

Abstract
The purpose of this article is to identify (by brand name) and then classify the modes available on contemporary portable ventilators used for noninvasive ventilation in the United States. We propose a formal taxonomy that identifies the modes by their control variable, breath sequence, and targeting scheme, therefore describing what the mode does. Use of this taxonomy should be helpful in finding modes with comparable functionality that cater to the specific goal of mechanical ventilation and effective ventilatory strategies for each disease state.
Introduction
Noninvasive ventilation (NIV) has become an indispensable tool for managing acute and chronic respiratory failure. NIV involves application of positive pressure to a patient in respiratory failure using a mouthpiece, mask, or helmet interface. There are various ways that this pressure is generated, and each unique method is called a mode of ventilation (see the next section for a full explanation). Mechanical ventilation is intended to reduce the work of breathing by improving respiratory system mechanics and directly unloading the respiratory muscles. Further, positive-pressure ventilation reduces cardiac preload and afterload, particularly among patients with congestive heart failure. In the acute setting, NIV has proven efficacy in reducing mortality and the need for endotracheal intubation for patients with left-ventricular systolic heart failure1 and ventilatory failure due to COPD exacerbation.2 In the ambulatory setting, patients with neuromuscular and restrictive lung disease experience improved quality of life and survival.3 More recently, clinical benefits such as improved quality of life and hospital admission-free survival have been demonstrated for patients with COPD and chronic ventilatory failure.4,5 Reaping such benefits seems to require a specific strategy: high-intensity ventilation,6 which aims to normalize PaCO2 by using high inspiratory pressure (> 18 cm H2O), set inspiratory time (0.8–1.5 s), and a backup rate.5 To the authors’ knowledge, this is the first instance where a specific ventilatory strategy for chronic respiratory failure has produced improved clinical outcomes in the ambulatory setting, akin to low tidal volume ventilation for ARDS7 in the acute care setting. To advance specific goals of mechanical ventilation, it is imperative that ventilator modes are appropriately prescribed. In order to prescribe ventilator modes correctly, a taxonomy that allows clear comparison, communication, and teaching of the modes is necessary.
In contrast, the current terminology of noninvasive (and invasive) ventilator modes is based on manufacturer whims, like the brand names of drugs, and of little or no utility in the categorization and communication of mode function. Today’s state of chaos presents a serious obstacle to teaching, learning, and communicating noninvasive mechanical ventilation. In an era when strategies, such as high-intensity ventilation, that depend on the use of an effective ventilator mode, are proving beneficial to patients, the status quo is unacceptable.
