

Abstract
Intermittent mandatory ventilation (IMV) is one kind of breath sequence used to classify a mode of ventilation. IMV is defined as the ability for spontaneous breaths (patient triggered and patient cycled) to exist between mandatory breaths (machine triggered or machine cycled). Over the course of more than a century, IMV has evolved into 4 distinct varieties, each with its own advantages and disadvantages in serving the goals of mechanical ventilation (ie, safety, comfort, and liberation). The purpose of this paper is to describe the evolution of IMV, review relevant supporting evidence, and discuss the rationales for each of the 4 varieties. Also included is a brief overview of the background information required for a proper perspective of the purpose and design of the innovations. Understanding these different forms of IMV is essential to recognizing the similarities and differences among many dozens of different modes of ventilation. This recognition is important for clinical application, education of caregivers, and research in mechanical ventilation.
Introduction
Intermittent mandatory ventilation (IMV) is a term used to describe modes of ventilation that allow both mandatory and spontaneous breaths. IMV has a long history, perhaps dating back as far as the late 1880s.1 IMV is not a “mode” of ventilation per se but rather one component of a mode classification. Indeed, over many decades of technological innovation, IMV has evolved into 4 distinct varieties, each with its own advantages and disadvantages in serving the goals of mechanical ventilation (ie, safety, comfort, and liberation. The purpose of this paper is to describe the evolution of IMV, review relevant supporting evidence, and discuss the rationales for each of the 4 varieties. We include a brief overview of the background information required for a proper perspective of the purpose and design of the innovations. Understanding these different forms of IMV is essential to recognizing the similarities and differences among many dozens of different modes of ventilation. This recognition is important for clinical application, education of caregivers, and research in mechanical ventilation.
To begin with, a mode of ventilation is a predetermined pattern of patient-ventilator interaction. A mode taxonomy or classification system has been described in which modes are characterized in terms of (1) the control variable, (2) the breath sequence, and (3) the targeting scheme(s).2
The control variable designation is based on the equation of motion for the respiratory system. There are many forms of this equation, but the one given here is most appropriate for classifying modes of ventilation:
 where Pvent is airway pressure above baseline PEEP, Pmus is the pressure generated by the ventilatory muscles, V is volume above end-expiratory volume, V̇ is flow, E is elastance, and R is resistance. Based on this equation, pressure control (PC) modes are defined as those where the ventilator controls the left-hand side of the equation (ie, Pvent is a preset target value, or the ventilator adjusts pressure so that it is proportional to Pmus). Once pressure is controlled, tidal volume (VT) and V̇ are dependent on E and R. In contrast, volume control (VC) modes are those for which the right-hand side of the equation is predetermined (ie, both VT and inspiratory V̇ are preset). Once VT and V̇ are controlled, Pvent depends on E and R.2 In general, the control variable in a mode classification refers to mandatory breaths during passive inflation (ie, Pmus = 0). In either PC or VC, flow is the manipulated variable in the feedback control system, not to be confused with a control variable.3,4
where Pvent is airway pressure above baseline PEEP, Pmus is the pressure generated by the ventilatory muscles, V is volume above end-expiratory volume, V̇ is flow, E is elastance, and R is resistance. Based on this equation, pressure control (PC) modes are defined as those where the ventilator controls the left-hand side of the equation (ie, Pvent is a preset target value, or the ventilator adjusts pressure so that it is proportional to Pmus). Once pressure is controlled, tidal volume (VT) and V̇ are dependent on E and R. In contrast, volume control (VC) modes are those for which the right-hand side of the equation is predetermined (ie, both VT and inspiratory V̇ are preset). Once VT and V̇ are controlled, Pvent depends on E and R.2 In general, the control variable in a mode classification refers to mandatory breaths during passive inflation (ie, Pmus = 0). In either PC or VC, flow is the manipulated variable in the feedback control system, not to be confused with a control variable.3,4
The breath sequence is the pattern of mandatory and spontaneous breaths allowed by the mode, whether they occur or not. A mandatory breath is defined as one for which the inspiratory phase is triggered (started) or cycled (ended) by the machine (ventilator).2 Machine triggering is most often accomplished with a preset breath rate, whereas machine cycling is most often determined by a preset VT or inspiratory time. In contrast, a spontaneous breath is one for which the inspiratory phase is both triggered and cycled by the patient.2 Patient triggering is most commonly achieved using inspiratory pressure or flow signals, and patient cycling is usually by flow or pressure signals (although many different signals can be used for each). It follows that there are 3 possible breath sequences: continuous mandatory ventilation (CMV) with all mandatory breaths, IMV with both mandatory and spontaneous breaths, and continuous spontaneous ventilation (CSV) with all spontaneous breaths.
