

Abstract
BACKGROUND: A universal method for determining ideal body weight (IBW) for the application of appropriate tidal volumes in children on mechanical ventilation is elusive. We sought to compare 3 commonly used IBW methods for subjects between ages 2 and 20 y.
METHODS: Demographic data were recorded, and the IBW was calculated based on the McLaren-Read, Moore, and body mass index methods by using growth chart data from the Centers for Disease Control and Prevention. The percentage error between each IBW method and the actual body weight were calculated and reported as median (interquartile range). We decided a priori that a ≥10% difference between the actual body weight and IBW would be clinically important. The Wilcoxon signed-rank test was used to compare the actual body weight with the IBW. Bland-Altman analysis was used to assess the individual agreement of each IBW method with the actual body weight. The Kruskal-Wallis test was used to detect differences among the IBW methods.
RESULTS: A total of 58 subjects (36% female) were analyzed. The median (interquartile range) percent weight error between the actual body weight and calculated the IBW was 14.8% (1.9–22.1%, P = .038), 13.8% (4.6–23.4%, P = .008), and 12.0% (3.9–20.5%, P = .037); the mean biases were 2.7 (95% CI −13.4 to 18.9) kg, 3.9 (95% CI −15.1 to 22.9) kg, 3.2 (95% CI −16.7 to 23.1) kg; and the numbers of subjects who would have a clinically important error were 29 (55.7%), 29 (56.9%), and 30 (51.7%) for the McLaren-Read, Moore, and body mass index methods, respectively.
CONCLUSIONS: The majority of the subjects demonstrated a clinically important error between the actual body weight and the IBW. The percent error increased in subjects > 25 kg actual body weight. These data underline the importance of obtaining height measurements and calculated IBW in pediatric patients who are mechanically ventilated.
- ideal body weight
- McLaren-Read
- Moore
- body mass index
- pediatric
- mechanical ventilation
- intensive care unit
- lung-protective
- growth charts
- comparative analysis
Introduction
Lung-protective ventilation strategies have been shown to reduce mortality during adult ARDS.1,2 Key components of lung-protective ventilation include the application of low tidal volumes (VT), elevated PEEP, and permissive hypercapnia.3 It is broadly understood that several factors affect normal VT, including age, sex, height, and thorax dimensions. The physiologic rationale for titrating VT to the ideal body weight (IBW) is that normal lung volumes are a function of age, sex, and thorax anatomy. Lung-protective ventilation may also be beneficial pediatric and adult in patients who do not have ARDS but receive mechanical ventilation in the ICU or operating room.4,5 Importantly, the calculation of the IBW and its use during mechanical ventilation is recommended in the pediatric ICU.6 Titration of VT relative to the IBW in the pediatric ICU is especially important because the size, height, and body composition of the population vary tremendously. However, calculation of the IBW for the titration of mechanical ventilation settings is not uniformly used.7
A universal method for determining the IBW in children on mechanical ventilation is elusive. Few studies have assessed the performance and need for IBW methods in a pediatric population.7 Therefore, we sought to compare the actual body weight with 3 commonly used methods for determining IBW in pediatric subjects: the McLaren-Read (a growth chart method), Moore (a growth chart method), and body mass index (BMI) (indexed equation based on height, sex, and age) methods.8 Further, we aimed to assess the proportion of pediatric subjects who had a clinically important difference between the IBW and actual body weight.
QUICK LOOK
Current knowledge
Using ideal body weight (IBW) to calculate tidal volumes is a common practice for adults on mechanical ventilation. However, in the realm of pediatrics, there is no clear methodology for either determining or consistently implementing an IBW calculation for appropriate tidal volumes during mechanical ventilation.
What this paper contributes to our knowledge
This study compared 3 common pediatric IBW methods to the actual body weight of pediatric subjects between the ages of 2 and 20 y. Although all 3 IBW methods yielded similar results, they also revealed a clinically important percent error from the actual body weight in more than half of the subjects analyzed. This difference was observed to increase in both frequency and scale for children who weighed > 25 kg.
