

Abstract
BACKGROUND: Dynamic hyperinflation, caused by expiratory flow limitation, markedly increases resting end-expiratory lung volume (functional residual capacity) in many COPD patients.
OBJECTIVE: To determine the impact and duration of impact of CPAP on hyperinflation and airway resistance in patients with stable COPD.
METHODS: In a case series, 21 patients underwent CPAP at 8 cm H2O for 15 min, then whole-body plethysmography immediately after, and at 15 and 30 min after CPAP.
RESULTS: The cohort's mean ± SD age was 70 ± 9 y, and the mean FEV1 was 41 ± 8% of predicted. Residual volume, functional residual capacity, total lung capacity, the ratio of residual volume to total lung capacity, and airway resistance decreased after CPAP and did not significantly change at 15 min (P < .001), but returned to baseline at 30 min.
CONCLUSIONS: In patients with severe to very severe stable COPD, CPAP reduces lung volumes and airway resistance for 15 min, but the lung volumes return to baseline by 30 min.
- chronic obstructive pulmonary disease
- COPD
- continuous positive airway pressure
- CPAP
- pulmonary hyperinflation
Introduction
The progression of COPD is associated with increased breathlessness, exercise intolerance, and impaired quality of life. Pulmonary rehabilitation is an efficient way to minimize the symptoms caused by COPD. CPAP has been used as an adjunct to pulmonary rehabilitation to reduce the work of the respiratory muscles and improve effort tolerance.1,2
As a result of dynamic hyperinflation caused by expiratory flow limitation, resting end-expiratory lung volume (functional residual capacity [FRC]) is markedly increased in many COPD patients. The increase in a subject's operating volumes at a given ventilatory rate expands the passive pressure load that needs to be overcome by the inspiratory muscles, and therefore, the work of breathing.3,4 Moreover, the time available for expiration may be insufficient to allow the system to return to end-expiratory lung volume. The residual inward elastic recoil creates a positive alveolar pressure at the end of expiration, known as auto-PEEP.5
During mechanical ventilation, auto-PEEP is a common feature observed in COPD patients; however, it is also common in stable COPD patients, even in the absence of respiratory failure.6 The presence of auto-PEEP requires inspiratory muscles to generate sufficient force to overcome the opposite recoil pressure before inspiratory flow can begin. In this regard, auto-PEEP acts as an inspiratory threshold load and represents additional impedance contributing to both elastic work of inspiration and the sensation of dyspnea. COPD patients' respiratory muscles must, hence, generate more negative pleural pressure swings in order to initiate a breath during spontaneous and/or assisted ventilation. According to the “waterfall” theory, if auto-PEEP is the result of expiratory flow limitation, then extrinsic, applied PEEP at the airway opening should decrease the pressure gradient between the mouth and alveoli at end-expiration (the inspiratory load).7
The effects of CPAP on lower-airway function are poorly understood. In patients with stable COPD, the benefits of CPAP may be explained by a reduction in lung hyperinflation.6,8 Indeed, several investigators have found that applied PEEP can counterbalance auto-PEEP without causing further hyperinflation.9,10 CPAP and applied PEEP decrease the inspiratory load at any given volume, therefore reducing the increased work-load and improving lung mechanics until a critical PEEP value is reached. Some researchers suggested that a PEEP of 5–10 cm H2O could partially decrease airway resistance (Raw), especially at the end of expiration, resulting in a faster and more uniform lung emptying.11,12 Applied PEEP above 10 cm H2O increases hyperinflation and worsens respiratory mechanics, muscle activity, and hemodynamics.13,14
Given the few and contradictory results of studies on the influence of CPAP in patients with stable severe airway obstruction, we investigated the impact and duration of impact of CPAP on hyperinflation and Raw in patients with stable COPD.
Methods
Per the World Medical Association Declaration of Helsinki, this study was approved by the ethics committee of Augusto Motta University, and written informed consent was obtained from all participants. The study was performed in the Respiratory Physiology Laboratory at the University of the State of Rio de Janeiro, Rio de Janeiro, Brazil.
Patients
From January 2009 to February 2010, we prospectively studied COPD patients referred to our respiratory physiology laboratory. We recruited 25 patients whose spirometry indicated severe or very severe COPD.15 All the subjects had been or were heavy cigarette smokers. All the patients were stable (no COPD exacerbation in the previous 2 months), and had not taken any bronchodilators for ≥ 24 h before the protocol measurements.
