

Abstract
BACKGROUND: Tubing systems are an essential component of the ventilation circuit, connecting the ventilator to the patient's airways. Coaxial tubing systems incorporate the inspiratory tube within the lumen of the expiratory one. We hypothesized that by design, these tubing systems increase resistance to air flow compared with conventional ones.
METHODS: We investigated the flow-dependent pressure gradient across coaxial, conventional disposable, and conventional reusable tubing systems from 3 different manufacturers. Additionally, the additional work of breathing and perception of resistance during breathing through the different devices were determined in 18 healthy volunteers.
RESULTS: The pressure gradient across coaxial tubing systems was up to 6 times higher compared with conventional ones (1.90 ± 0.03 cm H2O vs 0.34 ± 0.01 cm H2O, P < .001) and was higher during expiration compared with inspiration (P < .001). Additional work of breathing and perceived breathing resistance were highest in coaxial tubing systems, accordingly.
CONCLUSIONS: Our findings suggest that the use of coaxial tubing systems should be carefully considered with respect to their increased resistance.
- mechanical ventilation
- devices/equipment
- development and evaluation/technology assessment
- artificial airways
- breathing system
- airway resistance
- work of breathing
Introduction
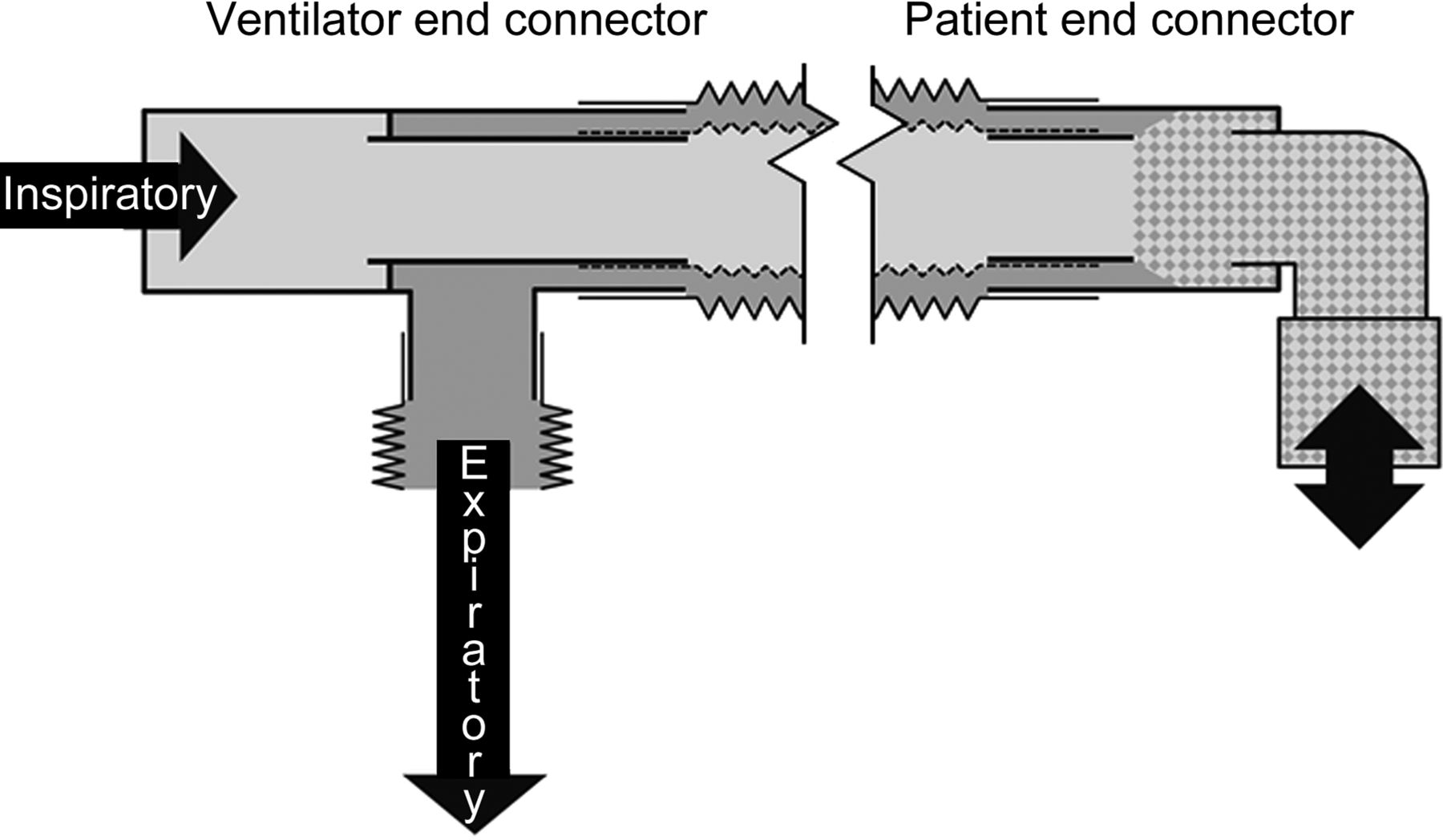
During mechanical ventilation, the tubing system links the ventilator to the patient's secured airways. Conventionally, 2 silicone tubes separate inspiratory and expiratory flow. Over the past years, disposable plastic tubes have been used increasingly, to cope with the growing demands on hygiene and cost/value ratio. Coaxial tubing systems incorporate the inspiratory tube inside the lumen of the expiratory tube (Fig. 1). Coaxial tubing systems may provide facilitated handling during anesthesia and gas temperature exchange across the inner laying surface.1 However, little is known about the resistive behavior of such tubing systems. Studies investigating other components of the artificial airways found the cross-sectional area to be the most relevant determinate for the components' resistance to air flow.2,3 Considering these findings, coaxial tubing systems may increase resistance to air flow, because their design is at the expense of the lumina's cross-sectional area.

