

Abstract
BACKGROUND: We previously reported a new management variable, work rate, defined as work load due per hour, based on cumulative standard treatment times. We found that work rates were unachievable (ie, exceeded 1 hour of scheduled work per hour of available labor) for 75% of scheduled due times, despite presumed achievable average work load.
OBJECTIVE: To determine the optimal strategy for creating work assignments based on work rate.
METHODS: A focus group used root-cause analysis to identify ways to balance assignments based on work rate. We surveyed employees to assess their willingness to start earlier. We determined the ratio of scheduled to unscheduled work during a 12-month period. The scheduled work comprised administering small-volume nebulizer, metered-dose inhaler, noninvasive ventilation, and mechanical ventilation. The unscheduled work consisted of all other modalities. We also developed a spreadsheet model to assess the effect of shifting the start time on work-rate distribution in a representative 24-hour period.
RESULTS: The focus group determined that starting treatments 1 hour earlier would help. Fifteen of the 24 clinicians surveyed responded, and 13 of the respondents were willing to start earlier. The scheduled work load averaged approximately 55% of the total work load, but there was high variability per assignment area (range 0–99%). The spreadsheet model showed that shifting treatment start times improved the distribution of work rate throughout the day, but did not guarantee that labor demand never outstrips supply.
CONCLUSIONS: Our studies to date suggest that: basing assignments on average work load leads to periods of unachievable work rate, resulting in missed treatments and staff dissatisfaction. We have only limited ability to reduce peaks in work rate, but staggering treatment times is effective. Fair assignment of work should differentiate scheduled from unscheduled work.
Introduction
Current strategies for distributing work load in respiratory care departments, which are based only on the volume of therapies and the available staff, are time-honored but problematic.1 The traditional strategies can create staffing challenges, missed therapies, and dissatisfaction. We developed the concept of work rate to enhance work assignment. The 2 main goals of work-rate-based work assignment are to enhance the allocation of respiratory therapy (RT) services and to assure the timely delivery of ordered therapies. Work rate is defined as work load that is due per hour, based on cumulative standard treatment times.
We previously reported a pilot study of work rate2 in which we found that day and evening shifts have some treatment due times with unachievable work rates (based on a maximum work rate of 1.0 scheduled hours of work per 1.0 hour of available time per worker). The findings suggested that to assure equal distribution of work load and the timeliness of delivered treatments, assignments should be based on work rate, not work load. In a subsequent study we found that work rates were unachievable with available staff for 75% of scheduled due times, despite presumed achievable average work load. We concluded that work-assignment practices that are common to the profession are based on questionable assumptions, and this invites a new approach, such as that based on work rate. The purpose of the current study was to determine the optimal strategy for creating work assignments based on the work rate variable.
Methods
The study was deemed exempt from review by the Cleveland Clinic institutional review board, as it was considered a quality-improvement project.
To help generate ideas and plan an initial approach, we convened a focus group of key RT staff and other content experts within the Cleveland Clinic (eg, process-improvement and operations-research experts) and used root-cause analysis methods to clarify how to create a schedule based on work rate. The group felt that starting scheduled treatments 1 hour earlier in the day shift would help. Clinical staff were then surveyed (see the supplementary materials at http://www.rcjournal.com) to determine their willingness to work modified shifts to accommodate altered treatment start times.
The work-rate metric is based on standard durations for procedures that are scheduled (by physician order) to be delivered at particular times of the day. Our standard treatment durations were based on our own time/motion studies and data from the American Association for Respiratory Care Uniform Reporting Manual.3 We collected 12 months of data with a custom program that we designed in data-collection software (Crystal Reports, SAP Crystal Solutions, Newtown Square, Pennsylvania) to query our hospital's database (MediLinks, MediServe, Chandler, Arizona) to determine the ratio of scheduled to unscheduled work.
