

Abstract
BACKGROUND: There is a persistent concern over the risk of respiratory pathogen transmission, including SARS-CoV-2, via the formation of aerosols (ie, a suspension of microdroplets and residual microparticles after evaporation) generated during high-flow nasal cannula (HFNC) oxygen therapy in critically ill patients. This concern is fueled by limited available studies on this subject. In this study, we tested our hypothesis that HFNC treatment is not associated with increased aerosol formation as compared to conventional oxygen therapy.
METHODS: We used laser light scattering and a handheld particle counter to detect and quantify aerosols in healthy subjects and in adults with acute respiratory disease, including COVID-19, during HFNC or conventional oxygen therapy.
RESULTS: The use of HFNC was not associated with increased formation of aerosols as compared to conventional oxygen therapy in both healthy subjects (n = 3) and subjects with acute respiratory disease, including COVID-19 (n = 17).
CONCLUSIONS: In line with scarce previous clinical and experimental findings, our results indicate that HFNC itself does not result in overall increased aerosol formation as compared to conventional oxygen therapy. This suggests there is no increased risk of respiratory pathogen transmission to health care workers during HFNC.
Introduction
Health care workers are at increased risk for infectious respiratory diseases, including COVID-19, by working in close contact with infected patients. It has been well established that respiratory pathogen transmission occurs through large exhaled respiratory droplets, such as those produced during coughing. However, aerosols, consisting of a continuum of microdroplets and residual microparticles after evaporation (size < 5 µm), which have a much longer airborne time,1,2 may under specific circumstances constitute an important mode of spread of respiratory microbes and viruses.3,4 Not surprisingly, during the current global health care crisis related to COVID-19, concerns over the ability of certain respiratory medical interventions and procedures to generate aerosols carrying SARS-CoV-2 (bio-aerosols) have spiked.5-7
One of the respiratory interventions that remains a topic of active discussion in the clinical field regarding risk for bio-aerosol formation is oxygen therapy via high-flow nasal cannula (HFNC), a potentially beneficial respiratory support modality in critically ill patients in the ICU.6,8,9 It has been suggested that the high flow (ie, up to 60 L/min in adults) of warmed, humidified oxygen during HFNC treatment forced over respiratory mucosa generates aerosols. However, it is important to realize that expiratory flows during normal coughing or labored breathing without any respiratory support are much higher, which somewhat questions the relative importance and physiological basis for the view of HFNC as an aerosol-generating procedure.7 In fact, recent observational and experimental findings suggest that HFNC does not generate higher numbers of aerosols as compared to conventional oxygen therapy modalities.10-13 Likewise, clinical studies have not shown evidence of increased risk of transmission of SARS-CoV-1 and SARS-CoV-2 from subjects receiving HFNC to health care workers,14,15 nor is there evidence of increased surface or air dispersion of viral and bacterial pathogens.13,16
Although the above data together provide reassurance for the safety of HFNC regarding pathogen transmission during the COVID-19 crisis, the sample sizes of the individual studies so far, in particular those involving actual patients with acute (infectious) respiratory disease, are small.13 This may fuel the hesitant approach or even avoidance of HFNC treatment for patients with COVID-19.6,8,17 Therefore, to gain further evidence on this subject, we aimed to test our hypothesis that HFNC treatment is not associated with increased aerosol formation as compared to conventional oxygen therapy in patients with acute respiratory diseases, including COVID-19.
QUICK LOOK
Current Knowledge
Aerosols play a role in the transmission of pathogens, including SARS-CoV-2. Respiratory care therapies that generate aerosols may increase this risk to health care workers who come in close contact with infected patients. There is an ongoing debate about whether oxygen therapy via high-flow nasal cannula leads to increased risk of aerosol formation.
What This Paper Contributes to Our Knowledge
In both healthy adults and subjects with acute respiratory diseases, including COVID-19, the use of high-flow nasal cannula was not associated with increased aerosol formation as compared to conventional oxygen therapy delivered via a non-rebreather mask or low-flow nasal cannula.
Methods
This study was approved by the local medical ethical committee at the Amsterdam UMC, location AMC (2020_098/NL73585.018.20 and W20_321#20.353), which is where this study took place.