The purpose of this article is to identify (by brand name) and then classify the modes available on contemporary portable ventilators used for NIV in the United States. Classification will be by mode taxonomy and by the Healthcare Common Procedure Coding System (HCPCS). In doing so, a key objective is to classify these modes using a formal taxonomy that has been introduced8 and refined9 over the last 2 decades.10
Ventilator Mode Taxonomy
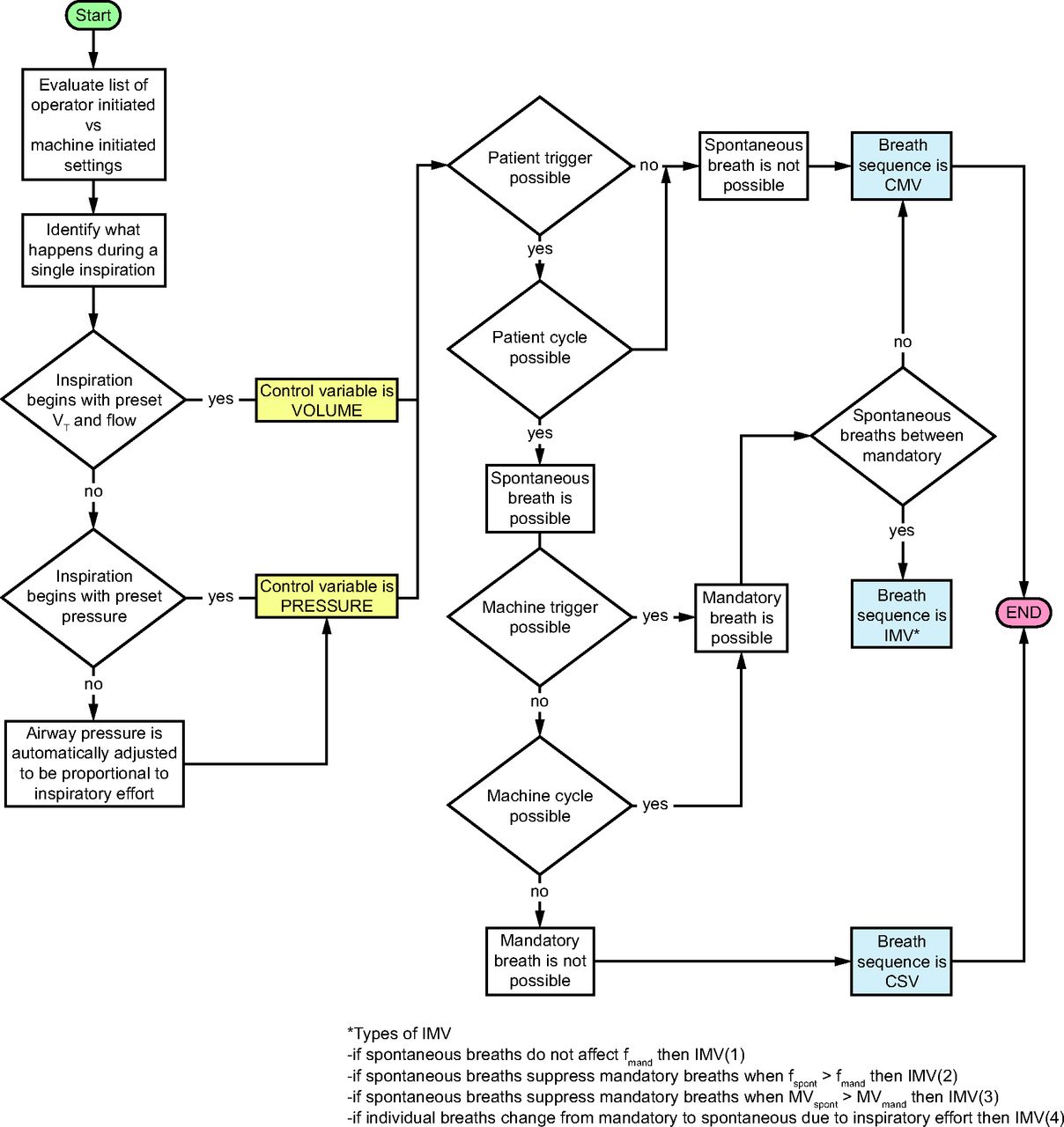
A mode of ventilation may be defined as a programmed pattern of patient-ventilator interaction. Our group has developed and described an easy-to-understand taxonomy for ventilator modes to distinguish brand names from generic classifications.8,9 Accordingly, modes are described by a combination of 3 elements: control variable, breath sequence, and targeting scheme. The control variable refers to the physical variable, either pressure or volume, the ventilator automatically adjusts (based on the equation of motion for the respiratory system). Pressure control (PC) means that either airway pressure is preset to a specific target value (eg, the mode named Pressure Support), or it is automatically adjusted to be proportional to the patient’s inspiratory effort (eg, the mode named Proportional Assist Ventilation). Volume control (VC) means that both tidal volume and inspiratory flow are preset. A breath sequence is a pattern of mandatory and/or spontaneous breaths. A mandatory breath is one for which inspiration is either triggered (started) or cycled (ended) by the machine. A spontaneous breath is one for which inspiration is both triggered and cycled by the patient. Consequently, there are 3 types of breath sequences: continuous mandatory ventilation, continuous spontaneous ventilation, and intermittent mandatory ventilation (IMV). IMV is defined as a breath sequence where spontaneous breaths may occur between mandatory breaths and can be programmed in 4 different ways.11 Finally, the targeting scheme, a key mode descriptor, describes the relationship between operator inputs and ventilator outputs to achieve a specific ventilatory pattern (generally a form of feedback control system). In this paradigm, the target is a predetermined ventilator output goal. For instance, set-point targeting refers to a scheme where all the targets are preset by the operator (as opposed to some being selected or adjusted automatically by the machine as in, for example, adaptive targeting). Ten basic maxims for understanding the mode taxonomy are summarized in Table S1 and a list of the targeting schemes is shown in Table S2 (see related supplementary materials at http://www.rcjournal.com).9 We provide a flow chart that simplifies classification of modes according to the taxonomy in Figure 1.

Flow chart for classification of modes according to taxonomy. CMV = continuous mandatory ventilation; VT = tidal volume; IMV = intermittent mandatory ventilation; CSV = continuous spontaneous ventilation; fmand = mandatory breaths; fspont = spontaneous breaths.