Technical scheme of coaxial tubing systems, given for 2 different sections. At the tubing's ventilator end, a rigid T-piece connector enables inspiratory (light gray area) and expiratory gas flow (dark gray area) to pass each other. At the patient end, the inspiratory lumen ends freely within the expiratory lumen, thereby mixing the gas flow (shaded area). Please note that the inspiratory tube, which is lying on the inside, is held in position at the ends only.
We hypothesized that resistance, additional work of breathing, and perceived breathing resistance are higher in coaxial tubing systems compared with conventional ones. Therefore, we quantified the pressure-flow characteristics of coaxial and conventional disposable or reusable tubing systems from 3 different manufacturers. Furthermore, additional work of breathing and perception of breathing resistance were determined in healthy volunteers.
QUICK LOOK
Current knowledge
All components of artificial airways contribute to artificial airway resistance, mainly depending on the inner diameter and the length of the respective device as well as on the present flow. Significant contribution to airway resistance has been shown for endotracheal and tracheostomy tubes but also for heat and moisture exchangers and humidifiers. High artificial airway resistance prolongs expiration time during controlled ventilation and increases the patient's work of breathing during spontaneous breathing. Therefore, artificial airway resistance should be as low as possible.
What this paper contributes to our knowledge
This study compared the resistances of recently introduced coaxial tubing systems (consisting of 2 interleaved tubes) with conventional tubing systems (consisting of 2 separate tubes) of a disposable or reusable type. Coaxial tubing systems exhibited a significant higher flow-dependent pressure gradient, particularly in expiration, when compared with conventional ones. Similarly coaxial tubing systems increased work of breathing to a relevant extent. Coaxial tubing systems should be carefully applied with regard to their increased resistance.
Methods
Coaxial tubing systems and conventional disposable tubing systems (including a Y-piece and a 90° connector) from 3 different manufacturers (Dräger Medical, Lübeck, Germany; Medisize, Siegburg, Germany; and Covidien, Neustadt/Donau, Germany, respectively) were investigated. As a reference, we additionally investigated a conventional reusable tubing system composed of 2 silicone breathing tubes, a Y-piece, and a 90° connector (all from VBM Medizintechnik GmbH, Sulz am Neckar, Germany). Types, full lengths, and cross-sectional areas of the tubing systems are specified in Table 1.