Detection of Aerosols in Healthy Subjects
We visually detected and quantified both large respiratory droplets and aerosols in 3 healthy volunteer adults, similar to our previous descriptions.1,4 Particles and droplets were detected in complete darkness with a SprayScan (Spraying Systems, Glendale Heights, Illinois) laser sheet during normal, unsupported breathing and during breathing while receiving treatment with either a non-rebreather mask (Salter Labs, Lake Forest, Illinois) at 15 L/min or HFNC (Fisher & Paykel Healthcare, Auckland, New Zealand) at 34–37°C and 60 L/min. As a positive control, these subjects were also asked to cough to generate both large respiratory droplets and aerosols,1,4 and they received normal saline (NaCl 0.9%) nebulization through the HFNC system to generate aerosolized microparticles. Quantification (light pixels) with ImageJ software was performed as described previously.4,18 All subjects received the different treatments in crossover, and measurements were carried out after ∼ 5 min per experimental condition. The experimental lab space in which the measurements took place is a dust-free room (ie, to minimize serious background signals) that was kept at a constant temperature of 20.5 ± 0.5°C, with a measured relative humidity of 45 ± 3% and normal atmospheric pressure. Laser diffraction measurement using a spray particle/droplet measurement system with wavelength of 0.6 µm (Malvern Spraytech, Malvern, United Kingdom) was used to determine size distribution of the positive aerosolized microparticle control test using normal saline nebulization via the HFNC system.4,18
Detection of Aerosols in Patients
We prospectively included adult subjects receiving conventional oxygen therapy via a non-rebreather mask or low-flow nasal cannula and subjects receiving oxygen therapy via HFNC for various acute respiratory diseases in the ICU or the specialized COVID-19 ward. Subjects were treated inside negative pressure rooms up to –7.5 kPa. As direct visualization of aerosols with a laser sheet in the dark is not possible in these subjects, we used a particle counter (Royco HH200, PACSCI EMC, Hollister, California) to detect microparticles with diameters of 0.5 µm and 5.0 µm during 15 s of air sampling at 2 distances (30 cm and 1 m) in 4 positions around the head of the subject (left, right, rear, front) to assess for dispersion in all directions. Previously, we validated the technique of using a handheld particle counter to detect aerosol formation.18 In addition, we separately measured aerosolized microparticles generated during normal saline nebulization through a HFNC system as a positive control for detection of aerosols by the handheld particle counter.
Statistical Analysis
Data from the healthy adults are derived from 2 separate experiments per condition per subject; they are presented as means ± SEM and were analyzed with repeated measures analysis of variance with a post hoc least significant differences test. Data from measurements in the subjects are presented as proportions and medians (interquartile range) and analyzed with the Fisher exact test or Mann-Whitney U test. P < .05 was considered statistically significant. Data analysis was performed with SPSS 26 (IBM, Armonk, New York).