Experimental Procedures
Figure 1 describes the sequence of measurements conducted with each patient. Spirometry (Collins Plus Pulmonary Function Testing System, Warren E Collins, Braintree, Massachusetts) was performed between 8:00 and 10:00 am, according to the American Thoracic Society standards.16 The results are expressed in absolute and percent-of-predicted values.17

Sequence of measurements.
After spirometry the subject underwent CPAP (Remstar Pro with C-Flex, Respironics, Murrysville, Pennsylvania) at 8 cm H2O, for 15 min, in the sitting position, via face mask (Image III, Respironics, Murrysville, Pennsylvania), on room air. Before CPAP, immediately after CPAP, and 15 min and 30 min after CPAP we measured heart rate, SpO2 (Pulsox-3i, Minolta, Osaka, Japan), respiratory rate, and blood pressure.
Before CPAP, immediately after CPAP, and 15 min and 30 min after CPAP we measured lung volumes with a constant-volume, variable-pressure plethysmograph (Warren E Collins, Braintree, Massachusetts). Measurements were taken with the subject panting shallowly at a 1–2 breaths per second and supporting the cheeks and floor of the mouth with their hands to reduce compliance and minimize the volume changes of the mouth and pharynx. The reported thoracic gas volume was averaged from 3 to 5 acceptable panting maneuvers. We recorded inspiratory capacity, total lung capacity (TLC), FRC, residual volume (RV), RV/TLC, and Raw. The results are expressed in absolute (static lung volumes and Raw), and percent-of-predicted values (static lung volumes).18
Data Analysis
We analyzed the data with statistics software (SAS 6.11, SAS Institute, Cary, North Carolina). We examined the effect of CPAP with repeated-measures 2-way analysis of variance. P < .05 was considered statistically significant. We conducted secondary analysis with the Bonferroni multiple-correction test, in which P < .005 was considered statistically significant.