Specifications of Tubing Systems
Pressure-Flow Characteristics
Pressure-flow characteristics were measured by streaming the tube under test with a defined gas flow (Fig. 2). To generate a reproducible curvature of the respective tube, it was mounted with a defined sagging of 33% of its total length. When applicable, foldable tubes were measured at their full lengths (Table 1). To cover a clinically relevant flow range, the model was streamed with a sinusoidal flow of ±1.2 L/s using a piston pump driven by a control unit (E1100, LinMot, Spreitenbach, Switzerland). Flow (V̇) was measured using a pneumotachograph (Fleisch 2, Dr Fenyves & Gut, Hechingen, Germany) connected to a differential pressure transducer (CP 100, Hoffrichter, Schwerin, Germany). Airway pressures were measured at both ends of the respective tubing system using piezoresistive pressure transducers (Type 4, SI-Special Instruments GmbH, Nördlingen, Germany). Proximal and distal pressure measuring sites were of identical inner diameter to prevent the Bernoulli effect from influencing the measurements. All instruments were calibrated daily before the beginning of the experiments, after interruption of an experiment exceeding 1 h, or after a visible offset in baseline values.
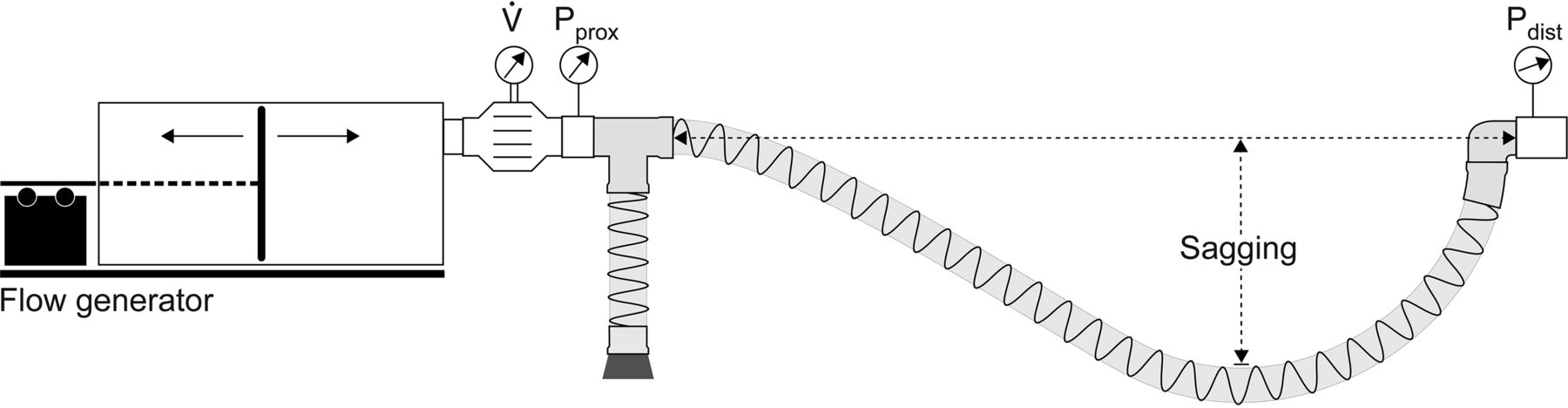
Flow model, exemplarily shown for measurements across the inspiratory lumen of a coaxial tubing system. Sinusoidal flow was applied using a piston pump driven by a linear motor (Flow generator). Flow (V̇) was measured at the tubing system's ventilator end. Airway pressures were measured at the proximal (Pprox) and the distal end (Pdist) of the tubing system. Please note that the tube's sagging was standardized to 33% of the total length.
