

The postoperative period for patients has been a focus of research for decades. In the early 1940s, a number of publications began to surface that challenged the common practice of therapeutic bed rest after surgery.1 The resulting evidence demonstrated that allowing patients to ambulate by actively sitting up in a chair or getting up and walking had a significant effect on reducing postoperative pulmonary complications. In more recent years, device-specific therapies have emerged with the goal of improving lung function by either encouraging particular breathing patterns and effort by patients, or by generating positive airway pressure to reduce atelectasis and increase functional residual capacity.
A number of studies have evaluated lung expansion therapies and their effect on lung volume changes as postoperative interventions to prevent postoperative pulmonary complications.2,3 More than 30 years ago, Stock and colleagues demonstrated that use of incentive spirometry (IS) after upper abdominal surgery did not increase functional residual capacity compared to coughing and deep breathing.2 Similarly, in cardiac bypass patients, Jenkins and colleagues3 showed that IS did not result in an increase in functional residual capacity compared to early mobilization and huffing and coughing exercises. A Cochran review published in 20144 found no differences in clinical complications, respiratory failure, and pulmonary complications when the use of incentive spirometry was compared to no therapy or physiotherapy after abdominal surgery. More recently, a study randomized 387 patients to receive physiotherapy combined with IS (n = 195) or physiotherapy alone (n = 192) after lung resection surgery and prior to the patients being able to ambulate independently.5 They found no significant difference in postoperative pulmonary complications at 30 d and no difference between groups in pneumonia rates, need for mechanical ventilation, home oxygen, length of hospital stay, or readmission.5
The combined evidence currently does not support the use of IS over simply ambulating the patient. Perhaps other therapies with a different mechanism of action could provide postoperative benefit. IS encourages slow guided inspiration, which explains similarities between IS and deep breathing in studies.2 Devices such as EzPAP (Smiths Medical, Minneapolis, Minnesota) require patients to breathe normally, resulting in the generation of positive airway pressure acting as PEEP.
In this issue of Respiratory Care, Rowley et al6 randomized 112 subjects to receive either IS or EzPAP for 5 d after upper abdominal surgery. The authors wanted to determine if there was a significant change in end-expiratory lung impedance (ΔEELI) in the dorsal lung regions after lung expansion therapies. Electrical impedance tomography (EIT), a noninvasive and radiation-free imaging technique, provides breath-by-breath images of ventilation distribution and additional tools for measuring changes in EELI to selected regions of interest. A change in EELI represents a change in end-expiratory lung volume (EELV). Rowley et al6 chose a threshold ΔEELI of 15% to represent a clinically relevant change in dorsal region EELI after lung expansion therapies. This outcome only occurred once on postoperative day 1 in the IS group. On day 3 and day 5, the median dorsal ΔEELI were all < 10% for both study groups. However, there was a median increase of 20% or more in ventral ΔEELI on postoperative day 3 and day 5 for the IS group. Although belt positioning between days could explain this difference, this would be a type of non-differential (or random) error that is not likely to affect only the group receiving IS treatment.
Although increasing dorsal ΔEELI seems to make intuitive sense because of the likely hood of having dorsal region atelectasis post-surgery, the ΔEELI in ventral regions can be less intuitive to understand. Similarly, the global ΔEELI can be misleading because this ignores ventral dorsal differences. An increase in EELI if representing an increase in EELV can have very different clinical meanings based on where the increase occurs but more important are the changes in regional compliance.
To understand whether an increase in ventral ΔEELI is beneficial or potentially harmful, the tidal variation (end-inspiratory distribution) information is important, although not reported by Rowley et al.6 In fact, it should be noted that the distribution of ventilation referred to in their paper refers to distribution of the ΔEELI, not the distribution of tidal volume (represented by tidal variation with EIT). Tidal variation is used to describe the change in ventilation to an area and changes in regional compliance, which is quite different than ΔEELI, which represents the changes in end-expiratory level only.