Results
Four patients were unable to perform body plethysmography and were excluded. The remaining 21 patients completed the study measurements (Table 1). Table 2 shows the effects of CPAP on the respiratory and hemodynamic variables. There was a statistically significant difference in respiratory rate and SpO2 (P < .001).
Baseline Anthropometry and Respiratory Function Data (n = 21)
Effects of CPAP on Respiratory Rate, SpO2, Heart Rate, and Blood Pressure
Table 3 shows the plethysmography results. All the differences were statistically significant (P < .001 via analysis of variance). Immediately after CPAP, inspiratory capacity was significantly increased (Fig. 2), and TLC (Fig. 3), RV (Fig. 4), and Raw (Fig. 5) were significantly decreased.
Effects of CPAP on Plethysmography Variables*
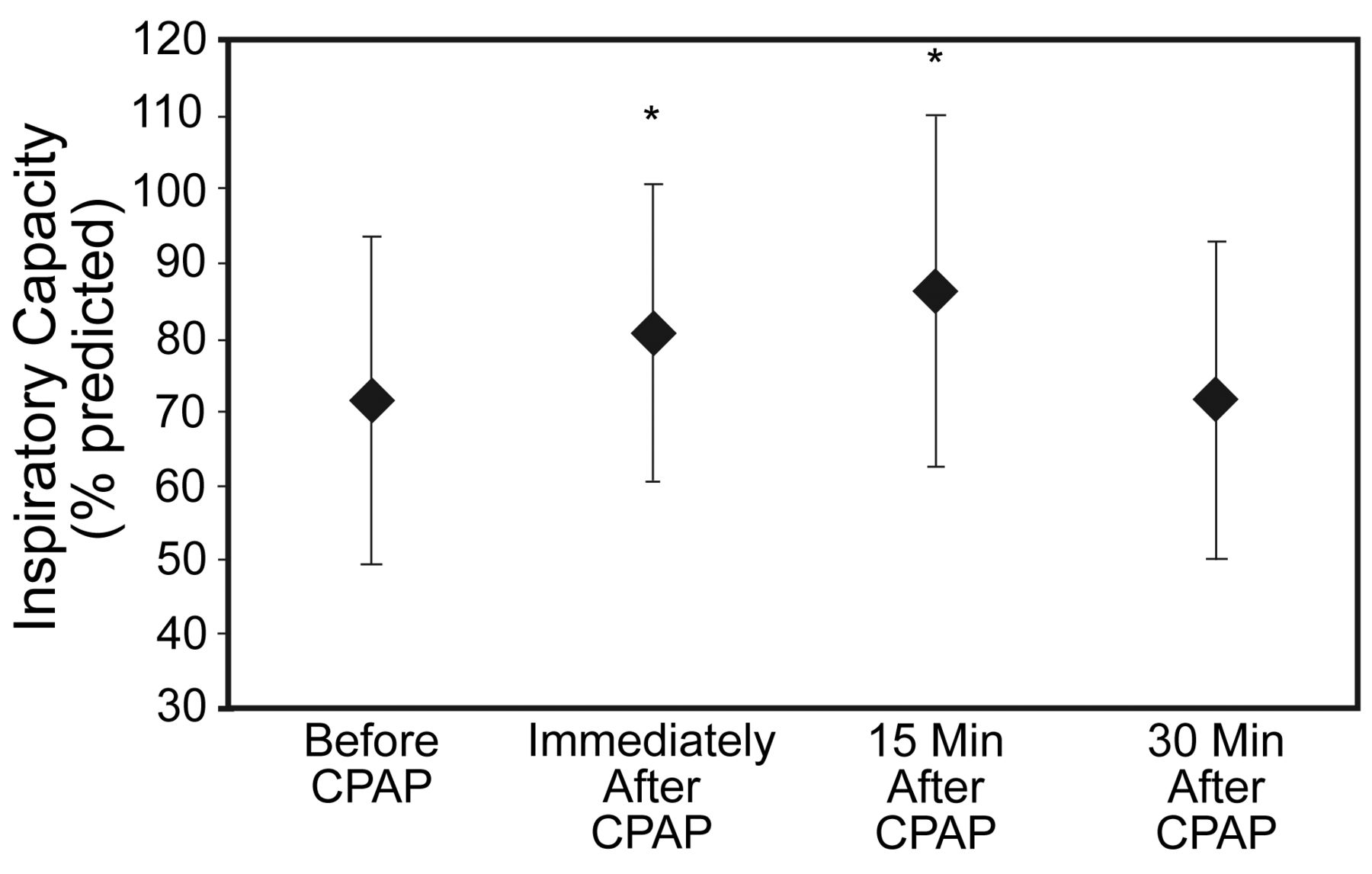
Inspiratory capacity before and after CPAP. * Significantly different from baseline (before CPAP).

Total lung capacity before and after CPAP. * Significantly different from baseline (before CPAP).

Residual volume before and after CPAP. * Significantly different from baseline (before CPAP).
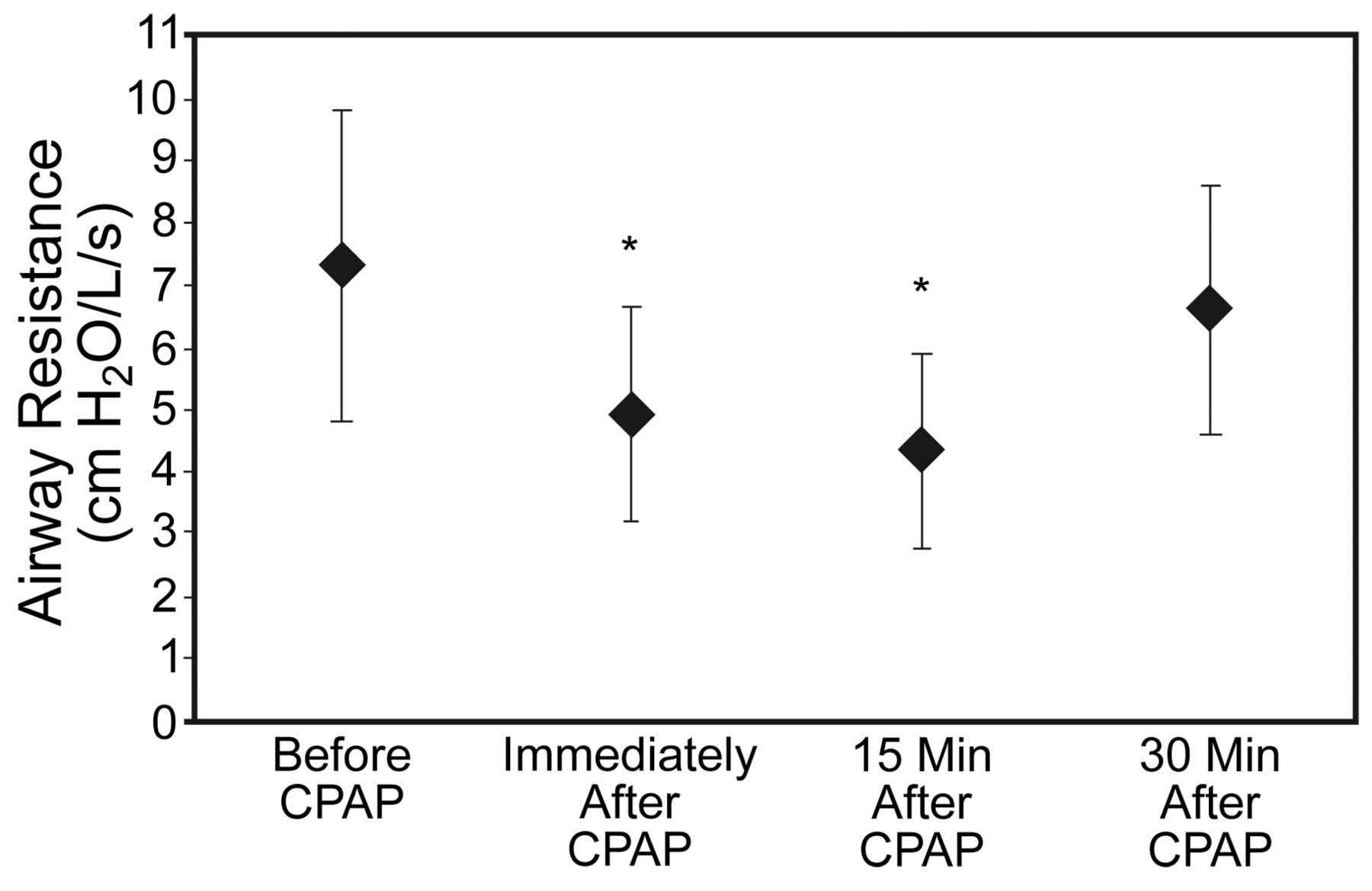
Airway resistance before and after CPAP. * Significantly different from baseline (before CPAP).
Discussion
CPAP decreased lung hyperinflation and Raw in patients with stable but severe COPD, and the benefit was sustained for at least 15 min but had disappeared at 30 min. To our knowledge, this is the first study to use body plethysmography to address the effects of CPAP upon pulmonary volumes and Raw in stable COPD patients. Other studies of CPAP in stable COPD have yielded conflicting results; nevertheless, there is some evidence that CPAP prevents gas-exchange deterioration, improves quality of life, and reduces the need for hospitalization in patients with hypercapnia or nocturnal hypoventilation.8,19,20 In addition to the favorable findings on