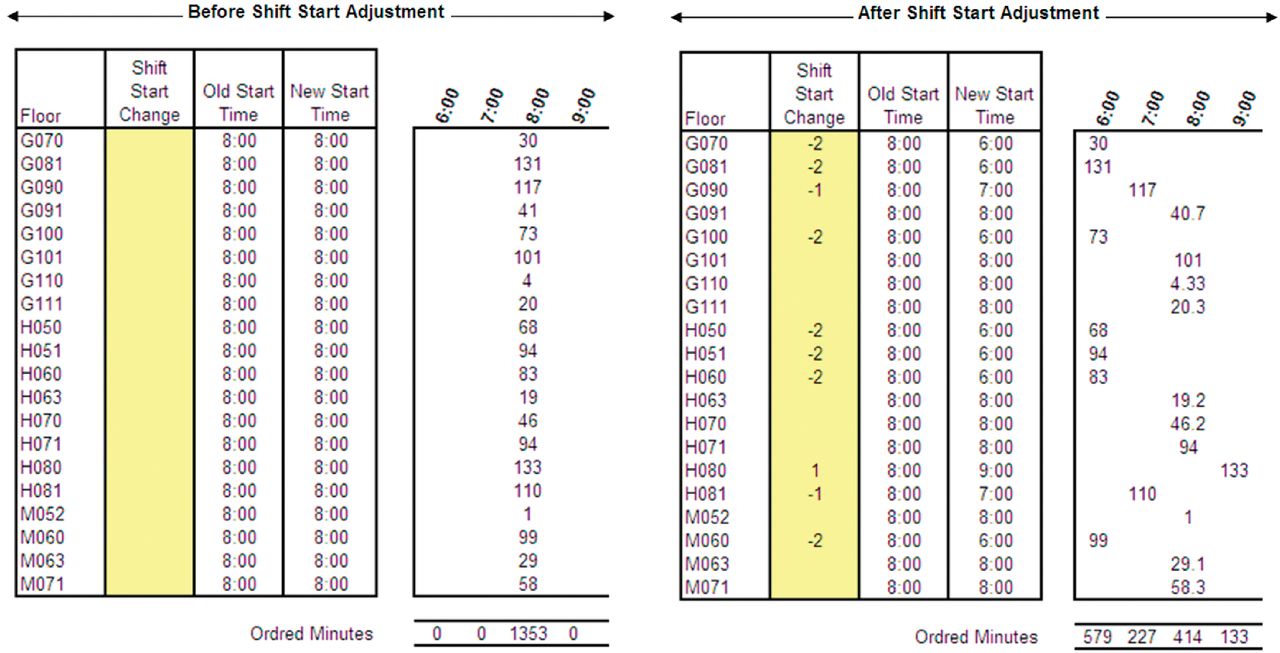
We developed a spreadsheet (Excel, Microsoft, Redmond, Washington) to assess the effect of shifting the start time on work-rate distribution in a representative 24-hour period. The spreadsheet was linked to the data-collection software such that the scheduled work due per hour could be represented by assignment area (hospital floor). The spreadsheet allowed adjustment of shift start times (eg, +1 or –2 hours) for “what if” analysis of the effects on hourly work rate. Figure 1 shows a representative day with a normal shift start time of 7:00 am on the left. With conventional work load scheduling, the result was that the work rate for 8:00 am was 1,353 min, which was unachievable because the available staff could provide only 420 min of work at 100% efficiency. However, after adjusting the start times on different floors by +1 or −2 hours, the work rate was distributed more evenly between 6:00 am and 9:00 am (see Fig. 1 right panel).

A portion of the spreadsheet model, showing work load by floor for each hour of the day. Before adjusting the shift start time (left) the work rate due at 8:00 am was 1,353 hours. After adjusting the start times the work rate was distributed more evenly between 6:00 am and 9:00 am.
We also analyzed how a standard assignment should be partitioned into scheduled (actually ordered at the time of making the assignment) versus unscheduled work. Scheduled work comprised small-volume nebulizer, metered-dose inhaler, noninvasive ventilation, and mechanical ventilation. Unscheduled work comprised all the other modalities.
Results
We surveyed 24 clinicians, of whom 15 responded, and 13 were willing to start earlier. The spreadsheet model demonstrated that a typical day could have unachievable work-rate peaks with the traditional work-assignment technique (Fig. 2). For the representative day shown in Figure 1, assuming 100% staff working efficiency, 44% of the ordered work load was unachievable with a conventional work-assignment model. For example, at 8:00 am the work rate was 1,353 ordered hours per hour of staffing (see the total ordered minutes in the 8:00 am column in Fig. 1). After adjusting the treatment start times (Fig. 3), only 5% of the ordered work load was unachievable, and the work rate at 8:00 am was only 414 ordered hours per hour of staffing, because the ordered work was distributed among 3 hours (6:00 am, 7:00 am, and 8:00 am). We recognize that the assumption of 100% efficiency is simplistic and probably overestimates the achievement of work-load assignments.