Methods
Subjects
We conducted a retrospective analysis on a convenience sample of subjects between 2 and 20 years of age who were admitted to a single academic children's hospital combination medical-surgical pediatric ICU and who received invasive mechanical ventilation between July 2, 2014, and June 16, 2016. Patients with scoliosis and congenital heart disease were excluded from this study. Demographic data included age, height, weight, sex, mechanical ventilation duration, ICU length of stay, hospital length of stay, and primary diagnosis (surgical, respiratory, neurologic, sepsis, gastrointestinal, immunocompromised, or other). The study was approved by the institutional review board, and the need for informed consent was waived.
IBW Calculation
Three commonly used pediatric IBW methods were used for the subjects between the ages of 2 and 20 years. The McLaren-Read method is a growth chart method in which the IBW is determined by using the 50th percentile for weight based on height.9 The Moore method is a growth chart method in which the IBW is determined by first locating the percentile of the subject's height and then locating the respective percentile on the weight chart.10 The BMI method is an indexed equation based on height.11 The BMI IBW was calculated by using a third-degree polynomial equation derived from plotting the 50th percentile BMI versus age (months) data according to the Centers for Disease Control and Prevention 2–20 y of age chart12 and multiplied by the subject's height (m2). Simplified equations were created to automate calculations with age (months) and height (m).
Equation 1: simplified IBW from BMI in male subjects


Equation 2: simplified IBW from BMI in female subjects


Statistical Analyses
The mean differences between each IBW method and the actual body weight for all the subjects were then calculated and their respective percent error from the actual body weight was reported as median (interquartile range). Bland-Altman analysis was used to assess the individual agreement of each IBW method and the actual body weight.13 Because the data were not normally distributed, the Wilcoxon signed-rank test was used to compare the IBW with the actual body weight.14 The Kruskal-Wallis test was used to detect significant differences among the methods of IBW calculations by using the actual body weight as