A target is a predetermined goal of ventilator output, such as parameters of the pressure, volume, and flow waveforms (ie, peak inspiratory pressure, PEEP, VT, and peak inspiratory flow, respectively).2 A targeting scheme is a model of the relationship between operator inputs and ventilator outputs to achieve a specific ventilatory pattern, usually in the form of a feedback control system. Examples of targets and targeting schemes are shown in Table 1. A full description of the various targeting schemes is beyond the scope of this paper, but has been described extensively elsewhere.2,5
Example Targeting Schemes and Targets
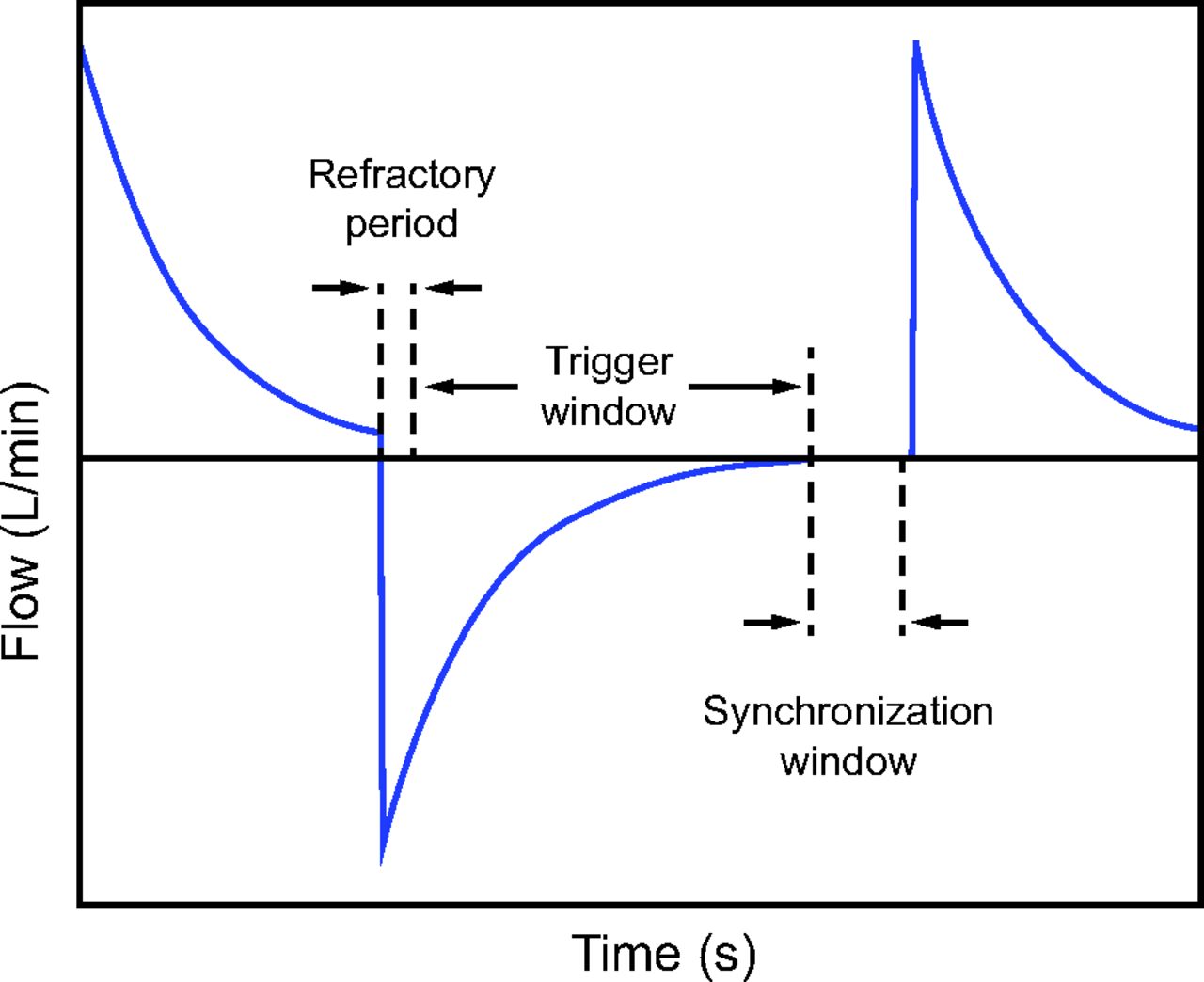
On the basis of these preliminary concepts, IMV is formally defined as a breath sequence for which spontaneous breaths are permitted between mandatory breaths.2 If a synchronization window is used to coordinate ventilator flow with inspiratory effort, it is called synchronized IMV (SIMV). Synchronization of mechanical inflation with the patient’s inspiratory effort is associated with lower airway pressures, improved hemodynamics, and reduced risk of ventilator-induced lung injury.6 A synchronization window is a short period (eg, 5 s) at the end of a preset expiratory time (ie, as a function of preset inspiratory time and breath rate) during which a patient signal may be used to synchronize the trigger event with a patient inspiratory effort signal. Therefore, if a patient inspiration effort signal appears in the synchronization window, and it is large enough to meet the trigger sensitivity criterion, then the inspiration is patient triggered. Generally, such an inspiration is machine cycled and hence results in a mandatory breath. Patient triggering in the synchronization window shortens the expiratory time, so the ventilator usually extends the expiratory time before the next breath to keep the set mandatory breath rate constant.
The portion of expiratory time that is not in the synchronization window is called the trigger window (Fig. 1). During the trigger window (minus a short refractory period to prevent inadvertent double triggering) a sufficiently large patient signal can start inspiration (ie, a patient-triggered, patient-cycled spontaneous breath). Such a spontaneous breath may or may not be assisted (eg, pressure support or PEEP, respectively). Note that the definition of a spontaneous breath has nothing to do with the level of assistance (ie, the proportion of inspiratory work provided by the ventilator).

Trigger and synchronization windows used to create intermittent mandatory ventilation.
