

Abstract
BACKGROUND: Prolonged mechanical ventilation is increasingly common in ICUs. Although a consensus conference defined weaning success in this patient population, few studies have used this definition. A clear definition of successful weaning is useful to assess clinical and epidemiological outcomes, facilitate clinical decision making, and set goals of care. The aims of our study were to describe the prevalence of reinstitution of mechanical ventilation within 28 d in patients successfully weaned according to our institution criterion (ie, weaning success as per consensus guidelines), to describe reasons to reestablish mechanical ventilation, and to identify associated factors.
METHODS: An observational, analytical, cross-sectional study was conducted at a weaning and rehabilitation center. All patients liberated from mechanical ventilation (ie, no ventilatory support for 7 d) were included as subjects. Requirement of and reasons for reinstitution of mechanical ventilation within 28 d of weaning were recorded.
RESULTS: A total of 639 tracheostomized subjects were analyzed. Of these, 219 (34%) were weaned, and 15 were eliminated due to lack of data. Of the remaining 204 subjects, 42 (21%) were reconnected to mechanical ventilation within 28 d. Sepsis accounted for 64% of reconnections. In the multivariate analysis, neurological comorbidity (adjusted odds ratio 5.1 [95% CI 2.3–11.1]) and delayed weaning (> 7 d after admission) (adjusted odds ratio 2.37 [95% CI 1.1–5.3]) were independently associated with reinstitution of mechanical ventilation within 28 d of weaning. The synergistic effect of both variables showed an adjusted odds ratio of 5.35 (95% CI 2.4–11.4).
CONCLUSIONS: Reinstitution of mechanical ventilation within 28 d is a common event in patients considered to be weaned: 1 in 5 of such patients requires reconnection to mechanical ventilation, with sepsis being the most prevalent cause. Neurological comorbidity and delayed weaning are risk factors associated with reestablishment of mechanical ventilation. The presence of more than one risk factor increases the association with reinstitution of mechanical ventilation within 28 d of weaning.
Introduction
Advances in intensive care have enabled more patients to survive a critical illness.1 This has led to a concomitant increase in the number of patients requiring prolonged mechanical ventilation (PMV), defined as mechanical ventilation for ≥ 21 consecutive days, for at least 6 h per day.2 Weaning success in patients with PMV is a prognostic factor associated with good outcome3–5; however, success rates range from 25% to 75%.5–14 The definition of weaning success plays a crucial role in epidemiological and clinical studies of invasive mechanical ventilation.15,16 A clear definition of weaning success allows the assessment of the efficacy of weaning protocols, a more accurate estimation of mechanical ventilation outcomes, and comparisons across centers.2 Furthermore, such a definition may be useful to guide discussions about prognosis with patients and their families, facilitate clinical decision-making, and set goals of care.16 Successful weaning has been defined by a consensus conference as liberation from PMV for 7 consecutive days.2 This is the definition adopted by our center. However, time-based success criteria are known to be arbitrary.2 In a review of definitions applied to describe cohorts of subjects receiving PMV, Rose et al16 found 54 studies that defined weaning success with a time-based criterion. Of these studies, only 33% used the 7-d ventilator-free period proposed in the consensus statement. In the rest of the studies, weaning success was variably defined as 6 h, 24 h, 48 h, 72 h, 5 d, 14 d, or 28 d without mechanical ventilation. Therefore, what constitutes PMV weaning success is currently unclear. In a previous study performed at our institution that involved 372 subjects undergoing PMV, 186 were weaned and 76 (40.9%) required reinstitution of mechanical ventilation, with a median of 16 d to reconnection (interquartile range 7–34.5).5 Schönhofer et al10 proposed considering the presence or absence of subsequent clinical stability in addition to time-based weaning success. Other authors have defined weaning success as freedom from ventilatory support at the time of discharge.6,14,16,17
According to the consensus statement, patients with PMV should only be considered to be successfully weaned when they are able to breathe spontaneously without ventilatory support for at least 7 d because respiratory system recovery is slower and chronic comorbidities are prominent in this patient population. Unlike short-term mechanical ventilation, where the time threshold for successful weaning (ie, 48–72 h) is associated with the likelihood of respiratory failure following extubation, defining a time criterion may be less intuitive in patients requiring PMV.2
Experts conclude that currently existing databases should be used to define the duration of the weaning process that best predicts long-term success (ie, durability of weaning success); in addition, they suggest analyzing factors resulting in reinstitution of mechanical ventilation to clarify the definition of weaning success in patients with PMV.2
The primary objective of our study was to describe the prevalence of reinstitution of mechanical ventilation within 28 d in subjects deemed to be successfully weaned according to our institution's criterion (ie, weaning success as per consensus guidelines). Secondary objectives were to describe the reasons for and to identify factors associated with the reinstitution of mechanical ventilation.
