

Abstract
OBJECTIVE: To determine the effects of different tracheotomy tube sizes on diaphragm effort and weanability indices.
METHODS: Ten tracheotomized and difficult to wean subjects were randomized to 2 T-piece trials, with different tracheotomy tube diameters: inner diameters 8 mm and 6.5 mm. Diaphragm pressure-time product per min. (PTPdi/min), lung compliance and resistance (CL and RL), breathing pattern, tension-time index of the diaphragm (TTdi), and the ratio of breathing frequency to tidal volume (f/VT) were recorded. In an in vitro model, the flow-pressure relationship was measured using the 2 tracheotomy tubes and 2 endotracheal tubes of the same diameter.
RESULTS: The use of a smaller diameter resulted in an increase of PTPdi (337.63 ± 194.35 cm H2O · s/min vs 263.28 ± 156.23 cm H2O · s/min for 6.5 mm and 8 mm, respectively, P = .004) and RL (16.74 ± 8.10 cm H2O · s/min vs 11.72 ± 7.88 cm H2O · s/min, respectively, P = .008). Both weanability indices were also significantly higher using the smaller tube: f/VT 93.32 ± 20.91 vs 77.06 ± 19.26 for 6.5 mm and 8 mm, respectively, P < .02; TTdi 0.09 ± 0.052 vs 0.08 ± 0.04, respectively, P < .02. In vitro measurements confirmed that the resistances were higher with the smaller diameter and similar between the tracheotomy tubes and the endotracheal tubes of the same diameters.
CONCLUSIONS: In tracheotomized difficult to wean subjects the decrease of the tracheotomy tube size was associated with an increased PTPdi, f/VT, and TTdi, that were otherwise normal, using a higher diameter. The in vitro study showed that the resistances increased similarly for tracheotomy tube and endotracheal tube, decreasing the diameter and increasing the flows.
Introduction
The goal of liberation from the ventilator, using a gradual reduction of pressure support or a T-piece trial, is to mimic unsupported breathing.1 The choice by a clinician to extubate the patient is mainly based on some clinical variables at the end of one of these attempts. Most of the unsuccessful attempts to free patients from mechanical ventilation are related to an impaired load/capacity balance of a respiratory pump, so that an increase in the ratio between breathing frequency and tidal volume (f/VT) is often observed.1 Lung model studies have shown that reducing the size of the endotracheal tube (ETT) is associated with an increased work of breathing.2,3 The problem of the ETT size during a spontaneous breathing trial has never been assessed; nevertheless, it may have an important influence in determining the indices of weanability directly related with the inspiratory effort, such as the f/VT ratio. The use of a tracheotomy tube with a cannula in difficult to wean patients gives us the opportunity to assess in vivo the effect of reducing the size of the tracheotomy tube and therefore assess its influence on respiratory mechanics. In a physiological trial we have studied as primary end points the diaphragm effort, respiratory mechanics, and the derivated index of weanability, during a T-piece trial using 2 different cannula sizes in stable difficult to wean patients. Indeed, as a secondary end point, in order to extrapolate the data obtained in this study with a “real life” situation in intubated patients, we have also compared the resistive properties, using the flow-pressure relationship, of the tracheotomy tubes with ETTs of the same diameter.
QUICK LOOK
Current knowledge
The resistance of artificial airways varies inversely with the internal diameter. Smaller internal diameter tubes increase the work of breathing and contribute to dynamic hyperinflation.
What this paper contributes to our knowledge
A reduction in tracheotomy tube diameter results in a significant increase of diaphragmatic effort, decrease in tidal volume, and an increase in intrinsic PEEP. During weaning the frequency to tidal volume ratio was significantly higher as internal diameter was reduced.
Methods
We evaluated 10 mechanically ventilated, tracheotomized, and difficult to wean subjects (mean age 77 ± 12 years, 7 male, 3 female) in a phase of clinical stability, defined as no fever, anxiety, hemodynamic compensation, or evident signs of respiratory distress. Three subjects were affected by COPD, 3 by post-surgical complications, and 4 by neuromuscular disease. Difficult to wean subjects were considered those who required at least 3 weeks of mechanical ventilation, with at least 3 disconnections from the ventilator attempts, and consequently they were tracheotomized.1 The subjects' clinical features and ventilatory settings are shown on Table 1.
Clinical Features and Ventilator Settings
The study was approved by our institutional ethical committee, and written informed consent was given by all the subjects.