CPAP for COPD exacerbation, some studies have found that CPAP either during or between exercise sessions can enhance the benefits of pulmonary rehabilitation.1,2,21,22 However, the underlying mechanisms of CPAP benefits are not fully understood. Since the applied PEEP given by CPAP counterbalances auto-PEEP, decreasing the pressure gradient between the mouth and alveoli at end expiration, one theory is that CPAP rests chronically fatigued respiratory muscles. The load reduction on the respiratory muscle pump seems to restore both central chemosensitivity and central drive to breathe.23 Additionally, a low level of CPAP can reduce the inspiratory swings in esophageal and transdiaphragmatic pressure and the amount of both paradoxical motion and expiratory recruitment of the abdominal muscles,24 by reducing auto-PEEP and the elastic work carried out.
We found that CPAP significantly increased inspiratory capacity and significantly decreased RV, FRC, and TLC. This inspiratory capacity improvement is very similar to that reported by Soares et al,6 who observed an average increase of 6.7% from baseline in responder patients. Soares et al did not measure RV, FRC, and TLC. Our results also agree with those of Díaz et al,8 who found that short-term noninvasive ventilation (bi-level positive airway pressure) significantly reduced RV (from 201 ± 48% of predicted to 165 ± 49% of predicted, P < .001) and TLC (from 173 ± 36% of predicted to 148 ± 35% of predicted, P < .001) in stable COPD patients. However, Díaz et al measured lung volumes with the nitrogen-washout method, the accuracy of which depends on all parts of the lung being well ventilated. The plethysmographic TLC value is often higher than that measured with the nitrogen washout, and patients with emphysema can have a ≥ 1-L TLC difference between the methods.14,24 Soares et al6 and Díaz et al8 assessed only the immediate effects of noninvasive ventilation.