We calculated the flow-dependent pressure gradient across the tubing systems (ΔP) by means of Rohrer's approach,2 reflecting originally a linear and a quadratic relation between flow and pressure gradient. In preliminary experiments, we found that in tubing systems, the linear term does not contribute to ΔP to any relevant extent. Therefore, we used a simplified equation containing only the coefficient of the quadratic flow term (K2) and inertance (I).3
 (1)
(1)
From the continuously measured ΔP, flow, and derived volume acceleration (V̈), K2 and inertance I were determined for each tubing system by linear regression of Equation 1. For easier comparison between the different tubing systems, ΔP was calculated for an exemplary flow of 600 mL/s (ΔP600).
All measurements were performed for each lumen separately and repeated 6 times after dismantling and reassembling of the model setup. Flow and pressure signals were sampled at a rate of 200 Hz. Twelve ventilation cycles were recorded for each condition.
Additional Work of Breathing
To quantify the tubing systems' load for a patient, we determined the additional work of breathing caused by the tubing systems during quiet breathing. In addition, to investigate whether differences in breathing resistance between the different tubing systems would be of clinical relevance, we evaluated the perception of tubing resistance in healthy volunteers when breathing via the different types of tubing systems. The study was approved by the ethics committee of the University of Freiburg, and written informed consent was obtained by each volunteer before the experiments. Eighteen volunteers (female, n = 5; male, n = 13; age, mean [range] 37 y [24–62 y]; weight, mean [range] 76 kg [54–125 kg]; height, mean [range] 176 cm [162–192 cm]) with no known history of lung disease were asked to breathe via a mouthpiece through a pneumotachograph (as above). Initially, 20 quiet breaths were taken in a sitting position without any tubing attached to the measurement system.
To eliminate effects of breathing variability during the different trials and to prevent adaptation of the breathing pattern in response to the current load, additional work of breathing (WOB) was calculated instead of directly measured. Additional WOB was calculated from the data measured during the subjects' quiet breathing (without tubing) by integrating the product of ΔP and V̇ over the time (t) of 1 min.4
 (2)
(2)
For that purpose, ΔP was calculated from the measured flow and the previously determined respective K2 and I, following Equation 1. Additional WOB/L of ventilation was calculated by dividing additional WOB by minute ventilation.5
Perceived Breathing Resistance
After the initial measurement, a conventional, a disposable, and a coaxial tubing system (the latter two from Dräger Medical) were attached successively to the measuring system, and the volunteers were asked to take another 20 breaths through each device, respectively. To achieve directed flow within the tubing systems, their ends were connected to passive inspiration and expiration valves (resistance < 0.7 cm H2O × s/L at 1.0 L/s). The tubing systems were presented in randomized order, blinded to the volunteers who were given a 1-min rest between 2 consecutive tests. Subsequently, the volunteers were asked to specify the one tubing system they had perceived to provide the highest breathing resistance, respectively.
Statistical Analysis
Data are presented as means ± SD if not indicated otherwise. Pressure and flow measurements were recorded using LabView 7.1 (National Instruments, Austin, Texas) and analyzed using MATLAB 2014.R1 (The MathWorks, Natick, Massachusetts). For comparisons of ΔP600, ordinary one-way analysis of variance was calculated, followed by Sidak post hoc tests if appropriate (GraphPad PRISM 6.02, GraphPad Software, La Jolla, California). The number of volunteers was calculated in an a priori power analysis based on a chi-square test. From our experimental findings, we expected a very large effect size of 0.75. Under this assumption, 18 subjects were required to achieve a power of 0.8 for identifying a difference in breathing resistance between the 3 types of tubing systems. For comparison of additional WOB, one-way analysis of variance was calculated, followed by the Dunnett multiple-comparisons test. The ratings for breathing resistance were compared using the Kruskal-Wallis test, followed by Dunn tests. A P value < .05 was considered significant.