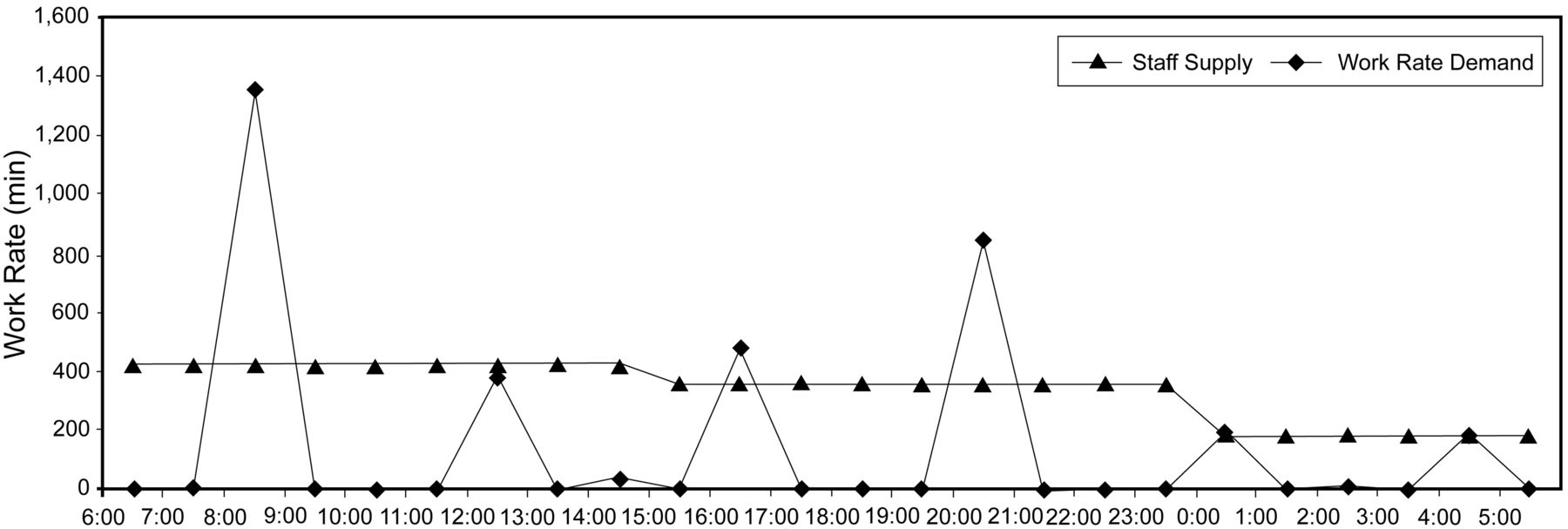
Work due per hour (work rate) on a representative day, before shift start-time adjustments. The work rate is unachievable at 8:00 am, 4:00 pm, and 8:00 pm.
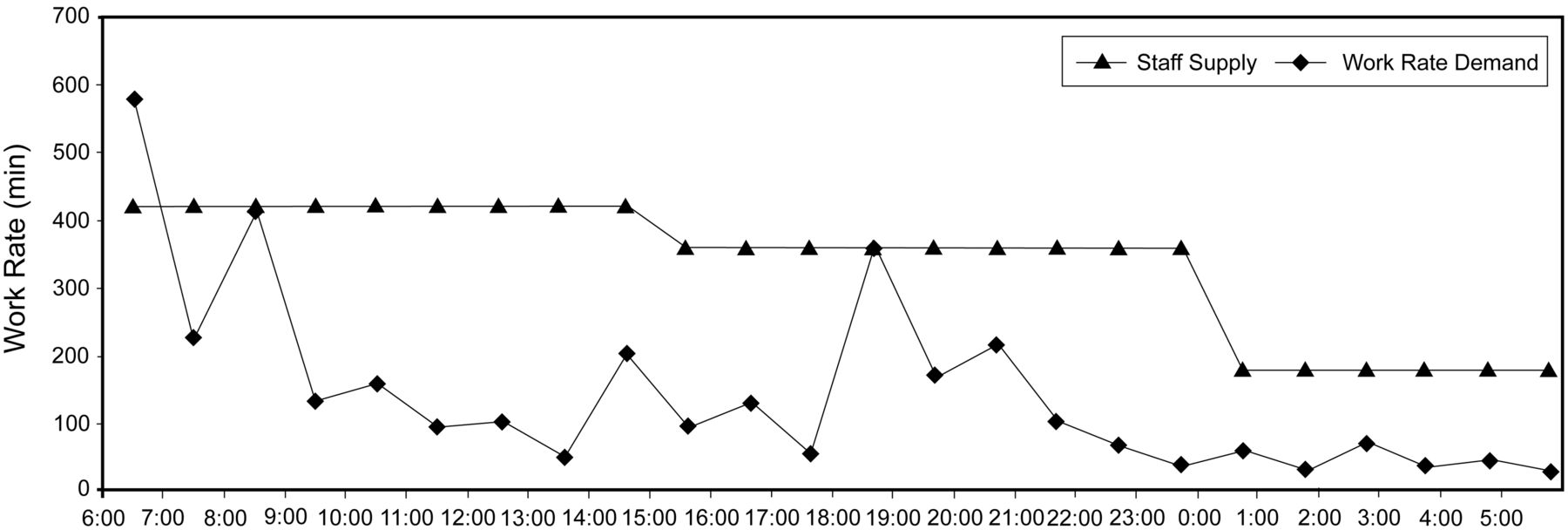
Work due per hour (work rate) on a representative day, after shift start-time adjustments. The work-rate distribution is much more favorable than in Figure 3, and is only unachievable at 6:00 am.