In Vivo Measurements
One hour after having changed their cannula with a new one of the same diameter (Portex, inner diameter [ID] 8 mm, cannula ID 6.5 mm, Blue Line Ultra, Smiths Medical, Watford, United Kingdom) the subjects were disconnected from the ventilator and breathed spontaneously through a T-tube circuit for 30 min, using 2 different tube sizes (using or not the cannula, so that the actual inner diameter was 8 mm or 6.5 mm, respectively). The T-tube circuit was kept constant for all the experiments, no humidification system was used. After that period they were briefly reconnected (30 min) to the ventilator, and thereafter the second trial was initiated. The order of the trial (ie, with or without the cannula, 6.5 mm and 8 mm) was randomized using a computer generated sequence, controlling, however, that the initial trial was homogeneously distributed (ie, 5 subjects initiated the experimental procedure with a 6.5 mm and 5 with an 8.0 mm).
The subjects were studied in a semirecumbent position, and oxygen therapy was administered to get an SaO2 of > 92%. Blood pressure, electrocardiogram, and pulse oximetry were continuously recorded during the experimental trial.
Flow at the airway opening was measured with a heated pneumotachograph (3700, Hans Rudolph, Shawnee, Kansas) and a differential pressure transducer (Honeywell, ± 300 cm H2O, Freeport, Illinois) placed at the end of the tracheotomy tube. VT was obtained by integration of the flow. Inspiratory time, expiratory time, total respiratory time, and frequency were measured from the flow signal.
Changes in esophageal and gastric pressures were measured using the balloon-catheter technique4: both esophageal and gastric pressures were measured with 2 balloon-tipped catheter systems connected to 2 differential pressure transducers (Honeywell, ± 300 cm H2O, Freeport, Illinois), and another monitoring line with a pressure transducer was used to sample the pressure at the airway opening, between the tracheotomy tube and the pneumotachograph. The subtraction of esophageal pressure from gastric pressure gave the measurement of transdiaphragmatic pressure (Pdi), while the subtraction of esophageal pressure from the pressure at the airway opening gave the value of transpulmonary pressure. The proper position of the esophageal balloon was verified using the occlusion test.5
Dynamic lung compliance was obtained from simultaneous recordings of transpulmonary pressure, VT, and flow, and calculated as the ratio of change in volume to change in transpulmonary pressure between instants of zero flow within the same breath.
Inspiratory pulmonary resistance was calculated by fitting the equation of motion of a single-compartment model using multilinear regression, according to the Neergaard-Wirtz elastic subtraction technique,6 while intrinsic PEEP was calculated from the change in Pdi preceding flow, as described elsewhere.7 Changes in the magnitude of the diaphragm effort were estimated from changes in the pressure-time product (PTPdi). The PTPdi was obtained by measuring the area under the Pdi-versus-time curve per breath, and for a period of 1 min.8 We used the PTPdi as an index of inspiratory muscle energy expenditure, as it has been shown to be correlated with the oxygen consumption of the respiratory muscles.9
Physiological signals were collected for 5 min at the end of the spontaneous breathing trial. To measure the maximum transdiaphragmatic pressure (Pdi-max) we inserted at the tip of tracheotomy tube a device consisting of a rigid T-tube with a unidirectional valve set on the expiratory line. Measurements were repeated 5 times, and the best value was considered for data analysis.