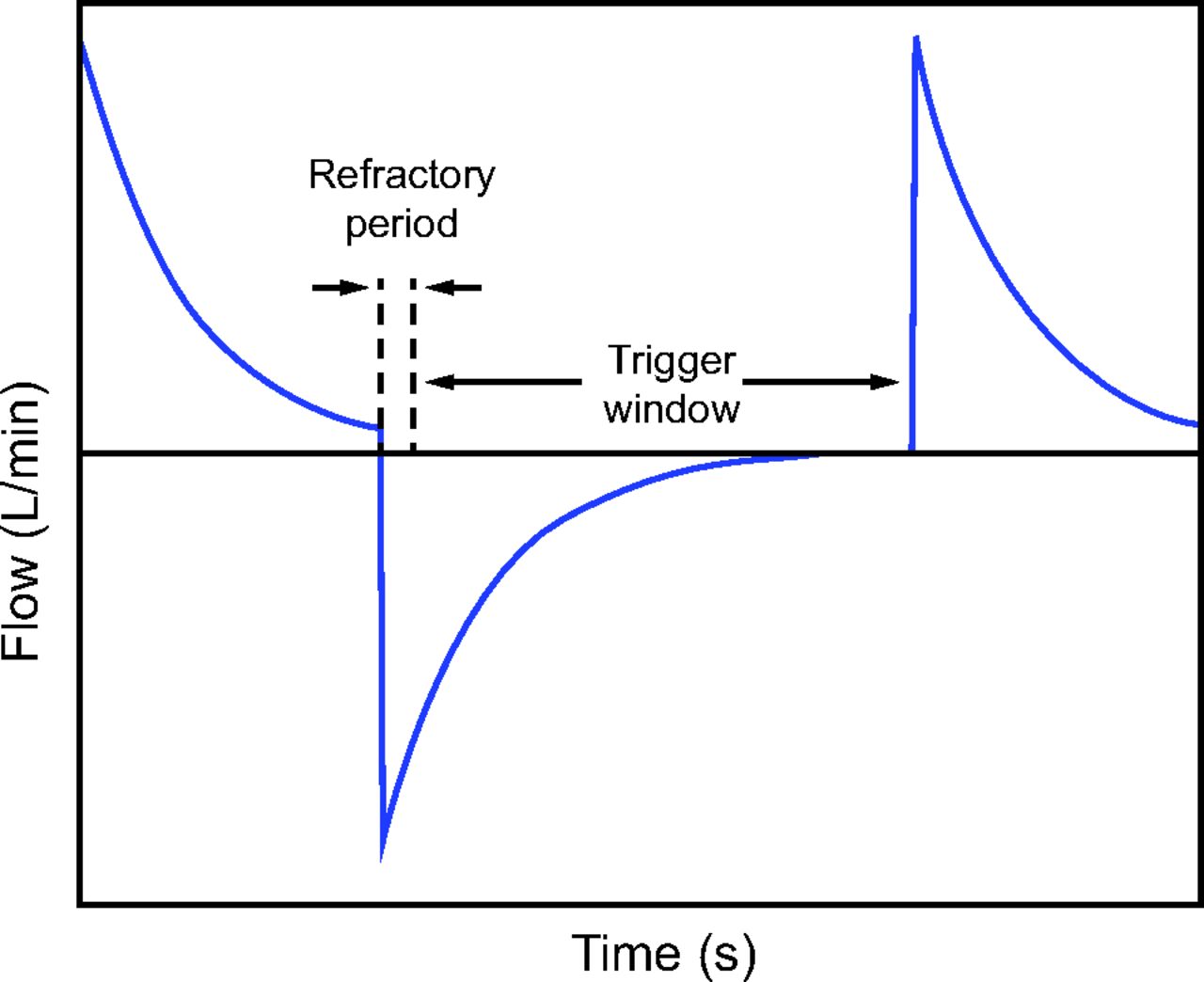
A trigger window (without a synchronization window) is used to create CMV (also known as assist/control) or CSV (ie, pressure support) as shown in Figure 2. The distinction between a synchronization window and a trigger window is what makes the set mandatory breath rate the highest possible for IMV and the lowest possible for CMV. That is, the synchronization window only allows patient triggering of a prescheduled mandatory breath and does not increase the set mandatory breath rate; but patient triggering may decrease it for IMV(2), IMV(3), and IMV(4). On the other hand, the trigger window permits a new mandatory breath between 2 scheduled (by set rate) mandatory breaths, hence increasing the total mandatory breath rate in CMV.

Trigger window used to create continuous mandatory ventilation and continuous spontaneous ventilation.
Some ventilators use an “active exhalation valve” for IMV modes so that spontaneous breaths are possible during PC mandatory breaths.7 Some ventilators do not. Some ventilators offer both on different modes. Note that if such a spontaneous breath occurs during PC CMV it does not turn CMV into IMV because it does not affect the mandatory breath rate. This is the reason that IMV is defined as a breath sequence for which spontaneous breaths are permitted between mandatory breaths, a definition that may not be intuitively obvious at first.
Finally, the symbol for a mode classification (ie, the tag, or taxonomic attribute grouping) has 3 components representing (1) the control variable (VC or PC), (2) the breath sequence (CMV, IMV, or CSV), and (3) the targeting scheme (s, d, r, a, b, o, i) for both mandatory and spontaneous breaths (if allowed). Specifically, for IMV, at least 2 symbols are used where the first refers to the mandatory breaths and the second to the spontaneous breaths.2 For example, the mode called SIMV PRVC (Servo ventilators) is classified as PC-IMV(1)a,s.