Our analysis across all assignment areas indicated that, on average, scheduled work composed 55% of the total work load (Table 1), and there was high variability per assignment area as indicated by the percentile plot (Fig. 4), which may have implications for improving work assignment. For example, Figure 1 shows that some areas had 100% unscheduled work, which suggests that those areas might be best covered by a float assignment rather than a fixed therapist assignment.
Analysis of Scheduled Versus Unscheduled Workload for 12 Months
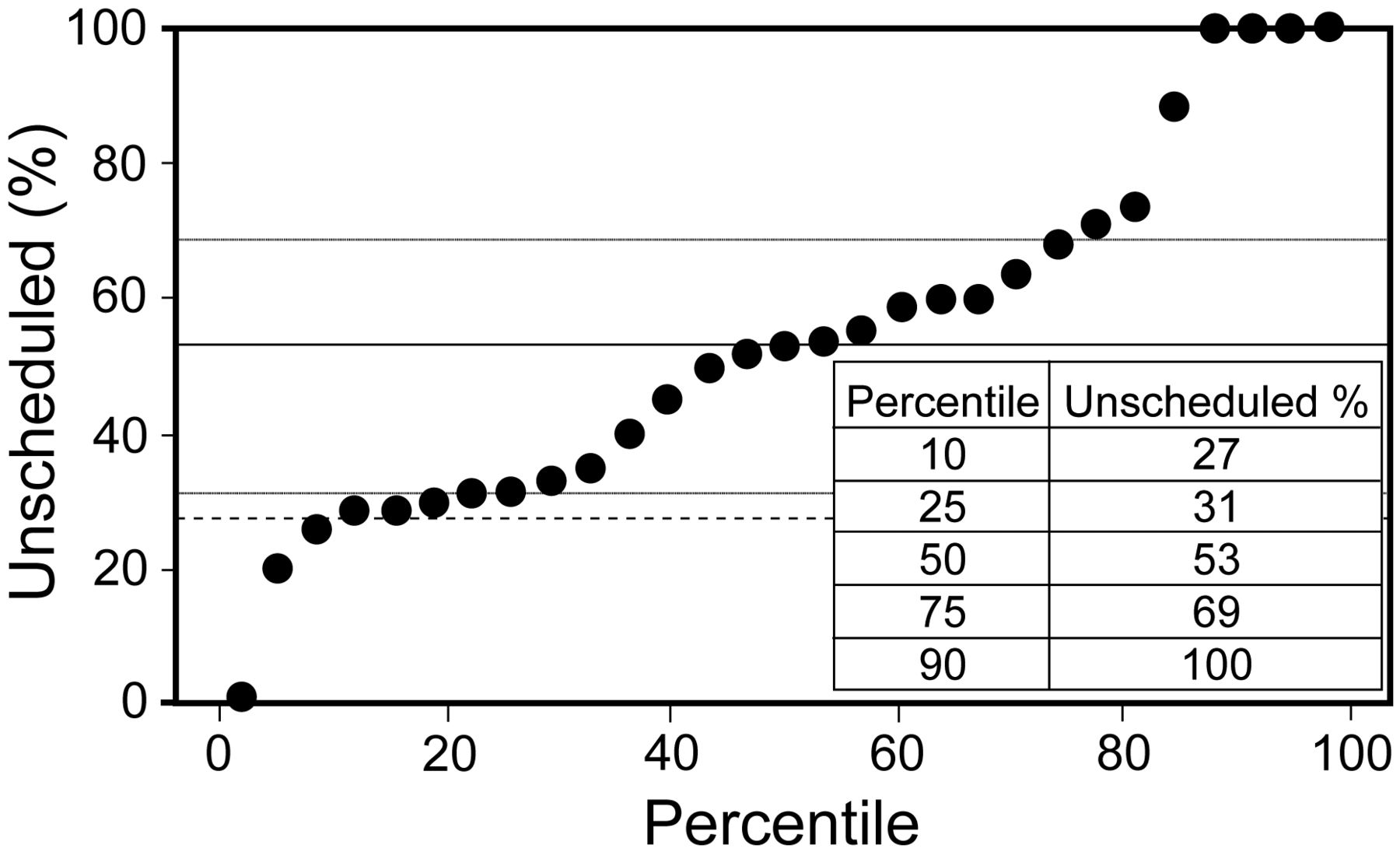
Percentile plot of unscheduled work, across all assignment areas. The horizontal lines indicate the 10th, 25th, 50th, 75th, and 90th percentiles.