A possible explanation for the lung volumes reduction after CPAP is the increase in expiratory time, which could favor the emptying of slow-time-constant lung units. Although Díaz et al8 found that a lower end-expiratory lung volume could be reached at the end of each CPAP session and maintained afterward by a newly adopted spontaneous pattern of breathing, the patients they studied returned to their baseline RV, FRC, and TLC after 30 min.
An acceptable plethysmography panting maneuver requires a certain degree of subject coordination.24 In subjects with severe airway obstruction, relatively minor changes in measured FRC can relate to small adjustments of position, anxiety, minute ventilation, and point of shutter closure, and one or more of these factors might have been operative on their second exposure to the plethysmograph.
We selected a CPAP pressure of 8 cm H2O based on previous investigations, and the fact that CPAP of 8 cm H2O does not increase hyperinflation in COPD patients.12,25,26 Increased hyperinflation has been observed at higher CPAP levels. Lim found increased FRC when CPAP increased above 10 cm H2O.27 Therefore, CPAP greater than 10 cm H2O may impair the function of the inspiratory muscles if it increases the operating volumes above the levels imposed by expiratory flow limitation, in particular if the operating volumes increase to the point at which the inspiratory muscles work at disadvantageously shorter lengths or less favorable mechanical advantage.9 Moreover, hemodynamic consequences can be expected as a direct result of both dynamic hyperinflation and auto-PEEP. The increase in lung volume may reduce venous return, directly through compression of the vena cava and right heart, and indirectly through an increase in right atrial pressure, decreasing the pressure gradient for venous return.10,14
The effects of nasal CPAP on the lung parenchyma of stable COPD patients has been assessed via high-resolution computed tomography. In a recently published study, Holanda et al28 obtained high-resolution computed tomography of 11 stable spontaneously breathing COPD patients immediately after CPAP trials of 5, 10, and 15 cm H2O. CPAP at 5 cm H2O caused regional lung deflation, whereas CPAP at 10 and 15 cm H2O increased the emphysematous zones in all of the pulmonary regions. Those results are consistent with those observed in relation to lung function.
Measurement of Raw may help distinguish airway obstruction due to intrinsic narrowing of the airway by mucus hypersecretion and bronchial wall inflammation (eg, chronic bronchitis) or to the loss of lung elastic recoil (eg, emphysema). Although Raw is elevated in both disorders, the increase is usually more marked in chronic bronchitis.24,29 In the Van Noord et al study,29 the resistance values were only marginally higher than in normal subjects. One explanation could be the predominance of subjects with emphysema rather than with chronic bronchitis.
After CPAP at 8 cm H2O the results showed significant Raw reduction. O'Donoghue et al30 used CPAP increments of 1 cm H2O in patients with severe stable COPD and found an Raw reduction tendency, from 16.5 cm H2O/L/s with 0 CPAP to 3.5 cm H2O/L/s at CPAP of 10 cm H2O. That difference was not significant (P = .08). Smith and Marini10 reported that applied PEEP may reduce Raw and the mechanical work of breathing in patients with severe COPD. The suggested mechanisms to explain the reduced Raw are the decrease of airway wall edema, the stretching open of chronically fibrosed airways, and the recruitment of normal lung, previously collapsed by hyperinflated emphysematous areas, with a consequent increase in airway tethering.21,31
Like previous authors, we did not measure auto-PEEP. Since all the patients had severe air-flow obstruction, we assumed that the results were related to the impact of applied PEEP on expiratory flow limitation and auto-PEEP. Our findings support the adjustment of PEEP in the therapeutic setting, especially when the foremost objective is to improve respiratory mechanics and reduce the respiratory muscle overload.
It could be conjectured that there is a relationship between the duration of CPAP and the duration of its benefits, or that a higher CPAP pressure might produce greater effects or longer duration, but further studies are necessary to answer those questions.
Conclusions
CPAP reduces lung volumes and Raw in patients with severe stable COPD, and the benefits last for 15–30 min after CPAP.
Footnotes
- Correspondence: Agnaldo J Lopes MD PhD, Rehabilitation Science Graduate Program, Augusto Motta University, Rio de Janeiro, Brazil, Rua Araguaia 1266 bloco 1/405, Freguesia, Jacarepaguá, Rio de Janeiro, Brazil 22745–271. E-mail: phel.lop{at}uol.com.br.
-
The authors have disclosed no conflicts of interest.
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}