QUICK LOOK
Current knowledge
The consensus statement on prolonged mechanical ventilation (PMV) suggests defining successful weaning as 7 consecutive days without ventilator support. However, this criterion is not used by all researchers. A clear definition of successful weaning from PMV allows assessment of efficacy of weaning protocols and of outcomes in this group of patients, as well as comparisons across weaning centers for patients requiring PMV.
What this paper contributes to our knowledge
Our findings on reinstitution of mechanical ventilation within 28 d of weaning and reasons for weaning failure support the criteria proposed in the consensus statement on PMV. It may be unnecessary to wait ≥ 7 d to define weaning success because most cases of reinstitution of mechanical ventilation are due to infection, likely a new event rather than failure of the weaning process. We could not establish with certainty whether infections were acute or chronic in our population. The probability of reinstituting mechanical ventilation was high in subjects with neurological comorbidities and those weaned after ≥ 7 d in our facility.
Methods
This was an observational, analytical, cross-sectional study performed from May 2017 to August 2017 at Clínica Basilea, a weaning and rehabilitation center located in Buenos Aires, Argentina. The study sample was selected from patients admitted to our institution from May 2004 to April 2017 who required mechanical ventilation. Subjects successfully weaned from PMV (ie, meeting the consensus criterion of 7 d without ventilatory support)2 were included in the study. The subjects' medical records were reviewed from the first night with no mechanical ventilation through day 28. Successfully weaned patients were excluded if they were hospitalized at our institution at the time of study closure or if they were discharged home, were transferred to an acute care facility, or died within 28 d of weaning. Subjects were also eliminated from the study when lack of data (eg, date of or reason for reconnection to mechanical ventilation) prevented the required analysis. Subjects' personal data were not included in the database; they were coded using correlative numbers based on date of admission. The study protocol was reviewed and approved by the Research Review Board of Clínica Basilea.
The need for reinstitution of mechanical ventilation within 28 d of weaning was recorded, as was the cause. Medical records pertaining to the day of reconnection were reviewed by 2 respiratory therapists to determine the cause of mechanical ventilation reinstitution (cause described by the physician and the respiratory therapist). If the reviewers did not agree on the cause, the reason for the reestablishment of mechanical ventilation was determined by the principal investigator.
On the basis of previous studies conducted at our institution,5,18 we analyzed the following variables potentially associated with reinstitution of mechanical ventilation: age, gender, comorbidities, reason for ICU admission, Glasgow Coma Scale, hemoglobin and albumin levels on admission to the weaning and rehabilitation center, and days to weaning in the weaning and rehabilitation center (calculated as days on mechanical ventilation from admission to the weaning and rehabilitation center until the first 24 h with no need for mechanical ventilation). Any preexisting disease at the time of ICU admission was recorded as a comorbidity. On the basis of previously published data,5 the need for > 7 d to achieve weaning success from the date of admission to the weaning and rehabilitation center was considered delayed weaning. In addition, the reason for discharge from the weaning and rehabilitation center was recorded. An analysis of subgroups at potential risk for the reinstitution of mechanical ventilation was performed in subjects with respiratory comorbidities or COPD as the reason for admission to the ICU, based on potential development of hypercapnic respiratory failure over time.
Subjects were followed during their entire stay in the institution. Days to weaning in the weaning and rehabilitation center (from admission to the first 24 h with no need for mechanical ventilation), date of and reason for discharge, date of and reason for transfer to an acute care facility, and mortality were recorded.