Results
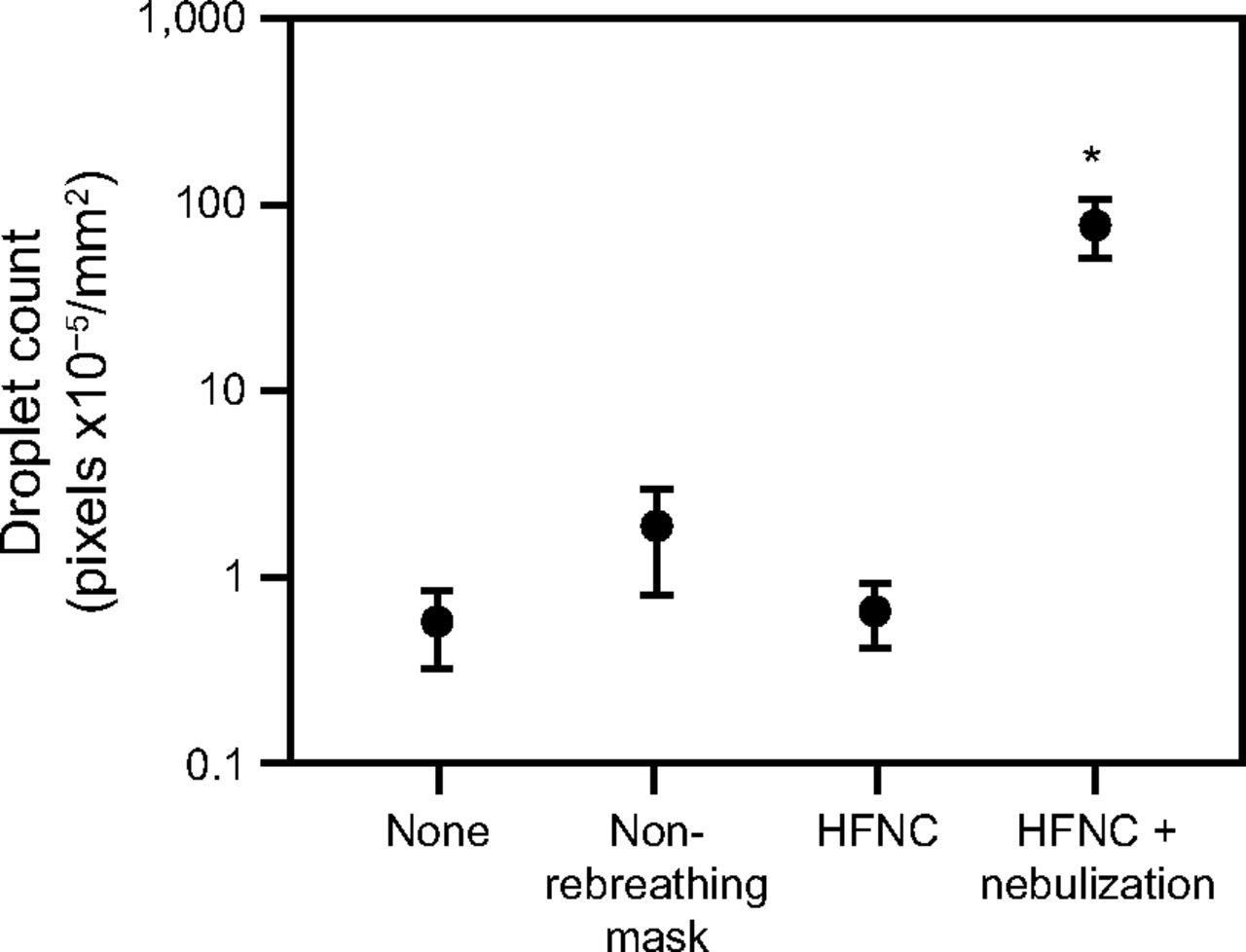
First, to have a more general estimation of the ability of HFNC to generate aerosols, we visualized and quantified particles/droplets generated by healthy adults breathing either unsupported or while receiving oxygen through a non-rebreather mask or HFNC. To have the highest chance to detect particle emission, we compared these conditions while subjects were breathing with their mouth open. As compared to unsupported breathing or a non-rebreather mask, HFNC treatment was not associated with increased aerosol formation. Normal saline nebulization through the HFNC system to generate aerosolized microparticles as a positive control indeed resulted in much higher numbers of aerosols (Fig. 1). With laser diffraction the size of these nebulized normal saline particles was well below 10 µm, confirming the size range of aerosols (Fig. 2). Similarly, no increased HFNC-mediated aerosols during other conditions, such as closed mouth breathing, using differential flow speeds (ie, 10–60 L/min), or upon intranasal inhalation of normal saline to mimic rhinitis, were observed in a set of separate experiments (data not shown). In addition, upon visualization of aerosols detected during HFNC treatment, these numbers were negligible when we compared them to the cloud of both large respiratory droplets and aerosols generated during a normal cough of a so-called “high emitter” (Fig. 3).4 However, as the expiratory flow generated during coughing maneuvers is highly variable in both rate and direction, we did not directly compare this further.

Aerosol detection. Detected particles/droplets (quantified by maximum light pixels/mm2) during open-mouth breathing during no oxygen support (none), non-rebreathing mask (NRM, 15 L/min), HFNC (60 L/min), and HFNC with normal saline nebulization (positive control for generating aerosolized microparticles). *P = .032 by repeated measures analysis of variance with post hoc least significant difference (LSD) analysis, as compared to all other groups. Data (mean ± SEM) from 3 subjects measured twice in separate experiments. HFNC = high-flow nasal cannula.

Aerosol size range from normal saline nebulization. Microparticle size distribution detected with laser diffraction during normal saline nebulization via high-flow nasal cannula treatment (positive control for generating aerosolized microparticles).

Aerosol visualization patterns. Particle/droplet visualization with laser light scattering from a healthy adult with the face oriented sideward from the left side. A: Receiving HFNC at 60 L/min; (B) during a single cough without respiratory support; and (C) during HFNC with normal saline nebulization for positive control of visualization of aerosolized microparticles. HFNC = high-flow nasal cannula.