The tension-time index of the diaphragm (TTdi) was computed using Pdi-max, according to the method of Bellemare and Grassino10:
In Vitro Measurements
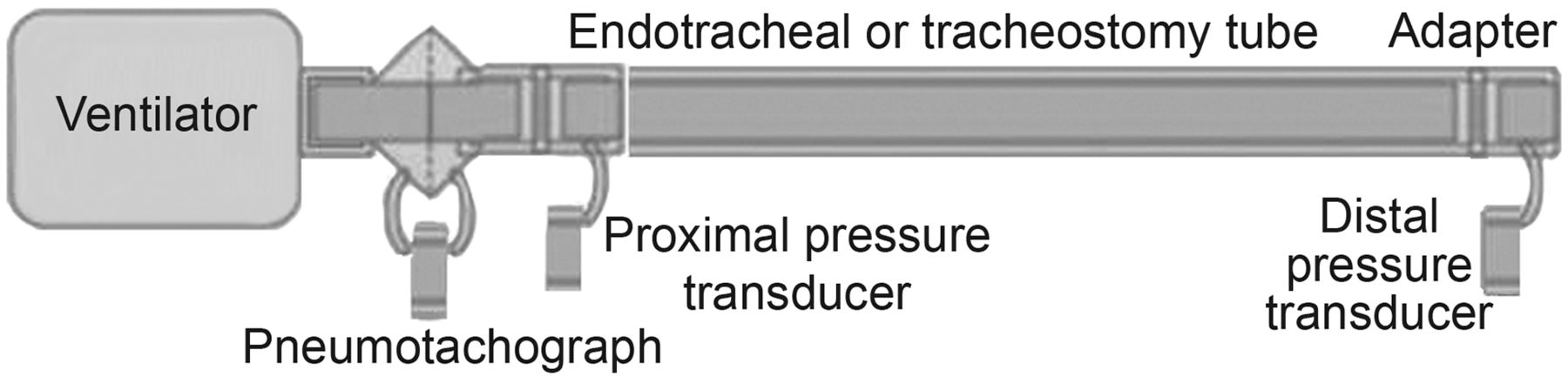
The actual ID of the tracheotomy tubes with and without the cannula, as well as that of the ETTs of the same diameter (Portex Blue line profile soft-seal oronasal cuff ID 8 mm and 6.5 mm) and length, was measured by volumetric water displacement method, as described elsewhere.11 ETTs with and without the cannula and with the different resistances were measured by using the setup shown in Figure 1. Pressure drop was measured with a distal differential pressure transducer (DP, ± 35 cm H2O, Validyne, Northridge, California) with one port opened to the atmosphere, and positioned with an adapter of the same size as the sampled tube at the end of the tracheotomy tube or of the ETT. A second differential pressure transducer (DP, ± 2 cm H2O, Validyne, Northridge, California), coupled with a pneumotachograph (Fleisch 1, Gould Electronics, Eichstetten, Germany) was positioned between the ventilator outlet and the sample tube. Flow was delivered using controlled, volume targeted mechanical ventilation, with a square waveform, at 0.3, 0.6, 0.8 and 1 L/s.
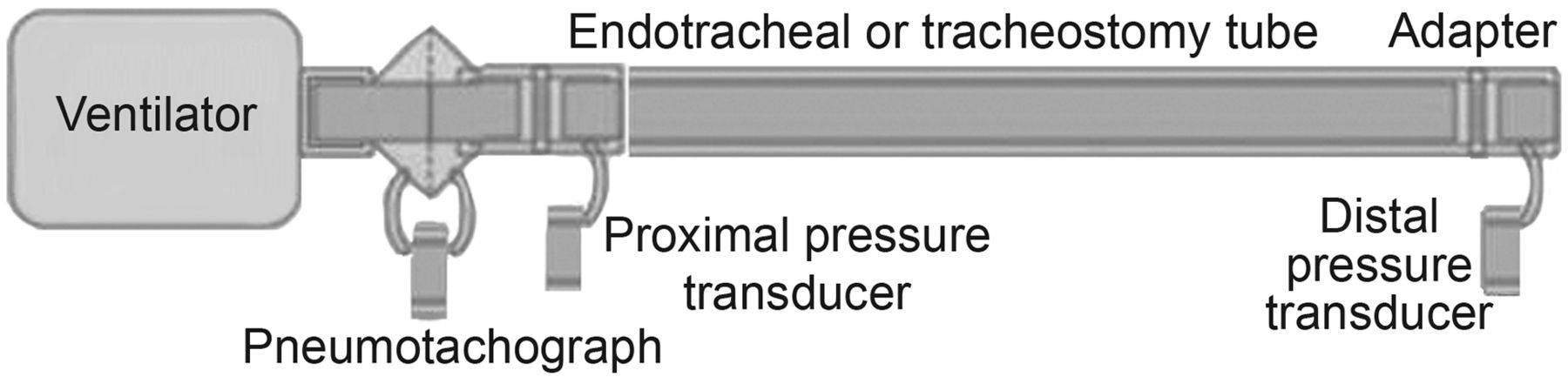
The experimental setup used in vitro to measure the pressure-flow relationship through endotracheal and tracheotomy tubes.
Statistical Analysis
Data are expressed as mean ± SD. Considering the primary outcome, reduction in PTPdi, we expected an ∼ 40% reduction in the 8.0 mm group, based on the frequencies reported in a previous physiological trial performed in vitro,3 considering work of breathing, using a VT of 600 mL and a maximum inspiratory flow of 157 mL/s. Thus, given a power of 80% with an α error of 5%, to detect the expected difference of > 30% between the 2 groups in the PTPdi, we had to enroll a total of 10 subjects. A paired sample test was used for statistical analysis.
A P value < .05 was considered statistically significant. All the analyses were performed using statistics software (Statistica/W, StatSoft, Tulsa, Oklahoma).