For data analysis, the sample was grouped into 2 categories according to whether or not subjects required reinstitution of mechanical ventilation within 28 d of weaning. Continuous variables were presented as mean ± SD or as median (interquartile range), as appropriate. Categorical variables were presented as absolute number and percentage. For comparison of continuous variables, the Student t test or the Mann-Whitney U test were used, and for comparison of proportions, the chi-square test or the Fisher exact test were used, as appropriate.
For a better interpretation in the logistic regression analysis of the numerical variables (continuous or discrete) that were significant, the sample median of each variable was used as the cut-off value. A univariate analysis was performed using a logistic regression model to estimate the effects of multiple variables on the need to reinstitute mechanical ventilation within 28 d of weaning. A significance threshold of P < .10 was chosen to include variables in the model. Odds ratios and their corresponding 95% CIs were estimated.
A risk analysis of variables that were significant in the logistic regression model was carried out to define their diagnostic performance in predicting the likelihood of reinstituting ventilation within 28 d of weaning. Interaction between variables was estimated using the Rothman synergy index.
A multivariate analysis was performed using a logistic regression model to estimate simultaneous effects of multiple variables on the need to reinstitute mechanical ventilation within 28 d of weaning. Confounding factors and interaction between variables were assessed. Odds ratios and their corresponding 95% CIs were estimated. P values < .05 were considered statistically significant. Sensitivity, specificity, and positive and negative likelihood ratios were calculated for variables that were significant in the multivariate analysis. Data analysis was performed using SPSS 20.0 (IBM, Armonk, New York).
