Our analysis is retrospective and lacks a control group. Although the temporal pattern of ventilatory pressures strongly suggests an impact of the mode of ventilation (Fig. 2), an effect of time on patient evolution cannot be excluded. A significant proportion of our patient population was at risk for deleterious heart–lung interactions, but we were not able to show any improvement in hemodynamic status with decreasing Paw for several reasons. First, cardiac output is not routinely monitored in the PICU. Second, at the time of NAVA initiation, the frequency of blood gas analyses was relatively low, and few subjects had available data for pre- and post-NAVA comparisons. The data available in the medical charts did not allow assessment of patient–ventilator synchrony or work of breathing. Moreover, the study sample size did not allow for subgroup analysis according to the type of cardiac surgery. Querying the electronic medical chart nonetheless allowed for all subjects ventilated with NAVA during the study period to be included with only a few missing data. Finally, we describe the clinical experience of a single center that has long used NAVA, and the external validity of our results in different contexts is uncertain.
Conclusions
NAVA represents a ventilation strategy that is feasible in pediatric cardiac intensive care, especially during weaning. In addition to other proven benefits of synchronizing breath delivery with diaphragmatic activity, this strategy is associated with lower airway pressures. Prospective interventional trials are needed to further assess the impact of NAVA in these children, first on short-term cardiac function and pulmonary vascular resistance, and ultimately on important clinical outcomes (eg, comfort, duration of ventilation, and length of stay).
Acknowledgments
The authors thank the respiratory therapists, nurses, and fellows of the PICU for their collaboration.
Footnotes
- Correspondence: Guillaume Emeriaud MD PhD, CHU Sainte-Justine, Université de Montréal, 3175 Chemin de la Côte-Sainte-Catherine, Montréal, QC H3T 1C5, Canada. E-mail: guillaume.emeriaud{at}umontreal.ca.
Parts of the results of this study were presented by Benjamin Crulli at the 2016 Reanimation Congress, held January 13–15, 2016, in Paris, France.
Dr Emeriaud holds a Clinical Research Scholarship from the Fonds de la Recherche en Santé du Québec. He is also the principal investigator of an ongoing clinical study which is financially supported by Maquet Critical Care. He does not receive any salary nor any personal financial support from this company. The other authors have disclosed no conflicts of interest.
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}