Results
Pressure-Flow Characteristics
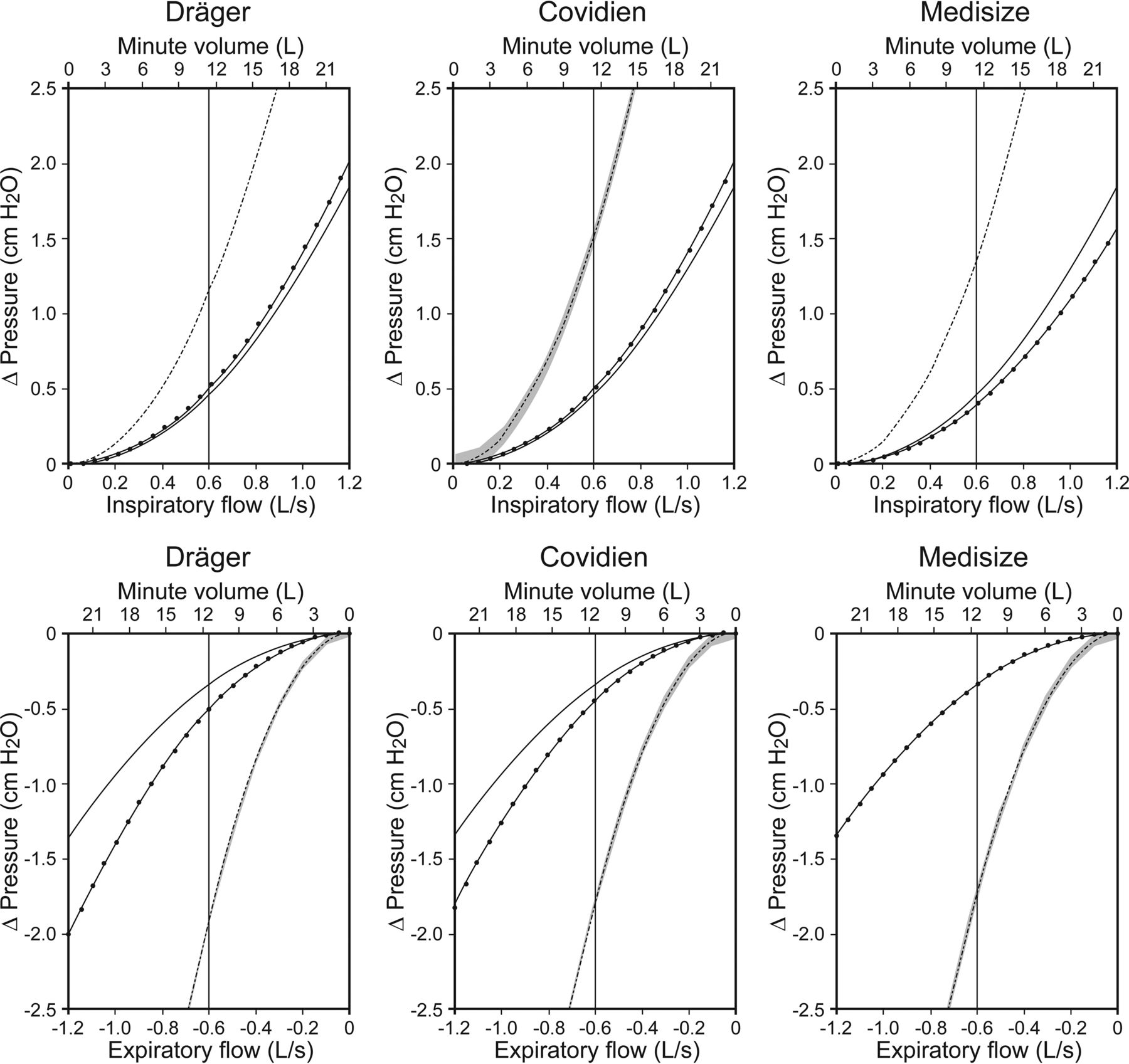
Measured pressure gradients were nonlinearly flow-dependent across all devices, increasing disproportionally with increasing flow. Derived resistive coefficients K2 differed between the investigated tubing systems (Table 2). The coaxial tubing systems showed the highest K2 values, whereas the conventional reusable tubing system exhibited the lowest ones. The pressure-flow characteristics varied considerably between the different types of tubing systems. ΔP of coaxial tubing systems exceeded considerably ΔP of conventional tubing systems (Fig. 3). ΔP was comparable during inspiration and expiration in conventional tubing systems but higher during expiration than during inspiration in all coaxial tubing systems (Fig. 3). Among coaxial tubing systems, those of Covidien showed the highest whereas those of Dräger showed the lowest ΔP during inspiration. Those of Dräger showed the highest and those of Medisize showed the lowest ΔP during expiration. ΔP600 of the coaxial tubing systems amounted up to 1.90 ± 0.03 cm H2O, whereas it was < 0.51 ± 0.01 cm H2O (disposable) and < 0.34 ± 0.01 cm H2O (reusable) in conventional tubing systems (P < .001). Among conventional disposable tubing systems, ΔP600 was lower in Medisize (0.40 ± 0.01 cm H2O, P < .001) compared with Covidien (0.51 ± 0.01 cm H2O) and Dräger (0.51 ± 0.01 cm H2O). Inertance was <0.17 cm H2O × s2/L in all devices (Table 2).