Results
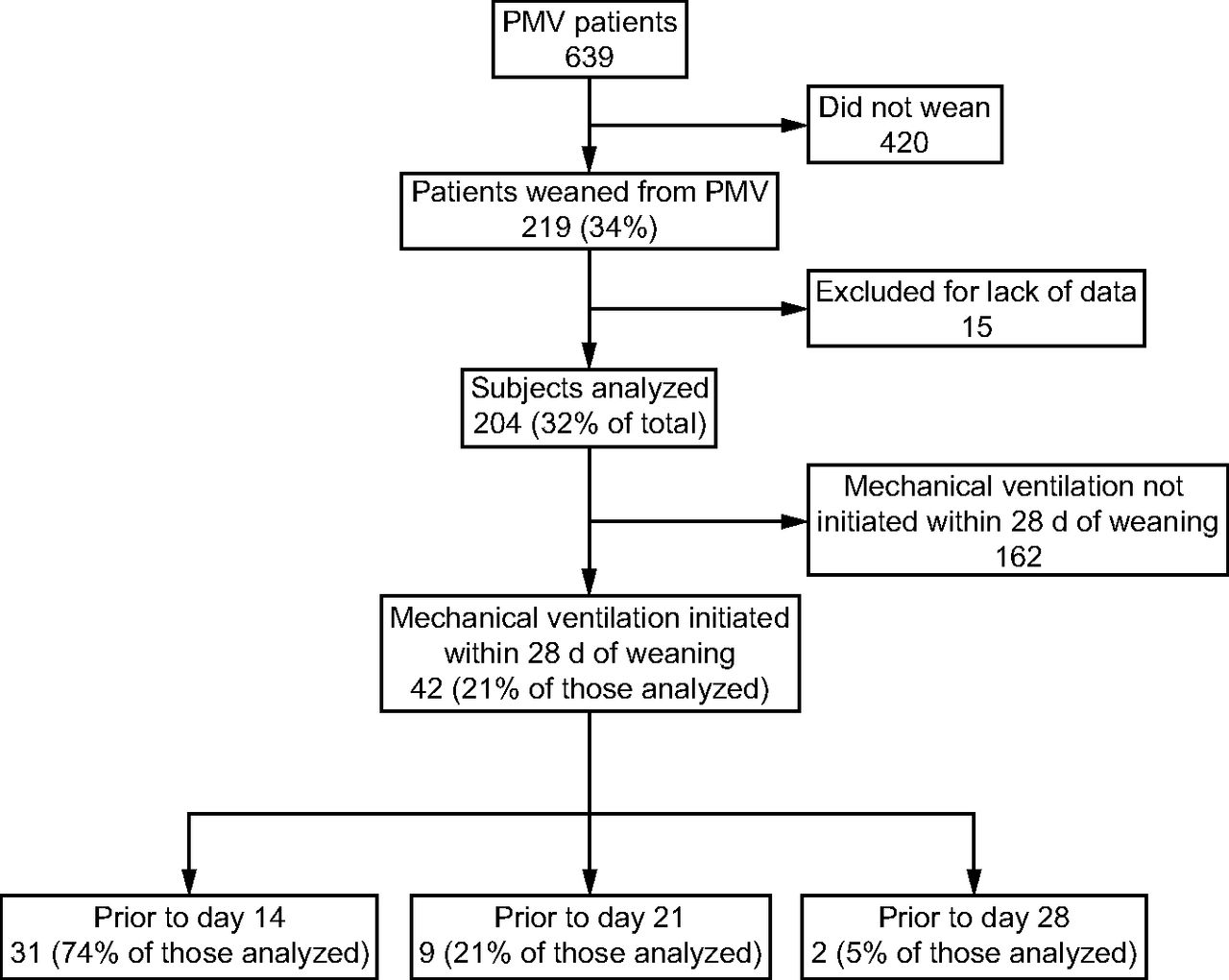
During the analysis period, 639 tracheostomized patients receiving PMV were admitted to the weaning and rehabilitation center; 219 (34%) of them were weaned, and 15 (6.8%) were excluded due to lack of data (date of or reason for reinstitution of mechanical ventilation). Of the 204 subjects included in the analysis, 42 (21%) were reconnected to mechanical ventilation within 28 d of weaning (Fig. 1). Table 1 shows data for subjects requiring and not requiring reinstitution of mechanical ventilation. The 204 subjects included comprise 100% of data of the study variables. No subjects had to be eliminated from the analysis. No significant differences were found in the analysis of subgroups with respiratory comorbidity or COPD as the reason for ICU admission.
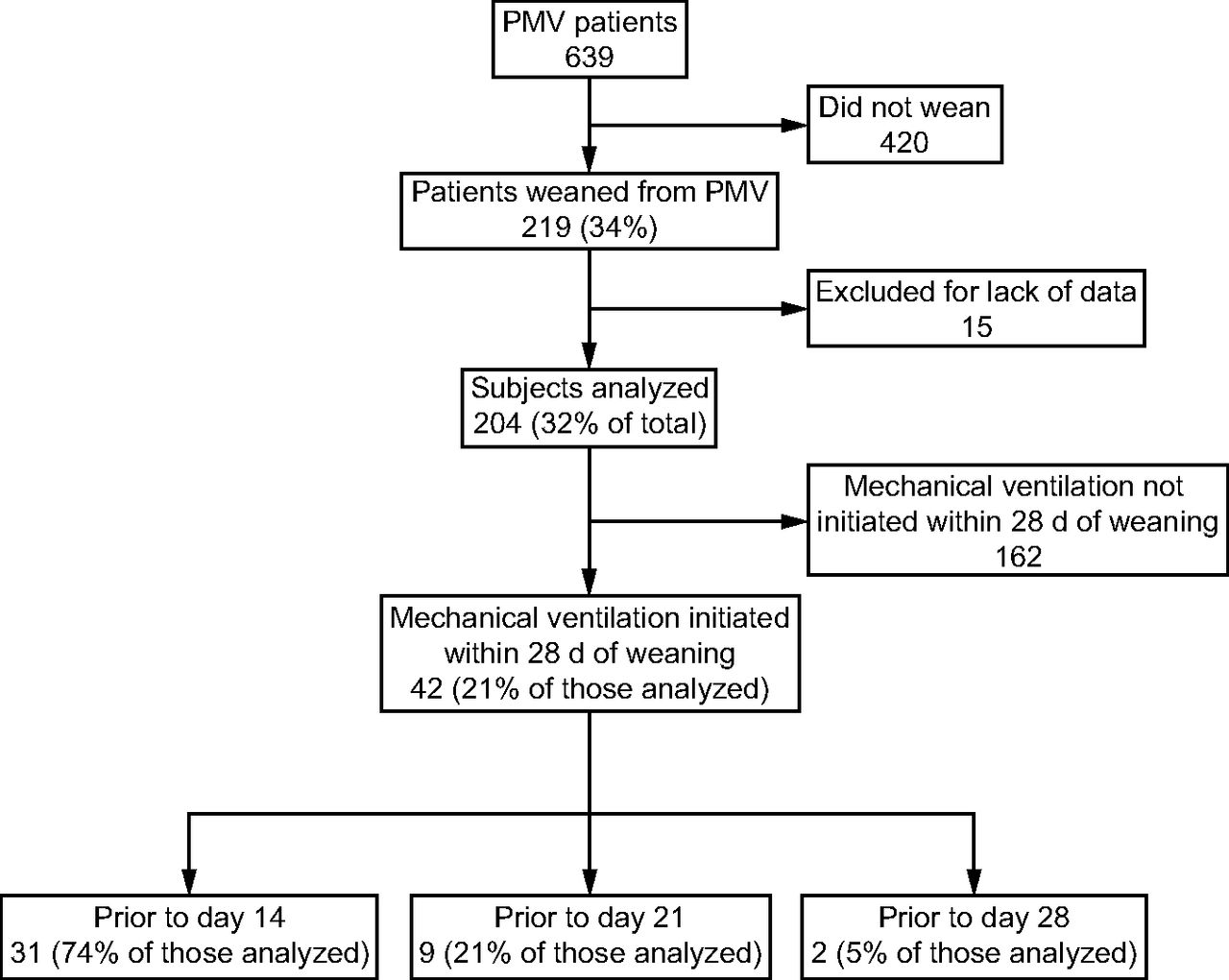
Flow chart. PMV = prolonged mechanical ventilation.
Characteristics of the Study Sample
Reasons for reinstitution of mechanical ventilation included sepsis (27 subjects), heart failure and acute pulmonary edema (4 subjects), structural airway alterations (4 subjects), hypercapnia (3 subjects), atelectasis and respiratory failure (2 subjects), tracheostomy cannula obstruction (1 subject), and clinical judgment of the physician on call (1 subject).