Results
Reasons for T-piece trial failure days before the experimental procedures were: f/VT > 100 (n = 5), increase of PaCO2 > 15 mm Hg at the end of 60 min trial (n = 3), agitation and diaphoresis (n = 1), inability to clear secretions (n = 1). All the subjects tolerated well the experimental study.
Inspiratory Effort and Respiratory Mechanics
As shown on Table 2, the reduction of the tracheotomy tube resulted in a marked and significant increased of the diaphragmatic effort and a concomitant augmentation of lung resistance and in dynamic intrinsic PEEP, while lung compliance did not significantly change.
Physiological Variables at the End of the T-Piece Trial Using 2 Different Tracheal Tube Sizes
Breathing Pattern
A significant reduction in VT was observed with the decrease of the tracheotomy tube size (see Table 2), while breathing frequency remained unchanged.
Index of Weanability
Figure 2 upper part shows the reduction of f/VT index after up-sizing the diameter of the tube. The subjects during the trial with a smaller tube had a significantly higher index, compared to the trial with a larger tube (f/VT 93.32 ± 20.91 vs 77.06 ± 19.26 for 6.5 mm and 8 mm, respectively, P < .02).

Individual values for the ratio of breathing frequency (f) to tidal volume (VT) and tension-time index of the diaphragm (TTdi) with tracheotomy tubes of 6.5 and 8 mm inner diameter. Note the overlap of data in 2 subjects.
Figure 2 lower part illustrates data of TTdi, which were significantly lower with a larger diameter (TTdi 0.09 ± 0.052 vs 0.08 ± 0.04, respectively, P < .02). At hospital discharge 6/10 subjects were finally liberated from the ventilator.
In Vitro Measurements
The actual diameters for both tracheotomy and ETTs measured by volumetric water displacement were almost identical between the one estimated by the manufacturers and those recorded in the study: tracheotomy tube 8 mm = 7.9 mm, tracheotomy tube cannula 6.5 mm = 6.3 mm, ETT 8 mm = 8.1 mm, and ETT 6.5 mm = 6.6 mm. Resistances with different tubes and flow are shown in Table 3. A marked increase in the resistive properties was found with increasing the flow and decreasing the diameter of the tubes, irrespective of the type of tube used.
Resistances With Different Tubes and Flow Measured In Vitro
Discussion
In this study we have assessed for the first time the effects of different tracheotomy tube sizes on the subject's inspiratory effort and indices of weanability. We have found that decreasing the inner diameter of the tube increased the diaphragm energy expenditure, due to the marked increase in pulmonary resistance, and that the load/capacity balance (Pdi/Pdi-max) also worsened, so that f/VT was approaching, and in some individuals overpassed, the “weanability threshold” of 120.1 Indeed the in vitro study showed that the resistances increased similarly for tracheotomy tubes and the ETTs, decreasing the diameter and increasing the flow.
The concept that a smaller inner diameter may induce an increased work of breathing has been known for a long time, as well as the concept that the in vivo resistance of ETTs exceeds the in vitro resistance, because of the presence of secretions. For example Wilson et al12 examined tubes removed from extubated patients, finding that secretions adhering to the inner lumen of the these tubes led to significant luminal narrowing (eg, 15% of tubes behaved like tubes that were 3 sizes smaller than the inserted tube.) The accompanying editorial by Vassilakopoulos13 noted how this can lead to rapid shallow breathing. There were similar findings by Epstein et al,14 reporting that patients with ETTs of 7 mm or smaller had a higher f/VT than patients with > 7 mm tubes. Mehta et al15 conducted a physiologic study of patients ready to be extubated, showing those with 7–7.5 mm tubes had higher respiratory rate, lower VT, higher f/VT, and higher PTP, compared to those with 8 mm tubes (during T-piece, CPAP, and pressure support ventilation). Lastly, Banner et al16 demonstrated the clinical relevance of “iatrogenic” weaning failure by showing that the work of breathing imposed by the ETT can be associated with significant tachypnea during weaning trials on CPAP.
Weissman17 evaluated flow-volume loops in postoperative patients intubated with 2 different tube sizes (7 and 8 mm) and found that only minimal limitation to air flow occurred at volumes and frequencies associated with tidal breathing. This study, despite not providing a direct calculation of the diaphragm effort and of the weanability indices, is nevertheless important, because it highlights the idea that the tube resistance may not be important when the appropriate size is chosen.