Rohrer Coefficient K2, Inertance, and Compliance of Tubing Systems

Flow-depending pressure gradients (ΔP) across coaxial tubing systems (dashed lines), conventional disposable tubing systems (dotted lines), and a conventional reusable tubing system (solid lines). Curves were calculated from the respective resistance coefficients for the displayed flow range separately for inspiratory flow and expiratory flow and 3 different manufacturers. Gray areas represent SD. The Medisize conventional disposable and reusable tubing systems showed identical progression curves during expiration. Minute volume with peak flow corresponding to flow mentioned in the scale above, assuming a sinusoidal flow profile.
Additional Work of Breathing and Perceived Breathing Resistance
Different types of tubing systems caused significantly different amounts of additional WOB (Fig. 4). Mean additional WOB accounted for up to 3.5 ± 1.7 J/min in coaxial but only 1.0 ± 0.5 and 0.8 ± 0.4 J/min in disposable and reusable conventional tubing systems, respectively (P < .001). Additional WOB/L caused by the coaxial tubing systems amounted up to 0.3 ± 0.1 J/L and was significantly higher (P < .001) compared with the conventional disposable and reusable ones (Fig. 4). Mean (range) tidal volume was 1.1 L (0.4–2.3 L); mean (range) breathing frequency was 13 breaths/min (8–20 breaths/min).

Comparison of additional work of breathing (WOB) (A) and additional WOB/L of ventilation (B) across the different types of tubing systems (conventional reusable, conventional disposable, and coaxial tubing system) and different manufacturers. Boxes show interquartile range, horizontal lines denote medians, and whiskers show the minima and maxima. * P < .001 versus conventional reusable and disposable tubing systems.
Rating of breathing resistance depended on the tubing system used. Of the 18 volunteers, 13 rated breathing resistance of the coaxial tubing system the highest compared with conventional reusable and disposable tubing systems (both P < .001). The perception of breathing resistance with conventional reusable and conventional disposable tubing systems did not differ significantly (P = .40).
Discussion
The main findings of the present study can be summarized as follows: (1) coaxial tubing systems exhibit a remarkably higher flow-dependent pressure gradient compared with conventional tubing systems; (2) in spontaneously breathing volunteers, additional work of breathing is highest with coaxial tubing systems; and (3) the breathing resistance was perceived to be highest in coaxial tubing systems.