Univariate and multivariate binary logistic regression analyses are shown in Table 2 and Table 3, respectively. In the multivariate logistic regression analysis, neurological comorbidity (adjusted odds ratio 5.1 [95% CI 2.3–11.1], P < .001), and delayed weaning (adjusted OR 2.37 [95% CI 1.1–5.3], P = .035) were statistically significant. The regression model showed a correct classification power of 80% regarding the events in the response variable.
Univariate Logistic Regression Analysis
Multivariate Binary Logistic Regression Analysis
Both the calibration measured through the Hosmer-Lemeshow test (P = .98) and the model discriminatory power were adequate (area under the curve = 0.714 [95% CI 0.626–0.803], P < .001).
An analysis of the risk for reinstitution of mechanical ventilation was performed based on the presence or absence of variables that were statistically significant in the logistic regression analysis (Table 4). In the analysis of interaction between risk factors, a synergy index of 5.35 (95% CI 2.4–11.4) was obtained between neurological comorbidity and delayed weaning.
Probability of Mechanical Ventilation Reinstitution Within 28 d of Weaning
Discussion
Based on the need to define the duration of the weaning process that best predicts long-term success and as recommended by the consensus conference, study subjects were followed up for 28 d after liberation from mechanical ventilation. Re-establishment of mechanical ventilation before day 28 occurred in a considerable proportion of subjects, with the greatest number of subjects being reconnected before the second week. Given that various investigators use differing definitions for weaning success, the question that arises is whether the weaning success threshold should be changed from 7 d to 14 d, thus reducing the number of patients who would require reinstitution of mechanical ventilation within 28 d of weaning from 21% (42 subjects) to 5% (11 subjects).