All modes on all ventilators used in the United States have been classified using the mode taxonomy in a recent textbook.5 The database used to write this book is maintained by one of the authors of this paper (RC) and is distributed on a telephone app called Ventilator Mode Map (free download for iPhone and Android). This database (which is continually updated) was used to estimate the number of mode names that are classified as various forms of IMV as described below. Note that we must distinguish mode names (ie, brand names invented by manufacturers for marketing purposes) from mode classifications for the same reasons we must distinguish drug brand names from generic names. Failure to do this introduces many problems, including inaccuracy in research comparing modes. For example, a recent meta-analysis by Jhou et al8 on weaning outcomes uses search terms including “Pressure Support Ventilation,” “Synchronized Intermittent Mandatory Ventilation,” “Automatic Tube Compensation,” “Continuous Positive Airway Pressure,” “Adaptive Support Ventilation,” “Neurally Adjusted Ventilatory Assist,” “Proportional Assisted Ventilation,” and “SmartCare.” These are all brand names of modes (rather than generic classifications) and as such are not representative of all modes that could be used for weaning. Furthermore, the meta-analysis only included one kind of IMV (that they called SIMV), which implies that the distinction among the 4 different kinds of IMV is irrelevant. The purpose of this article is to explain why such a distinction is indeed relevant.
History of IMV
Kacmarek and Branson9,10 gave a brief history of conventional IMV but did not cover its evolution to more sophisticated forms. Downs et al11,12 coined the term intermittent mandatory ventilation in 1973 in reference to adult VC ventilation. It was thought to promote weaning from mechanical ventilation by gradually decreasing the mandatory breath rate and the patient would maintain minute ventilation by increasing the spontaneous breath rate.13 This procedure, however, was later found to delay extubation.9 Of note, Kirby et al14 2 years earlier had described this functionality in a new PC infant ventilator that was later to be marketed as the Baby Bird (now obsolete).
In 1977, Hewlett and colleagues15 proposed a new mode called mandatory minute ventilation (MMV), which also allows spontaneous breaths to occur between mandatory breaths but with more theoretical advantages compared to the original IMV. What makes MMV different from conventional IMV is that the mandatory breaths do not appear if the preset minute ventilation target is met by the patient’s spontaneous breaths. Over time, MMV evolved into even more capable modes like adaptive support ventilation (ventilators made by Hamilton Medical, Bonaduz, Switzerland)16 and adaptive ventilation mode (the bellavista ventilator made by Vyaire Medical, Mettawa, Illinois).17
In 1989, the spontaneous/timed (S/T) mode was invented by the engineers from Respironics (now Koninklijke Philips, Amsterdam, the Netherlands) with the feature that “the system automatically triggers to the IPAP mode for just long enough to initiate patient inspiration if the system does not sense inspiratory effort within a selected time after exhalation begins.”18 It was originally invented for use in patients with sleep apnea because mandatory breaths are not as comfortable as spontaneous breaths (perhaps causing sleep fragmentation19) but are essential when the patient stops triggering breaths. S/T is essentially pressure support (normally all spontaneous breaths in conventional forms of pressure support) but with a backup rate for mandatory breaths. Yet this backup rate is not used in an alarm condition (ie, apnea) but rather built into the mode such that if the spontaneous breath rate is higher than the set mandatory breath rate then mandatory breaths will be suppressed. Hence, this is a form of IMV by definition. The S/T mode has become very popular with home care ventilators and even appears on some ICU ventilators.
Finally, Servo ventilators (Getinge, Göteborg, Sweden) have yet another variation of IMV using a unique feature for VC modes called “Flow Adaptation.” Under passive conditions, inspiration is delivered at a constant target flow calculated as the VT divided by the inspiratory flow time. Inspiratory flow time is the inspiratory time minus the pause time (if used). Inspiration is cycled off when the VT is delivered (or when the inspiratory pause time expires). However, if the patient makes an inspiratory effort during the preset inspiratory flow time, and this effort is large enough to make airway pressure drop by at least 3 cm H2O, then the ventilator switches from VC to PC with enough extra flow to maintain at least the PEEP pressure. During PC, inspiratory flow naturally decreases as the VT is delivered. If the inspiratory effort is short and flow decreases back to the VC target flow, the ventilator switches back to VC at constant flow, and inspiration is again cycled off when the VT is delivered (but the added flow and volume shorten the inspiratory flow time). However, if the inspiratory effort is long enough, and flow does not decrease to the VC target flow by the time the preset inspiratory time has elapsed, then inspiration is flow cycled, as in a pressure support breath, and the VT is larger than the preset volume.20 Now, if this breath was machine triggered, it is still a mandatory breath. However, if it was patient triggered, it is a spontaneous breath because it was flow (patient) cycled. Flow cycling is classified as patient cycling because the inspiratory time is determined by the patient’s respiratory system mechanics (resistance, compliance, and ventilatory muscle activity), not by a preset inspiratory time on the ventilator.