Several authors have suggested that the “minimal” ideal size of the tube is 7 mm, but on the other side it has been shown that the “final” size at the time of extubation is lower than this threshold in more than 20% of the patients.18 A particularly interesting finding was that this obstruction was documented within 24 hours of intubation, and this may represent an unsuspected difficulty in liberation of patients from mechanical ventilation and a forgotten complication of prolonged mechanical ventilation.
Similar data were also reported by Villafane et al,19 in patients requiring mechanical ventilation > 24 hours, where significant alterations in the inner tube diameter were observed, especially when using a hydrophobic heat and moisture exchanger to humidify the airways.
When the flow is generated at the entrance of the tube, the pressure drop in the tube, for a given flow, is proportional to the length, and, more interesting for this study, inversely proportional to the diameter to the power of 4.75.11 This means that, for the same length, when the diameter decreases from 8 mm to 6.5 mm, the pressure drop is multiplied by 8 to the power 4.75 and divided by 6.5 to the power 4.75,19 which may well explain the 45% increase in the resistances observed in this study. Indeed, inside the tube the laminar flow may switch to turbulent flow, where the flow is associated with nonlinear pressure-flow relationships that are gas-density dependent. The flow-dependent shift from laminar to turbulent flow is captured in the Rohrer equation.20
Despite numerous other studies suggesting that tube resistance may represent a significant impediment to spontaneous breathing,2,3 few other authors have demonstrated the relationship between narrow tube size and increased f/VT.14,15 The present investigation is one of the few that showed in vivo that not only may the PTPdi be abnormally increased by reducing the inner diameter, but also that the breathing pattern may be altered. As a matter of fact, all our subjects reduced VT, keeping breathing frequency unchanged, so that the f/VT index was significantly altered. This suggests in some subjects (n = 5) the impossibility of being liberated from mechanical ventilation; however, this index did return to normal values after increasing the tube diameter. What distinguishes the current study from others is that each subject was able to act as their own control, thus minimizing confounding variables that may have influenced the findings in the previous ones. Weissman et al,21 in a group of normal subjects and patients undergoing surgery and breathing through a mouthpiece with various resistances, reported a higher VT and reduced breathing frequency using the smaller diameter. These differences may be well explained by the fact that our subjects were considered difficult to liberate from mechanical ventilation and that, due to the nature of their disease, the maximal diaphragmatic pressure was markedly reduced. The impaired load/capacity balance of the respiratory pump may well explain the adoption of a breathing pattern characterized by an attempt to minimize the energy expenditure by decreasing VT.22 The data obtained in this study may not be applied in real life situations, where the large majority of trials to liberate patients from mechanical ventilation are performed in intubated patients. Indeed most of the patients nowadays are intubated using quite large diameter tubes (ie ≥ 8 mm), but as Wilson et al12 showed in their study, large diameter tubes frequently have reduced caliber in vivo because of accumulation of secretions. The results of our in vitro study, however, showed a rather surprising similarity in the resistive properties of the tracheotomy tube and ETT, which are characterized by different length and curvature, suggesting that an extrapolation of our data for the “usual” practice to rid patients from mechanical ventilation may be possible. If we consider specifically the problem of tracheotomized patients, our results may instead be useful to decide not only if a patient cannot tolerate an unsupported breathing trial, simply because of a small tube diameter, but also when the objective is to get the patient freed from the tracheotomy. In the subset of tracheotomized patients, however, it may be worth mentioning that the use of a larger tube may increase the risks of complications, such as difficult phonation and swallowing function and also damage of the airways.
One potential criticism of our study is that the data were collected in tracheotomized subjects and therefore may not represent the real life situation of intubated patients. Few studies have shown that the work of breathing is significantly reduced after tracheotomy, but the clinical importance of these effects is questioned.23,24 As a matter of fact, the presence of the ETT may exaggerate even more the dependence of the indices of weanability on the size of tube, emphasizing the concept of using a “clean” tube with a diameter ≥ 7 mm.
Conclusions
In conclusion, we have shown that the energy expenditure of the diaphragm is markedly increased when reducing the size of the artificial airways, mainly due to the augmented resistive component. In difficult to wean patients this may lead to a breathing pattern that may alter some indices of weanability that are otherwise normal using a greater tube diameter.
Footnotes
- Correspondence: Stefano Nava MD, Pneumologia e Terapia Intensiva Respiratoria, Azienda Opedaliera Universitaria Sant Orsola-Malpighi, via Massarenti no. 9, Bologna 40138 Italy. E-mail: stefano.nava{at}aosp.bo.it.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 2130
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}