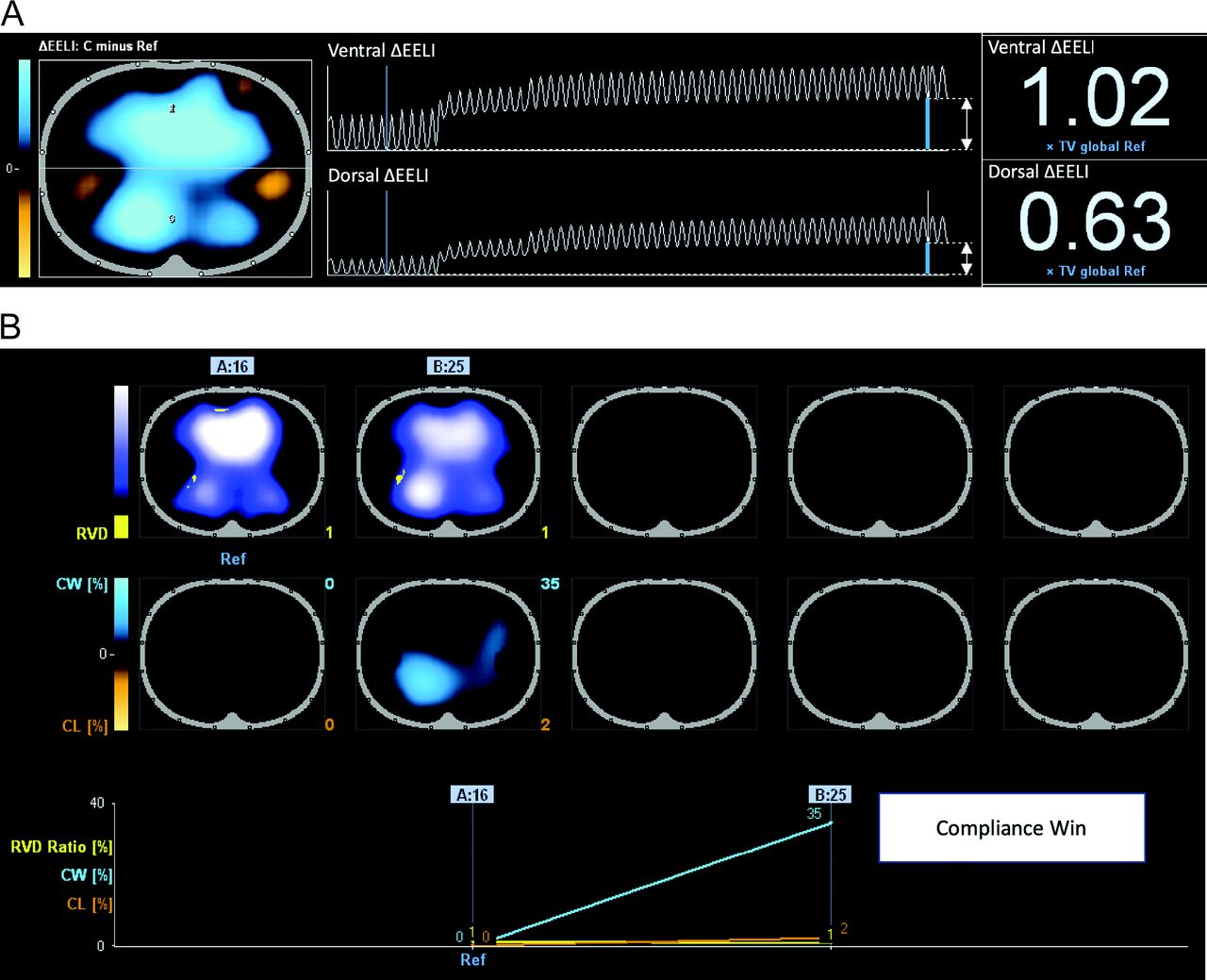
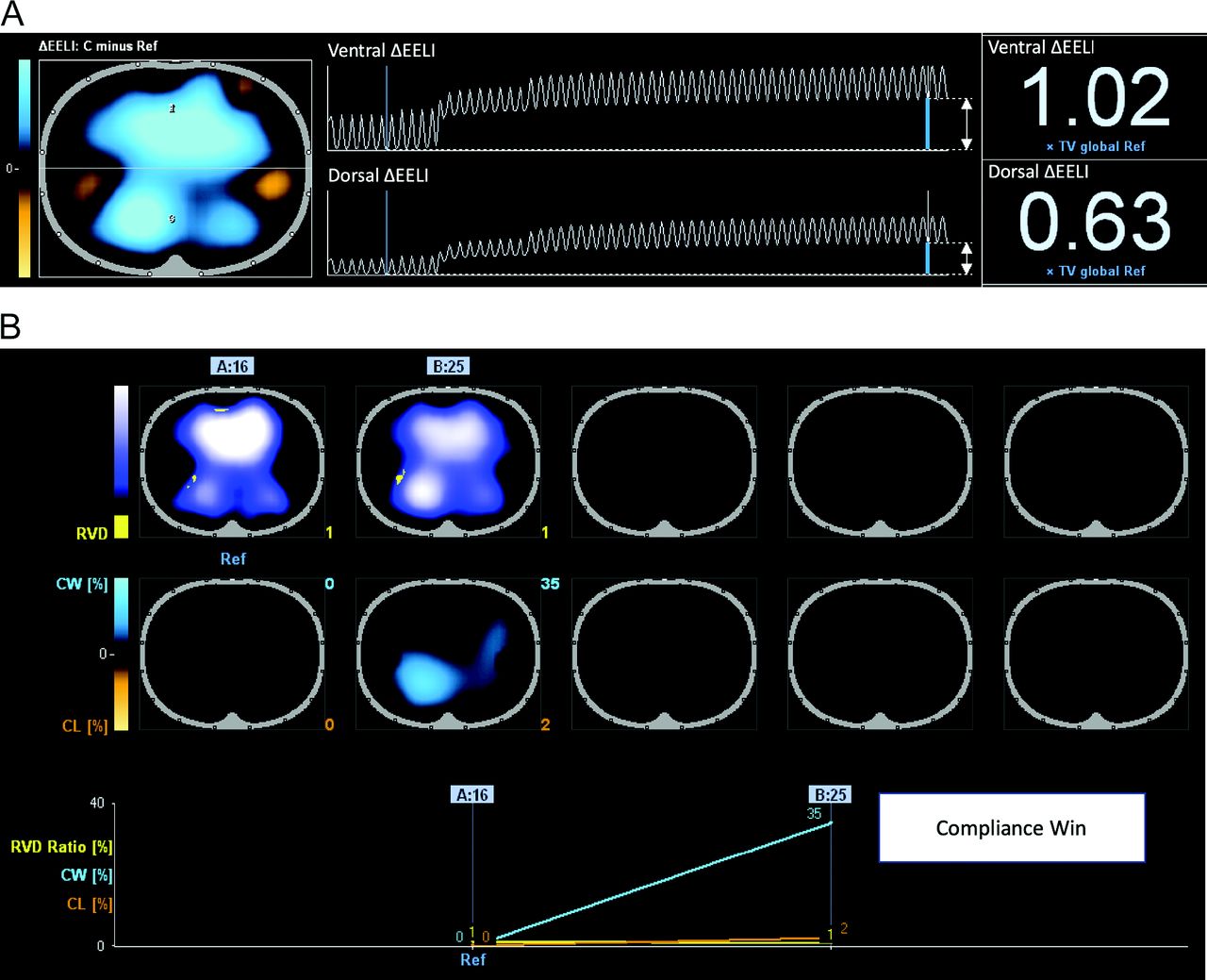
In passively ventilated critically ill patients, changes in EELI after increasing PEEP are often predominant in the ventral regions, in both recruiters and non-recruiters. This is because the ventral regions are the most compliant regions while in the supine position. However, the regional compliance changes can be used to distinguish potential benefit, or the lack thereof. An increase in dorsal region compliance would be demonstrated by a shift of ventilation distribution (tidal variation) to the dorsal regions during inspiration, without a significant loss of ventilation distribution to the ventral regions. In Figure 1A, a larger increase in ventral ΔEELI (compared to dorsal ΔEELI) is associated a significant worsening in ventral region compliance with minimal to no improvement in dorsal region compliance (Fig. 1B). In Fig. 2A, a similar increase in ΔEELI is seen in the ventral and dorsal regions, but with a significant improvement in dorsal region compliance with no loss of ventral region compliance (Fig. 2B). Future studies looking at lung expansion therapies should consider both ΔEELI and regional compliance. This would allow analyses to be done in subjects that show improvements in both ΔEELI and regional compliance.