Evidence Supporting Different Types of IMV
In general, modes of ventilation have been approved by regulatory bodies and marketed without much scientific evidence of safety or efficacy.21 This is in stark contrast to the process for introducing new drugs. It may, in fact, be impossible to prove safety and efficacy of individual modes in a practical manner because the mode of ventilation plays a relatively small role in major patient outcomes such as morbidity and mortality. Hence, we may have to suffice with theoretical analyses of benefit. In this section we will give examples of the 4 types of IMV and describe their ability to serve the 3 goals of mechanical ventilation. These goals are (1) safety, or the ability to maintain adequate gas exchange and protect the lungs from risk of ventilator-associated lung injury; (2) comfort, or the ability to maintain adequate patient-ventilator synchrony22 with an appropriate balance of work output from the ventilator compared to that of the patient; and (3) liberation, or minimizing the duration of ventilation and risk of adverse events, such as failed extubation.23 Note that as it relates to the safety goal, volume delivery is a critical factor; the dosage is just as important as it is for drug administration. Dosages that are too small or too large can be life threatening. Many years of research have supported the notion that safe VT dosage is in the range of 4–8 mL/kg ideal body weight for sick adult24 and pediatric lungs25 as well as normal lungs.26 Normalization of VT by respiratory system compliance (instead of ideal body weight) may be even more important.27 This metric is often called “driving pressure” but is more accurately called tidal pressure because it is simply VT scaled by a constant (ie, compliance or elastance).28
In the next section we will assess the ability of each type of IMV to serve these goals (ie the rationales for various IMV types). Where possible, we will provide references to studies that provide supporting evidence. Otherwise, our assessment will be theoretical.
There is no standardization of mode names among ventilator manufacturers. As a result, there are many unique names for modes that have the same classification (like the situation with drugs).2 Table 3 shows this diversity by listing some of the mode names on common ICU ventilators grouped by IMV type.
Four Types of IMV
Clearly, IMV has undergone a radical evolution over the last half century. Yet amazingly, this fact has not been recognized in research papers or explained in textbooks (with 2 exceptions5,22). For this reason, most clinicians fail to see that an important change has taken place. As a result, they don’t appreciate the fact that modes of ventilation have become very sophisticated and that old ways of thinking about IMV (such as believing it is an inefficient weaning mode) are outdated.10 The best way to remedy this situation is to include the different kinds of IMV into the formal taxonomy for modes of ventilation.2 Recognizing the type of IMV from the ventilator’s graphical displays is often difficult. Although identification may be possible if enough time is spent observing the patient, a more practical approach is to simply read the description of the mode in the ventilator’s operator manual or look up the mode in a classification table.5 Below are descriptions of the 4 different types of IMV (see Table 2).
Definitions for Different Types of Intermittent Mechanical Ventilation
Description of IMV(1)
IMV(1) means that mandatory breaths are always delivered at set breath rate.
Volume-controlled IMV (VC-IMV) for adults started out as a patient circuit modification made by clinicians because ventilators (for adult patients) only provided CMV. Note that infant ventilators at this time only provided pressure-controlled IMV (PC-IMV), and this was because in those days (early 1970s) the technology was not available to accurately trigger mandatory breaths for infants with erratic inspiratory efforts.14 Adult ventilators were modified by inserting anesthesia bags and one-way valves in the patient circuit and supplying the bags with a continuous flow of air/oxygen to support spontaneous breathing between the mandatory breaths. The idea was that to wean patients all you had to do was gradually decrease the mandatory breath rate and the patient would maintain minute ventilation by increasing the spontaneous breath rate. It was not long before ventilator manufacturers started to build this feature into their modes. This is called IMV(1) where mandatory breaths are delivered at the set rate regardless of what the patient does. An example would be a mode called SIMV PC (Puritan Bennett 980 ventilator made by Medtronic, Minneapolis, Minnesota). However, there are data to suggest that, for most patients, IMV(1) prolongs the weaning process compared to daily spontaneous breathing trials followed by sudden discontinuation of ventilation.9 This is no doubt due to the requirement for manual adjustment of the mandatory breath rate.
Rationale for IMV(1)
There are at least 225 unique mode names that are classified as IMV(1).5 Example modes on common ICU ventilators are shown in Table 3.
Example Mode Names Classified as Forms of Intermittent Mechanical Ventilation
Safety
Modes classified as IMV(1) assure adequate gas exchange by providing a minimum MMV because of the set mandatory VT and breath rate. Therefore, the goal of safety is served (in terms of gas exchange and lung protection) assuming the operator selects appropriate values for VT dosage and mandatory breath rate.7,8
Comfort
For most types of IMV(1), mandatory breath delivery can be synchronized with the patient’s inspiratory effort, assuming that the efforts are large enough relative to the trigger sensitivity setting. However, mandatory breaths are still machine cycled, and hence dyssynchronies may occur in the form of early or late cycling of inspiration.22 In the 20th century, IMV(1) was thought to produce less patient-ventilator discordance as compared to CMV.29 However, as the evolution of IMV modes has advanced for decades, recent studies have found IMV(1) to be associated with patient-ventilator discordance as high as 11%.30 Furthermore, SIMV algorithms of various manufacturers and models deliver ventilation rates with significantly different degrees of synchronization.31 Zhou et al32 found that during VC-IMV(1) higher inspiratory flow was associated with a higher risk of discordance. Robinson et al33 found discordance was more common in IMV(1) with set breathing frequencies of > 10 breaths/min in trauma subjects. In children ventilated with PC-IMV(1), those with higher VT who have a set ventilator rate close to their spontaneous respiratory rate are more likely to have early triggering (also known as reverse triggering), which results in breath-stacking > 25% of the time.34
Note that there are some modes classified as IMV(1) that do not allow patient-triggered breaths (eg, the mode named PC-CMV on the Babylog VN500 ventilator made by Dräger Medical, Lübeck, Germany). The same is true for modes classified as CMV (ie, the modes named PCV or timed on the Vyaire bellavista ventilator). The idea, apparently, is that sometimes patients are connected to a ventilator during cardiopulmonary resuscitation and the intent is to avoid inadvertent triggering due to compressions.