a reference. We decided a priori, that a ≥10% difference between the actual body weight and the IBW would be clinically important.7 Data were compiled by using MATLAB (V9.1.0.441655, Mathworks, Natick, Massachusetts), and statistical analyses were completed in Excel (V12.0 071130, Microsoft, Redmond, Washington). Prism 6.0 (GraphPad Software, La Jolla, California) was used to graph and derive the equations for the BMI IBW method and to perform the Kruskal-Wallis test.
Results
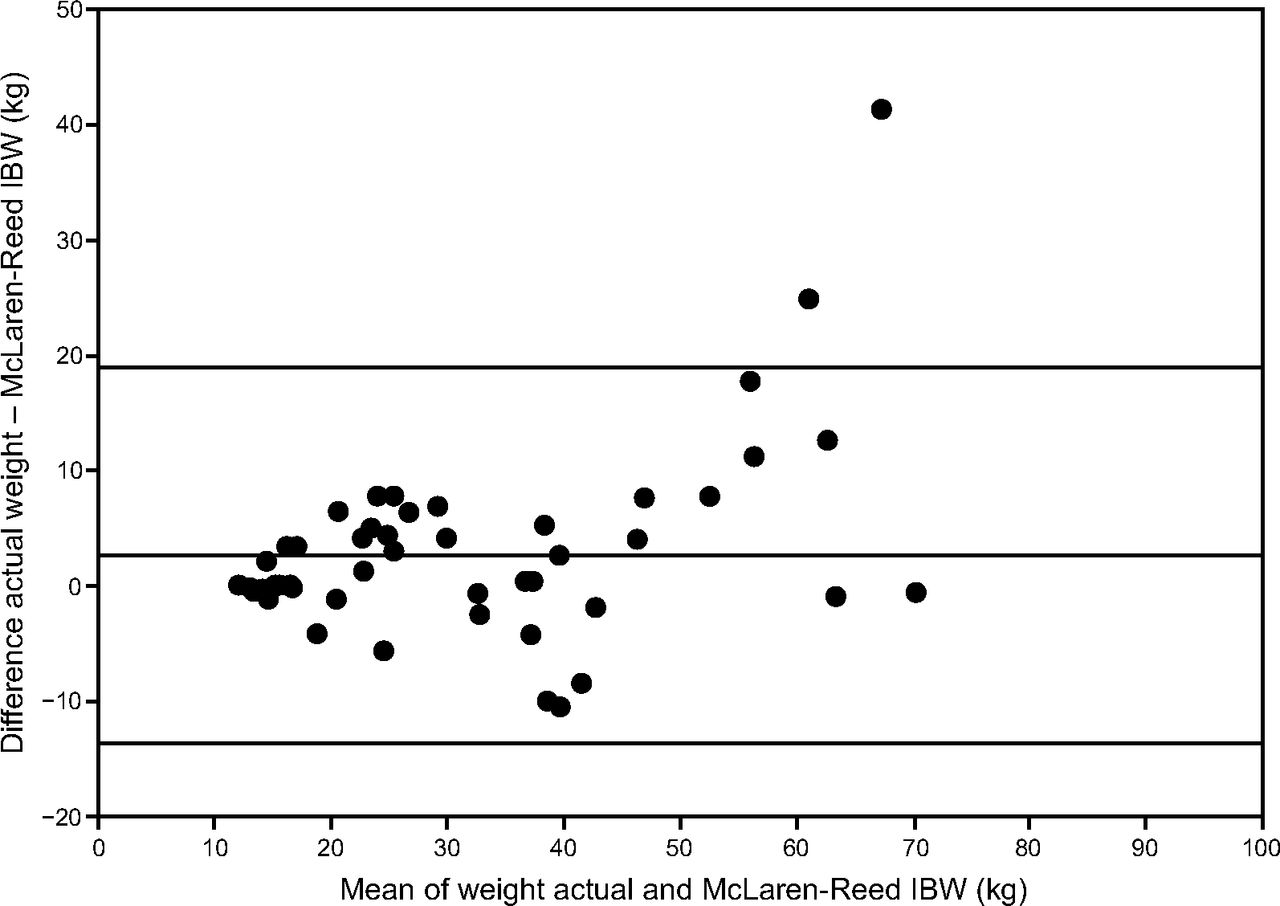
A total of 58 subjects (36% female) were analyzed. Demographic data included age, height, weight, sex, mechanical ventilation duration, ICU length of stay, hospital length of stay, primary diagnosis (surgical, respiratory, neurologic, sepsis, gastrointestinal, immunocompromised, or other) and reported as median (interquartile range) as depicted in Table 1. The median (interquartile) weight differences (%) between the actual body weight and calculated IBW was 14.8% (1.9–22.1%, P = .038), 13.8% (4.6–23.4%, P = .008), and 12.0% (3.9–20.5%, P = .037) for McLaren-Read, Moore, and BMI methods, respectively (Table 1). The numbers of subjects who would have a clinically important error were 29 (55.7%), 29 (56.9%), and 30 (51.7%) for McLaren-Read, Moore, and BMI methods, respectively (Table 1). The Kruskal-Wallis test did not detect a significant difference between the methods of IBW calculation for male or female subjects (P = .99 and P = .91, respectively). The mean biases were 2.7 (95% CI −13.4 to 18.9) kg for McLaren-Read (Fig. 1), 3.9 (95% CI −15.1 to 22.9) kg for Moore (Fig. 2), and 3.2 (95% CI −16.7 to 23.1) kg for BMI (Fig. 3). The percent error increased in subjects > 25 kg actual body weight.
Demographic, Diagnosis, and Ideal Body Weight Method Data

Bland-Altman plot for the McLaren-Read IBW method in male and female subjects ages 2–20 y. The center line denotes bias; outside lines show upper and lower limits. IBW = ideal body weight.

Bland-Altman plot for the Moore IBW method in male and female subjects ages 2–20 y. The center line denotes bias; outside lines show upper and lower limits. IBW = ideal body weight.

Bland-Altman plot for the BMI IBW method in male and female subjects ages 2–20 y. The center line denotes bias; outside lines show upper and lower limits. BMI = body mass index; IBW = ideal body weight.