(A) An increase in PEEP from 14 cm H2O to 25 cm H2O shows an increase in ΔEELI in both the ventral and dorsal regions (predominantly in the ventral regions). (B) The resulting regional compliance is worse in the ventral regions with no improvement in dorsal region compliance.
(A) An increase in PEEP from 16 cm H2O to 25 cm H2O shows an increase in ΔEELI in both the ventral and dorsal regions (predominantly in the ventral regions). (B) The resulting regional compliance is improved in the dorsal regions with no worsening in ventral region compliance.
The measurement of EELI has significant limitations that clinicians need to be aware of. First, movement or changes in pressure applied to the EIT belt can impact the measurements between electrodes. This artifact is commonly seen in patients lying on ICU beds with inflatable mattresses and alternating pressure settings (Fig. 3). The artifact does not change measurements of distribution of ventilation (tidal variation), but it can drastically affect the EELI measurements. Second, the administration or removal of fluid can also impact EELI. Patients receiving aggressive fluid removal can show significant changes in EELI, but with no change in distribution of ventilation measured by EIT or respiratory system mechanics. Figure 4 demonstrates ΔEELI over 30 min in a patient who received a furosemide bolus. The ΔEELI increases over time, but there is no change in the distribution of ventilation (tidal variation), and no changes occurred in respiratory system compliance. In a recent letter published in the American Journal of Respiratory and Critical Care Medicine, a significant decrease in ΔEELI results after a patient is given a fluid bolus, also with no changes in any respiratory system mechanics or distribution of ventilation.7

The effects of automated bed mattress pulsation on the EELI measurements.

EELI measurements following a bolus of furosemide. EELI continues to increase with no change in distribution of ventilation.
Due to these limitations, it is important to establish a period of baseline quiet breathing lasting 2–5 min to ensure patients are relatively still during therapy, and patients should not receive fluid boluses or diuretic boluses during assessment. Stability was assessed in the article by Rowley et al6 by recording 2 min of eupneic breathing before and after the lung expansion therapies.
Finally, ΔEELI has been used to study the effects of setting PEEP in patients with hypoxemic respiratory failure8 and its correlation with changes in EELV have good correlation, although the limits of agreement with nitrogen wash-in/wash-out techniques are less than acceptable when considering the actual amount of volume.9–12 Therefore, although the absolute volume of the increase in EELV is questionable due to accuracy, an increase is correlated to the ΔEELI.
A similar study was performed postoperatively in healthy endorological surgery patients.13 These authors also found an increase in EELI post-therapy, but this effect wore off during post-therapy quiet breathing. Rowley et al6 reported sustained changes after 2 min of eupneic breathing; it is unclear how long the effects remained, but considering there was no difference in hospital stay and no association between therapy device and postoperative pulmonary complications, it likely had no lasting benefit. Although the results of these recent EIT studies of lung expansion therapies appear consistent with those from the past, they did not include a control group of subjects without lung expansion therapies. These studies only answer the question of differences between therapies. There appears to be no difference between therapies in terms of clinically relevant outcomes, and both seem to provide no lasting benefits after therapy.
It is clear from the currently available evidence that postoperative lung expansion therapies provide no clinically relevant benefit. The use of EIT to assess the response to lung expansion therapies is an intuitive concept that can provide valuable information, provided the limitations of ΔEELI measurements is understood. Future studies should evaluate the differences between subjects with significant improvements in EELI, along with improvements in dorsal region compliance as measured with EIT to those with no improvements in dorsal region compliance. However, the issue will always be whether the benefits of the lung expansion therapies are short-lived, even in subjects with the best response to therapy. Despite the current lack of evidence for its use, lung expansion therapies are still used routinely without any clear value (cost/benefit), and hospitals continue to provide the therapy as a result of habitual rather than evidence-based practice.
Footnotes
- Correspondence: Thomas Piraino RRT FCSRT, St. Michael's Hospital, 30 Bond Street, Toronto, Ontario M5B 1W8, Canada. E-mail: thomaspiraino{at}gmail.com.
Mr Piraino has disclosed relationships with Dräger, Philips, and Fisher & Paykel.
See the Original Study on Page 1181
- Copyright © 2019 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}
{kind=link}