Liberation
IMV(1) was invented as an aid to weaning. It enables gradual weaning by decreasing the rate of mandatory breaths11,35,36 as opposed to decreasing the VT in CMV or switching to CSV (ie, pressure support or CPAP). However, manually decreasing the mandatory rate may introduce a delay in weaning for several reasons. First, if spontaneous breaths between mandatory breaths are assisted with pressure support, and if the assistance results in spontaneous VT dosage the same as mandatory breaths, then simply decreasing the mandatory rate does little to reduce ventilatory support (except possibly decreasing mean airway pressure). Second, this procedure implies periodic reassessment of the patient (eg, during daily rounds), and the delay between these assessments may be unnecessarily long.13,37 Landmark studies in the 1990s demonstrated that IMV(1) was the poorest approach to determining whether patients are ready for ventilator discontinuation.9 Esteban et al38 showed that a once-daily trial of spontaneous breathing led to extubation about 3 times more quickly than IMV and about twice as quickly as pressure support ventilation. Brochard et al39 showed that when all causes for weaning failure were considered a lower number of failures was found with pressure support (classified as pressure controlled CSV, PC-CSV) than with T-piece or IMV(1).
On the other hand, one recent study comparing CMV with IMV(1) in adults showed no significant differences in hospital length of stay, duration of mechanical ventilation, mortality, failed extubation, and the need for tracheostomy.40 Certainly, IMV(1) is still commonly used and poses no threat to patient care so long as it can be manually adjusted at appropriate intervals. In situations where this is not possible, the automation provided by the other types of IMV may be helpful.
Description of IMV(2)
IMV(2) means that mandatory breaths may be suppressed if the spontaneous breath rate is greater than the set mandatory breath rate.
Makers of home care ventilators, notably Respironics (now Philips), recognized that their patients’ comfort was an important goal. Mandatory breaths are not as comfortable as spontaneous breaths because an arbitrary preset frequency and inspiratory time are imposed on the patient. Yet mandatory breaths provide the safety net in the event of apnea. Hence, engineers invented a compromise; if the patient’s spontaneous breath rate exceeds the set mandatory breath rate, mandatory breaths would be suppressed. In practice, the machine trigger criterion is usually the absence of a patient trigger signal within the preset expiratory time, TE, determined by the set mandatory breath rate and inspiratory time, TI, where TE = (60/rate)−TI. An example would be a mode called S/T (eg, V60 ventilator made by Philips). If mandatory breaths are indeed suppressed, the ventilator waveforms look like CSV (eg, pressure support).
Rationale for IMV(2)
There are at least 38 unique mode names that are classified as IMV(2).5 Example modes on common ICU ventilators are shown in Table 3.
Safety
Two common forms of IMV(2) are called Automode on Servo ventilators and S/T on Philips/Respironics ventilators (and others). Modes with IMV(2) assure adequate gas exchange by providing a minimum MMV in the event of apnea because of the set mandatory VT and breath rate. Therefore, the goal of safety is served (in terms of gas exchange and lung protection) assuming the operator selects appropriate values for VT dosage and mandatory breath rate.
Comfort
Because spontaneous breaths are triggered and cycled by the patient, a mode comprised of spontaneous breaths is theoretically more likely to improve patient-ventilator synchrony than a mode comprised of mandatory breaths.2,22 Thus, modes with IMV(2) are more likely to promote synchrony than modes with IMV(1) because mandatory breaths may be suppressed by spontaneous breaths.6 Indeed, with adequate patient ventilatory drive, mandatory breaths may never appear. One study with noninvasive ventilation found IMV(2) to be associated with less subjects ventilatory discordance as compared to CSV in subjects with amyotrophic lateral sclerosis.41
Liberation
If weaning is thought of as increasing the proportion of spontaneous breaths relative to mandatory breaths, as in the historical justification for IMV(1), then IMV(2) is theoretically more likely to contribute to a shorter duration of weaning, other factors being equal. This is because it automatically substitutes spontaneous breaths for mandatory breaths and thus avoids any delay with manual adjustment. Roth et al6 showed that IMV(2) can be used for postoperative weaning of neurosurgical patients with healthy lungs, and compared to IMV(1), fewer manipulations of ventilator settings were necessary. Fewer manipulations may be important because manual adjustment of mandatory breath rate can be prolonged (relative to patient need), which the study showed could lead to episodes of hyperventilation and hypoventilation.
When combined with PC and adaptive targeting, IMV(2) could make an effective approach to weaning (for patients with appropriate ventilatory drive) because of the increased ability to generate spontaneous breaths with adequate VT while gradually shifting the work of breathing from the ventilator to the patient and shortening duration of ventilation.42,43 On the other hand, for patients with abnormally high ventilatory drive (eg, patients with COVID-19) the work shifting can be extreme while simultaneously allowing excessive VT dosage, working against the goals of comfort and safety. This highlights the need to understand both the type of IMV and the targeting scheme used.
Description of IMV(3)
IMV(3) means that mandatory breaths may be suppressed if the spontaneous minute ventilation is greater than the set MMV (ie, set mandatory breath rate times set VT).
There is a drawback of IMV(2); for patients with worsening lung condition (eg, ARDS), often the breath pattern becomes rapid and shallow. Hence the patient may hypo-ventilate (due to a small VT and hence large VD/VT) with spontaneous breaths while the ventilator continues to suppress the larger mandatory breaths. IMV(3) attempts to avoid this problem by suppressing mandatory breaths only if the spontaneous minute ventilation is less than the minute ventilation created by the preset mandatory breath rate and VT. An example would be a mode called mandatory minute volume (eg, V500 ventilator made by Dräger). Of course, this is only a partial solution because the settings for frequency and VT are just a guess by the clinician about the gross minute ventilation, not knowing the true alveolar minute ventilation requirement. And indeed, shallow breathing can yield a sufficient minute ventilation but insufficient minute alveolar ventilation. More advanced modes, like Intellivent-ASV (Hamilton Medical), use volumetric capnography to automatically set an appropriate minute alveolar ventilation to maintain acceptable PaCO2.