Second, as healthy volunteers obviously lack mucus hypersecretion associated with infectious respiratory diseases and may thus introduce a type-2 error, we measured aerosol formation in subjects receiving conventional oxygen therapy via a non-rebreather mask or low-flow nasal cannula and compared this to subjects receiving therapy via HFNC. A total of 17 subjects with acute respiratory diseases receiving either conventional oxygen or HFNC treatment admitted to the ICU (n = 13) or to a specialized COVID-19 ward (n = 4) were included in the study (Table 1). In 9 (53%) of the subjects, the underlying disease was COVID-19. As expected, subjects on HFNC received higher flows as compared to the conventional group (P = .001) (Table 1). However, both groups had similar median counts for both the 0.5 µm and the 5.0 µm aerosol sizes as sampled at distances of 30 cm and 1 m from the subject (Table 2). No differences between the number of aerosols and the level of pressure inside the rooms was found. As a positive control for the handheld particle counter, normal saline nebulization through a HFNC system results in median (interquartile range) aerosolized microparticle counts that are of several orders of magnitude greater: 224.6 × 103 (180.3–311.7 × 103) and 2.2 × 103 (1.3–6.8 × 103) for 0.5 µm and 5.0 µm particle sizes, respectively.
Subject Characteristics
Aerosol Detection
Discussion
The main finding of this study of aerosol dynamics is that HFNC treatment itself is not associated with increased aerosol formation, as determined in both healthy subjects and critically ill subjects (n = 17) with acute respiratory disease, including COVID-19.
Our findings are in line with a very recent study among 9 subjects with COVID-19,13 as well as recent experimental observations in 10 healthy subjects.10 Importantly, our findings provide further scientific basis for studies that have failed to detect increased dispersion of bacteria or viruses, such as SARS-CoV-1, SARS-CoV-2, to surrounding surfaces or air during HFNC.13,16 In contrast, Ahn et al19 detected viable SARS-CoV-2 particles in environmental swabs, though in that case-study the only subject who received HFNC was also subsequently treated with noninvasive ventilation. Recently, Vianello et al14 reported a case series of 28 patients with COVID-19 treated with HFNC. The authors reported that none of the staff (wearing FFP2 masks) working in close contact with these patients had a positive SARS-CoV-2 PCR test within a 14-d period. Such studies underline prior views of the safety of HFNC during this current COVID-19 health crisis.9,12
By the combined effort of these studies, derived by different investigator groups in various patient cohorts, using a number of aerosol and pathogen detection methods, the risk of bio-aerosol generation during HFNC appears to be low. However, a clear limitation to studying aerosol dynamics in relation to the transmission of novel pathogens such as SARS-CoV-2 is our current lack of understanding of virion stability and infectivity (ie, the number of virions needed to produce an active infection).4,20 It should thus be noted that aerosol detection findings in the setting of HFNC, such as in this study, without measurements of virus particles or transmission to health care workers must be cautiously interpreted.17 Nevertheless, the stark contrast between our findings of low aerosol formation during HFNC treatment and the very high numbers of both large respiratory droplets as well as aerosols that can be produced by a normal single cough or sneeze, as clearly demonstrated in various studies,2,4 at least suggests that we should do our best to protect health care workers from this type of transmission risk while they work in close contact with patients, regardless of whether they receive any form of respiratory support.
Conclusions
Our study of healthy and critically ill adult subjects, including those with COVID-19, provides additional evidence to bolster the scarce previous findings that HFNC is not associated with increased aerosol formation. Further research investigating modes and risk of pathogen (SARS-CoV-2) transmission to health care workers is urgently needed.
ACKNOWLEDGMENTS
Of the Amsterdam UMC, we thank Niels W Rutjes MD (Department of Pediatric Pulmonology), as well as Dick Markhorst MD PhD and Job BM van Woensel MD PhD (Department of Pediatric Intensive Care), for a fruitful discussion on this study and implications. We thank D. Giesen (Institute of Physics, UvA) for expert technical assistance.
Footnotes
- Correspondence: Reinout A Bem MD PhD, Meibergdreef 9, 1105AZ Amsterdam, The Netherlands. E-mail: r.a.bem{at}amsterdamumc.nl
See the Related Editorial on Page 1039
Drs Bem and van Mourik are co-first authors.
The authors have disclosed no conflicts of interest.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}