This study confirms our hypothesis that the flow-dependent resistance of new coaxial tubing systems is substantially higher compared with systems composed of 2 separate tubes. The coaxial systems' disproportionally high resistance may be caused by their geometry. It is well known that the cross-sectional area determines a tube's resistance.6 Typically, the endotracheal tube represents the narrowest component of the artificial airways and hence the highest resistance to air flow. Accordingly, the pressure-flow characteristics of endotracheal tubes have been studied extensively, and Rohrer's equation has been well evaluated in this regard.2,7 By contrast, breathing tubes have relatively large cross-sectional areas; therefore, one would expect only marginal contribution to artificial airway resistance. Our results, however, demonstrate that this is only true for conventional tubing systems and particularly not for coaxial ones. Integration of the inspiratory lumen into the expiratory one in coaxial tubing systems is at the expense of both luminal sectional areas. Whereas the sectional areas of conventional tubing systems comply with the ISO standard of a 22-mm inner diameter, the net sectional area of coaxial systems is considerably lower, only an approximately 16-mm diameter. Despite marginal differences, this was comparable among all manufacturers. As a consequence, the coaxial tubes caused about two thirds of the resistance of an endotracheal tube with an 8.0-mm inner diameter.2
In our study, coaxial tubing systems showed the highest pressure gradient during expiration, which may be attributable to the tube's expiratory limb's greater length. This finding should call attention to patients presenting with expiratory flow limitation. During passive expiration, the respiratory systems' elastic recoil forces and total airway resistance determine the time required for complete exhalation. High artificial airway resistance, as caused by the coaxial tubing systems, may prolong expiratory time, thus promoting incomplete expiration and emergence of intrinsic PEEP.8
Although we found significantly higher resistances across disposable compared with reusable conventional tubing systems in 2 manufacturers, this difference was of minor clinical relevance. Both systems showed comparable geometries but varying properties of their tubes' inner surfaces. Disposable tubing systems (as well as coaxial tubing systems) are fabricated from thin plastic. This requires a corrugated texture of the material to ensure flexibility and stability at the same time. However, one can assume that the riffled surface promotes turbulent flow,9 which increases resistance. Our data support this assumption. Turbulent flow profiles prevailed in all tubing systems to different extents. This becomes evident by the nonlinear dependence of ΔP.
The high resistance of coaxial tubing systems was associated with a high additional WOB during spontaneous breathing. In a previous study including anesthetized, intubated, and spontaneously breathing subjects, total WOB/L of ventilation was found to amount to about 1 J/L.5 According to our results, a conventional tubing system would have contributed nearly 10% to the total WOB in those subjects. However, under the same assumptions, a coaxial tubing system would cause about 25% of the total WOB/L.
Pressure support ventilation may partly compensate for the additional WOB caused by coaxial tubing systems. Pressure support ventilation provides constant pressure support in inspiration, thereby inevitably leading to undercompensation or overcompensation of the airways' resistance, depending on the actual flow.10 However, to roughly compensate for the additional WOB, the amount of additional pressure support may correspond to ΔP600.
The higher additional WOB caused by a coaxial tubing system compared with a conventional one requires a larger breathing effort. Consequently, our volunteers rated the resistance of breathing via a coaxial tubing system higher than the resistance of breathing via a conventional tubing system. Whereas the healthy volunteers are likely to be able to tolerate this additional WOB, the patient with an impaired respiratory system may fail to do so. In this regard, the conventional tubing system clearly performs better.
It has to be noted that we have calculated additional WOB from the pressure-flow characteristics of the respective tubing system and the flow that was generated by the volunteers during breathing without a connected device. We omitted the direct measurement while breathing through the respective device for reasons of comparability between the investigated situations. First, we wanted to eliminate effects of breathing variability during the different trials. Second, we wanted to prevent adaptation of the breathing pattern in response to the demanded work of breathing.
Conclusions
In summary, all elements of the breathing circuit contribute to artificial airway resistance. Conventional tubing systems contribute to airway resistance only to a minor extent. By contrast, coaxial tubing systems contribute to airway resistance to a relevant extent. Based on these findings, we suggest applying coaxial tubing systems carefully with regard to their increased resistance.
Footnotes
- Correspondence: Johannes Spaeth MD MSc, Department of Anesthesiology and Critical Care, Medical Center, University of Freiburg, Hugstetter Strasse 55, 79106 Freiburg, Germany. E-mail: johannes.spaeth{at}uniklinik-freiburg.de.
This study was supported by departmental funding. The authors have disclosed no conflicts of interest.
Ms Wenzel presented a version of this paper at the Deutscher Anästhesie Congress, held April 14–16, 2016, in Leipzig, Germany, and at BMT 2016, held October 4–6, 2016, in Basel, Switzerland.
- Copyright © 2017 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}