Discussion
We compared 3 common IBW methods used in the pediatric population. If the actual body weight were used instead of IBW, then the majority of the patients would have a clinically important difference in applied VT. The projected error between the actual body weight and the IBW methods would similarly affect measured VT/kg in this population. Importantly, subjects with an actual body weight of >25 kg were at an increased risk for a large difference between the actual body weight and the IBW.
Martin and Richards7 defined similar percent error targets when comparing IBW models (Devine formula15) used in the 2000 ARDS Network study and the IBW relationship taken from the 1998 trial by Stewart et al16 against their synthesis of a unisex population median reference curve derived from 4 major data sources designed to produce the most-appropriate lung-protective VT. The investigators found significant weight disparities, including up to a 30% overestimation, among the referenced IBW models. Although their study did not apply these models to the actual body weight within a studied cohort, it set forth more applicable percent weight error targets of no more than 5% above and no more than 10% below the given IBW models.
The accountancy of this possible over- and underinflation of the lungs was not as well represented in our study, in which a clinically important error was presented as an absolute value of the percent error. Whereas the paucity of pediatric data has limited the ability to set such a similarly detailed lung-protective error range within this small-scale investigation, the consistent weight discrepancies should emphasize the use of the IBW for mechanically ventilated children. In the past, it has been suggested that the actual body weight be used for pediatric patients who weigh less than the 50th percentile for their age whereas the IBW predicted from the height or ulna length be used for those weighing above the 50th percentile.17 However, our data underscored the importance of the applied IBW for mechanical ventilation for all patients. The risk of volutrauma could potentially be mitigated across all populations by following a standardized approach to VT calculation.18
Although the use of the IBW in pediatric mechanical ventilation can be beneficial, there is some ambiguity about which method is preferred. In the present investigation, we noted a similar error among 3 IBW methods when compared with the actual body weight. There are some important practical differences among the methods assessed that should be considered. The BMI IBW has a greater height range and, therefore, may be applied to a broader range of patients relative to the other methods, but variables such as marginalized height and weight percentiles may interfere with this accuracy.
There are important limitations of the present study. First, the population was heterogeneous, and it was difficult to specifically note differences based on sex or other factors. However, the mix of diseases and subject sizes was generally reflective of a typical combined medical surgical pediatric ICU population. Second, the study was retrospective in nature and we, therefore, were not able to directly measure VT/kg provided. However, because the relationship between VT/kg and IBW is linear, extrapolating the error was straightforward. Third, we were unable to assess differences based on sex because the number of subjects enrolled in the study was modest. It will be important to address this feature in future work. Fourth, due to the retrospective nature of this study, we were not able to verify the height measuring technique, which is known to be difficult to accurately obtain in bedridden subjects. Fifth, the threshold for clinical importance in the present work was defined as an error of ≥10%. This threshold may be different, depending on individual practice, patient conditions, and severity of illness. Sixth, we did not detect differences among the methods of calculating IBW, but our sample size was modest, and, therefore, it is conceivable that differences could be detected in select cohorts or with a larger sample. Seventh, we did not examine the effects of IBW on VT in children < 2 y old, and extrapolation of present findings should be done with caution. It is necessary for future work to assess this population.
Conclusions
The majority of the subjects demonstrated a clinically important error between the actual body weight and the calculated IBW regardless of what IBW method was used. However, this percent error increased in subjects > 25 kg actual body weight for all 3 IBW methods. These data underline the importance of obtaining height measurements and calculated IBW in pediatric patients on mechanical ventilation. We recommend future mechanical ventilation research to clearly indicate a methodology for IBW calculations and their relationship to patient outcomes.
Footnotes
- Correspondence: Craig D Smallwood PhD RRT, Division of Critical Care Medicine, Department of Anesthesiology, Critical Care and Pain Medicine, MSICU Office, Bader 634, Boston Children's Hospital, 300 Longwood Avenue, Boston, MA 02115. E-mail: craig.smallwood{at}childrens.harvard.edu.
The authors have disclosed no conflicts of interest.
Mr Bilharz presented a version of this paper as an Editors' Choice abstract at the Open Forum of the American Association of Respiratory Care Congress, held October 4-7, 2017, in Indianapolis, Indiana.
See the Related Editorial on Page 1189
- Copyright © 2018 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}