An example will help to illustrate the use of the mode taxonomy: the mode known by the commercial name of Bi-level S/T provides pressure-controlled breaths (preset inspiratory pressure target) that are triggered and cycled by the patient (spontaneous breaths, S) as well as pressure-controlled breaths that are triggered and cycled by the machine (mandatory or timed breaths, T). The intermittent mandatory breaths are suppressed by the spontaneous breaths if the frequency of latter is greater than the set backup rate. This scheme corresponds to the second category of IMV, designated IMV (2). Furthermore, all mandatory and spontaneous breath targets are operator set (ie, set-point targeting). Using the taxonomy, this mode is classified as PC-IMV type 2 with set-point targeting for both spontaneous and mandatory breaths, or PC-IMV (2)s,s. This brief taxonomic attribute grouping (TAG) adequately describes what the mode does and allows comparison with other modes in clinical consideration of appropriateness at the bedside. A mode TAG is like a generic name for a drug and has the same vital importance. Indeed, drug orders in electronic medical records are entered as generic TAGs, and this convention will likely spread to ventilator orders.12
A rational approach to choosing a mode of ventilation is to first assess the goal of the therapy for a particular patient at a particular point in time.13 There are only 3 basic goals: Safety (provide adequate gas exchange and protect the lungs from ventilator-induced lung injury), Comfort (maximize patient-ventilator synchrony14 and provide adequate support for work of breathing), and Liberation (minimize duration of mechanical ventilation) with the understanding that only one goal can be predominate at the point in time based on clinical assessment of the patient’s condition. Then, the most appropriate mode is the one that has the most technological features that serve the goal. These features have proliferated to the point where a single mode may serve one goal (basic mode), 2 goals (intermediate mode), or all 3 goals (advanced mode).
Classification of Modes Used for Home NIV
In order to classify ventilator modes available in the United States, we first needed to create a list of ventilators by HCPCS codes. HCPCS code definitions are provided in Table S3 in the online supplement (see related supplementary materials at http://www.rcjournal.com). To do this, we accessed a public web site called PDAC-Medicare Contractor for Pricing, Data Analysis, and Coding of HCPCS Level II DMEPOS Codes (https://www4.palmettogba.com/pdac_dmecs/searchProductClassificationResults.do?manufacturer=&codeDecision=E0471&productName=&modelNumber=&classification=&producttable_length=10, Accessed January 24, 2024). Here we were able to search the database for ventilators with specific HCPCS codes (ie, E0465, E0466, E0467, E0470, and E0471). The results for each code were exported as Excel spreadsheets. Ventilators with both E0470 and E0471 designations were converted to E0471 for simplicity. From these, we selected ventilators classified as respiratory assist device (RAD) since 2010 (Table S4, see related supplementary materials at http://www.rcjournal.com). From the operators’ manuals of these ventilators, we identified the named modes and then classified them and assigned TAGs using the ventilator mode taxonomy (described above). Next, we identified the modes with unique TAGs (Table S5, see related supplementary materials at http://www.rcjournal.com). We expanded that table by listing all the unique mode names associated with the mode TAGS (ie, several different names have the same TAG, hence the need for the taxonomy) as shown in Table 1. We repeated this procedure for ventilators classified as home mechanical ventilators (Tables S6 and S7, see related supplementary materials at http://www.rcjournal.com), which resulted in a list of unique mode names for these ventilators (Table 2).
Unique Mode Names From Respiratory Assist Device Ventilators Sorted by Mode Name
Unique Mode Names From Common Home Mechanical Ventilators Sorted by Mode Name
Summary
In this paper, we present a taxonomy of NIV modes that is based on their control variable, breath sequence, and targeting scheme. This structure allows the practitioner to manage the plethora of mode names created by ventilator manufacturers, which rarely provide a clue for what the mode actually does. By classifying modes based on these 3 aspects, one would be able to compare the actual function of a mode with another on a different device to determine if they are the same or different. For instance, Bi-Level S/T has the TAG PC-IMV (2)s, s. Modes with this TAG are available both on RADs with backup rate and home mechanical ventilators, and hence capable of providing high-intensity ventilation for the treatment of COPD with chronic ventilatory failure. Whereas there appears to be no difference in efficacy between Bi-Level S/T and other more advanced modes based on current literature,15,-,17 the mode taxonomy can offer a better understanding of the functionality of these modes and foster optimal use.
We propose that a paradigm shift in our approach to prescribing NIV is necessary. Instead of a device-based (ie, classifications of RAD or home mechanical ventilator) approach, we should adopt a therapeutic approach based on clinically effective ventilator modes for that disorder. A rational mode taxonomy provides the basis for such paradigm shift.
Footnotes
- Correspondence: Umur Hatipoğlu MD MBA, 9500 Euclid Avenue A-90, Cleveland, Ohio, 44195. E-mail: hatipou{at}ccf.org
Dr Hatipoğlu discloses a relationship with UpToDate. Mr Lewarski discloses relationships with ABM Respiratory Care, Live Fully, and the American Respiratory Care Foundation. Mr Chatburn discloses relationships with IngMar Medical, Inovytec, Timple, Aires Medical, Ventis Medical, Stimdia Medical, and the University of Cincinnati.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2024 by Daedalus Enterprises





{kind=link}