An interesting view on this topic is that provided by Thille et al,19 who proposed identifying whether reintubation is secondary to weaning failure or to a new event. In this respect, we noted that sepsis was the most common reason to reinstitute mechanical ventilation, which could be considered a result of a new event rather than failure of the weaning process itself; however, whether infection was a new event or part of the underlying condition of chronic critically ill patients could not be determined with certainty. Taking these data into account, it seems unnecessary to extend the 7-d threshold to consider that a patient on PMV has been successfully weaned.
Ruan at al15 analyzed the clinical course of subjects requiring more than 48 h of mechanical ventilation with the use of Taiwan's National Health Insurance database. For subjects who were weaned from PMV, the probability of reinstituting mechanical ventilation was found to decrease over the first 7 d (25%, 8%, 3%, 3%, 2%, 1%, and 1% for the initial 7 d, respectively). The authors concluded that the probability curve reaches a stable level on the fifth day, suggesting that a 5-d ventilator-free period could be an appropriate criterion to define weaning success in this population. However, reasons for reinstitution of mechanical ventilation and associated risk factors were not reported.
Schönhofer et al10 suggest considering not only a time-based criterion (which can be misleading) but also the patient's clinical stability after weaning (ie, absence of hyperthermia, stable hemodynamics, conscious and cooperative patient, and good management of secretions). Clinical instability after weaning was associated with increased mortality, although the need to reinstitute mechanical ventilation in weaned unstable patients is not specified. It should be noted that mortality in our institution was higher and statistically significant in subjects who required reinstitution of mechanical ventilation, although it is unclear whether this was the only factor differentiating both groups.
In our multivariate logistic regression analysis, neurological comorbidity and delayed weaning (ie, after 7 d of admission to the weaning and rehabilitation center) were linked to a higher risk for reinstitution of mechanical ventilation. Predictive performance of these factors indicates that the presence of both neurological comorbidity and delayed weaning substantially increases the likelihood of reestablishment of mechanical ventilation. Interaction between them is synergistic and multiplicative (synergy index > 1), which shows the need for greater caution in weaning patients with both factors. The subgroup of patients who, apart from the event leading to ICU admission, presents with neurological comorbidity is likely to be in a worse general condition and at greater risk for complications, such as aspiration due to a swallowing disorder. With regard to weaning, in concordance with what was reported in a previous study,5 a great number of patients are weaned within the first days of admission to a weaning and rehabilitation center (IQR 25% of the patients were weaned on the fifth day of admission); we can now add that those not weaned within 7 d are at greater risk for reinstitution of mechanical ventilation.
Our study has some limitations. First, it was a retrospective study that relied on clinicians entering the appropriate data in the chart; therefore, despite the reliability of our records, 15 subjects were excluded due to a lack of data regarding the date of mechanical ventilation and/or the reason for mechanical ventilation reestablishment. Moreover, this was a single-center study. However, we believe that our results have external validity because study subjects are representative of a traditional weaning and rehabilitation center.
Because the consensus criterion of 7 d with no ventilatory support is not consistently used,2 the definition of PMV weaning success as described in the study by Rose et al16 should be validated through multi-center studies specifically designed for this purpose. We believe that our study provides important data for future research on the topic.
Conclusions
A clear definition of successful weaning allows the assessment of protocol efficacy, a more accurate estimation of mechanical ventilation outcomes, and comparisons across centers. In our study, reinstitution of mechanical ventilation within 28 d of weaning in subjects considered successfully weaned was a common event: 1 in 5 of these subjects required the reinstitution of mechanical ventilation, with sepsis being the most prevalent cause. Neurological comorbidity and delayed weaning are risk factors associated with the reinstitution of mechanical ventilation. The presence of more than one risk factor increases the association with reestablishment of mechanical ventilation within 28 d of weaning.
Footnotes
- Correspondence: Darío Villalba PT, Clínica Basilea, Solís 1025, C1078AAU, Buenos Aires, Argentina. E-mail: dario.villalba{at}clinicabasilea.com.ar.
Mr Gil Rossetti presented a version of this paper at the 27th Argentine Congress of Intensive Care, August 30 to September 3, 2017, Córdoba, Argentina.
The authors have disclosed no conflicts of interest.
- Copyright © 2020 by Daedalus Enterprises





{kind=link}