Rationale for IMV(3)
There are at least 19 unique mode names that are classified as IMV(3).5 Example modes on common ICU ventilators are shown in Table 3.
Safety
Modes with IMV(3) assure adequate gas exchange by providing a minimum MMV. For a mode like mandatory minute volume, this requires setting of acceptable values for both mandatory breath rate and VT dosage. In contrast, for modes like adaptive support ventilation (Hamilton Medical) and adaptive ventilation mode (Vyaire Medical), the operator sets a percentage of the predicted normal minute ventilation to support, and the ventilator automatically selects optimal mandatory breath rate and VT dosage based on lung mechanics.17 For these modes, it is probably impossible to distinguish the safety effects of the breath sequence, IMV(3), from the other safety features that are included in the optimal and intelligent targeting schemes they use.17,44,45
Comfort
As with modes with IMV(2), modes with IMV(3) are theoretically more likely to promote synchrony because mandatory breaths may be suppressed by spontaneous breaths.
Liberation
As with IMV(2), IMV(3) is theoretically more likely to result in shorter duration of weaning, other factors being equal. This is because the reduction of the mandatory breath rate is achieved automatically as the patient’s ability to sustain spontaneous breaths increases. IMV(3) has been shown to decrease the duration of weaning from mechanical ventilation, compared to IMV(1) or CMV.46,50 One study showed that IMV(3) reduced the duration of ventilation even compared to IMV(2).51
Description of IMV(4)
IMV(4) means that individual mandatory breaths may be suppressed due to the effects of the patient’s inspiratory efforts on trigger and cycle events. This currently may happen in two ways. In both cases, a scheduled mandatory breath (ie, machine triggered by set rate) becomes patient triggered so that the first criterion of a spontaneous breath is satisfied. In one case, a VC inspiration switches to PC due to high inspiratory effort (dual targeting) and becomes flow (patient) cycled, and hence this breath becomes spontaneous. In the second case, the mandatory inspiration was already set to be patient cycled (by flow), and hence again the mandatory breath becomes a spontaneous breath.
With IMV(4), individual, scheduled mandatory breaths may be turned into spontaneous breaths as explained above. The simplest example of this is a mode called pressure A/C with flow cycle on the Avea ventilator (Vyaire Medical). In this mode, every breath for a passive patient is pressure controlled and machine triggered (preset frequency) but flow cycled (possibly because it is a PC mode). However, if there is a sufficiently large patient inspiratory effort in the trigger window, then the delivered inflation is patient triggered and patient cycled and hence is, by definition, a spontaneous breath. This means that the mode is not CMV as the manufacturer’s name (A/C) suggests but rather IMV because spontaneous breaths may occur between mandatory breaths.
The risk of synchrony problems during conventional VC is high because the operator sets arbitrary values for VT and inspiratory flow. Hence the preset inspiratory timing rarely matches the patient’s neural inspiratory timing. Also, for a patient making an inspiratory effort, patient-ventilator synchrony will always occur because the preset inspiratory flow virtually never matches the patient’s inspiratory flow demand. If the effort is large enough, the result may be potentially dangerous work shifting. Work shifting means some portion of the inspiratory work of breathing has shifted from the ventilator (ie, under passive conditions) to the patient due to the effect of Pmus decreasing Pvent (see equation of motion for VC).22 One engineering solution is for the ventilator to recognize this condition as a drop in airway pressure and compensate by increasing inspiratory flow. This yields another, slightly more complex example of IMV(4) called VC with flow adaptation (Servo ventilators, Getinge). As required by the equation of motion, in VC, if Pmus (inspiratory effort) increases, then Pvent (airway pressure) must decrease an equal amount. Thus, the ventilator monitors Pvent; and if it drops by some default threshold (eg, 3 cm H2O), the ventilator gives as much flow (and hence volume) as the patient wants. If the effort is large enough, inspiration may also change from volume or time cycling to flow cycling. This is a form of dual targeting where VC switches to PC and the VT is larger than the preset value.20 In this case, if inspiration becomes both patient triggered and patient cycled, it is by definition a spontaneous breath that is more synchronous with the patient’s demand.
Rationale for IMV(4)
There are at least 7 unique mode names that are classified as IMV(4).5 Example modes on common ICU ventilators are shown in Table 3.
Safety
Some modes with IMV(4) are forms of VC with dual targeting. That means they start inspiration with a preset VT and inspiratory flow. As such, they assure protection from volutrauma to the extent that the operator has selected a safe VT dosage (ie, 4–8 mL/kg ideal body weight).24,26 On the other hand, with sufficient inspiratory effort, all forms of IMV(4) may allow the patient to inhale a potentially dangerous VT dosage, highlighting the need for appropriate alarms.
Comfort
As mentioned above, one mode classified as PC-IMV(4) is named pressure A/C with flow cycle on the Avea ventilator (Vyaire Medical). For this mode, every breath for a passive patient is machine triggered (preset frequency) but flow cycled and hence is a mandatory breath. However, for an active patient, if there is a sufficiently large patient inspiratory effort in the trigger window, then the delivered inflation is patient triggered and patient cycled and hence is a spontaneous breath. Flow cycling of a PC breath (as in pressure support) is a form of patient cycling because the point in time at which the flow cycle threshold is reached is a function of lung mechanics (ie, resistance, R, compliance, C, and Pmus) so that even in the absence of Pmus the time constant (the product of R and C) determines inspiratory time, which can vary randomly independent of any ventilator setting (once pressure rise time is set). This is in contrast to a mandatory breath that may be patient triggered but is time cycled by a preset inspiratory time, independent of changes in the time constant of the respiratory system. As with IMV(2) and IMV(3), substituting spontaneous breaths for mandatory breaths should increase patient-ventilator synchrony.
For modes classified as VC-IMV(4), understanding the contribution to comfort is a little more complicated. According to the equation of motion, if Pmus increases during a VC inspiration, then Pvent must decrease.22 The total work per breath remains constant, but the proportion of the work done by the patient is higher. That is, work has shifted from the ventilator to the patient.22,52 Some work shifting is tolerable, indeed, necessary, just to permit patient triggering if inspiration. Very large inspiratory efforts, as seen, for example, in some patients with COVID-19, can shift virtually all the work to the patient. Obviously, this is an uncomfortable situation for the patient. At what point between these 2 extremes of work shifting we cross the line of acceptability has not been investigated in the literature. The engineers that invented dual targeting in the form wherein a VC mandatory breath changes to a spontaneous pressure support breath have arbitrarily selected a Pvent drop of 3 cm H2O as the threshold for the switch. (There is another form of dual targeting where inspiration starts out in PC and can switch to VC2 but to serve the goal of safety, not comfort.) If you breathe on a ventilator with this mode (ie, with a mouthpiece), it is obvious that this targeting scheme is more comfortable than VC with set-point targeting because you get as much flow and volume as you wish (imagine doing this on an exercise bike). To our knowledge, there has been only one simulation-based study on this form of IMV19 and no clinical studies.
Liberation
IMV(4) may indirectly serve the goal of liberation. For a mode like pressure A/C with flow cycle, one could envision IMV(4) as contributing to the weaning process in the case of a patient with normal lungs awakening from anesthesia (ie, allowing the patient to transition to full spontaneous breathing without intervention by a clinician). But this may not be the case with other examples of IMV(4), dual targeting during VC (ie, activating flow adaptation in the mode called VC on a Servo ventilator, Getinge). This mode turns the CMV breath sequence into IMV (despite no notification of this either on the ventilator or the operator’s manual). However, the suppression of mandatory breaths in this case is a result of trying to assure comfort rather than to serve as a weaning feature. That is, making the patient work harder to get unassisted spontaneous breaths may not contribute to an ideal weaning experience.
The Future of IMV
As the title of this article indicates, our purpose is to describe the evolution of the breath sequence called IMV. The progress from IMV(1) to IMV(4) has occurred in the context of the evolution of targeting schemes from the simplest, all manual types, to the most complex using artificial intelligence (AI). Both breath sequences and targeting schemes have promoted the evolution of modes themselves. To date, arguably the most technologically advanced mode is Intellivent-ASV (Hamilton Medical).53-56 This mode of ventilation is classified as PC, IMV(3) with both optimal and intelligent targeting.2 The optimal targeting17 is designed to minimize the power transfer from the ventilator to the lungs, which may decrease the risk of ventilator-induced lung injury. (The concept of power transfer is on the cutting edge of research in mechanical ventilation.57) Intelligent targeting makes use of the tools of AI such as rule-based expert systems,58 “fuzzy logic,” and artificial neural networks.59 Naturally, as AI evolves toward human-level artificial general intelligence,60 ventilators will make increasing use of AI capabilities, resulting in modes that are more robust in the sense that they have more and more technical capabilities serving all 3 goals of ventilation.22 As we have described above, IMV is a breath sequence that serves these goals better than CMV and CSV, so logically any “ideal” mode of the future would be a form of IMV. What remains to be seen is how targeting schemes evolve. One path might be that AI controls (and learns from) the experience of large groups of ventilators united in a “network of medical things.”61
Summary
IMV is one kind of breath sequence used to classify a mode of ventilation. It has a long evolutionary history spanning over a century. There are now 4 distinct kinds of IMV, each with its own advantages and disadvantages in serving the goals of mechanical ventilation. Understanding the various forms of IMV is an important skill required for recognizing the similarities and differences among many dozens of different modes of ventilation. This recognition is essential for clinical application, education of caregivers, and research in mechanical ventilation.
Footnotes
- Correspondence: Robert L Chatburn MHHS RRT RRT-NPS FAARC. E-mail: chatbur{at}CCF.org
Mr Chatburn discloses relationships with IngMar, Vyaire, Timple, Inovytec, Aires, Ventis, Promedic, and AutoMedx. Ms Liu has disclosed no conflicts of interest.
- Copyright © 2023 by Daedalus Enterprises
REFERENCES





{kind=link}
{kind=link}
Jump to section
- Article
- Abstract
- Introduction
- History of IMV
- Evidence Supporting Different Types of IMV
- Four Types of IMV
- Description of IMV(1)
- Rationale for IMV(1)
- Description of IMV(2)
- Rationale for IMV(2)
- Description of IMV(3)
- Rationale for IMV(3)
- Description of IMV(4)
- Rationale for IMV(4)
- The Future of IMV
- Summary
- Footnotes
- REFERENCES
- Figures & Data
- Info & Metrics
- References