Discussion
A recent literature review found that decreased nurse staffing is associated with adverse outcomes in intensive care unit patients.4 There are also data to suggest that there is an association between staffing and teamwork. The higher the perception of the adequacy of staffing and the fewer patients cared for on a previous shift, the higher the teamwork scores.5 However, little is available in the literature regarding how staffing matches work load variability in healthcare. One study of nursing practice used process-control theory to define appropriate staffing levels as those that exceeded predefined rates within acceptable and tolerable limits (50% and 80%, respectively).6 That study found that work load was acceptable 42% of the time and tolerable 71% of the time. Appropriate staffing based on work load was achieved only 45% of the time.
Traditionally, nursing schedules are determined without knowing the imbalances in work load.7 Part of the challenge to improving work assignment may simply be an inability to track work load. In a related sense, nursing has struggled with creating standardized nursing intervention terminologies for use in electronic health records.8 While the respiratory care profession is just beginning to address this issue,9 respiratory care has a fully developed system for reporting treatment times,3 which is an invaluable resource for measuring and documenting work load and hence work rate.
A novel data-mining and simulation approach to evaluate patient-to-nurse assignments ahead of nursing shifts has been proposed by Sundaramoorthi et al.10 Our study applies a similar concept, with a different method, to respiratory care. To our knowledge, it is the first to propose the concept of work rate in respiratory care. We focused on the new variable, instantaneous work rate, instead of average work load as a potential new strategy by which to make RT staffing assignments. This approach has provided insights regarding the limits of current staffing models and opportunities to improve staffing to optimize timely delivery of RT services.
Our practice has been to assign each staff member 300 min of work in a 480-min (8-hour) shift. This assumed that 63% (300/480) of the work load was scheduled (currently ordered) and 37% was unscheduled or wasted (eg, travel time), based on time/motion studies at our institution. However, our current data suggest a larger portion of unscheduled work (45%). Therefore, individual work assignments should be based on an average scheduled work load, which is 264 min (55% of 480 min). Thus, if a therapist is assigned 264 cumulative minutes of scheduled work in particular areas of the hospital, it is understood that the therapist will also be responsible for the unscheduled work that arises in those areas. Given the high assignment-area variability in scheduled versus unscheduled work in various work-assignment areas, it is clear that work assignments should be based on actual daily data. Other main findings and implications of this preliminary analysis are that:
Basing assignments on average work load leads to periods of unachievable work rate, potentially causing missed treatments and staff dissatisfaction.
Given current technology and traditional work-assignment practices, the ability to meet work peaks is limited, but it appears that staggering treatment times can help.
Fair work assignments based on average work load should differentiate between scheduled and unscheduled work.
Our spreadsheet model showed that shifting treatment start times improved the distribution of work rate throughout the day, but this measure alone will not guarantee that labor demand never outstrips supply. Other methods of reducing work load, particularly unnecessary work load, should be explored (eg, protocols driven by therapist-initiated patient assessment). Once such measures are in place there may be little gained from daily treatment-time adjustments. However, the tool still has utility if used to review retrospective data (ie, at the end rather the beginning of the day) to see the effects of both treatment time redistribution and actual unscheduled work. Such analyses may provide ideas for further refinement of assignment practices.
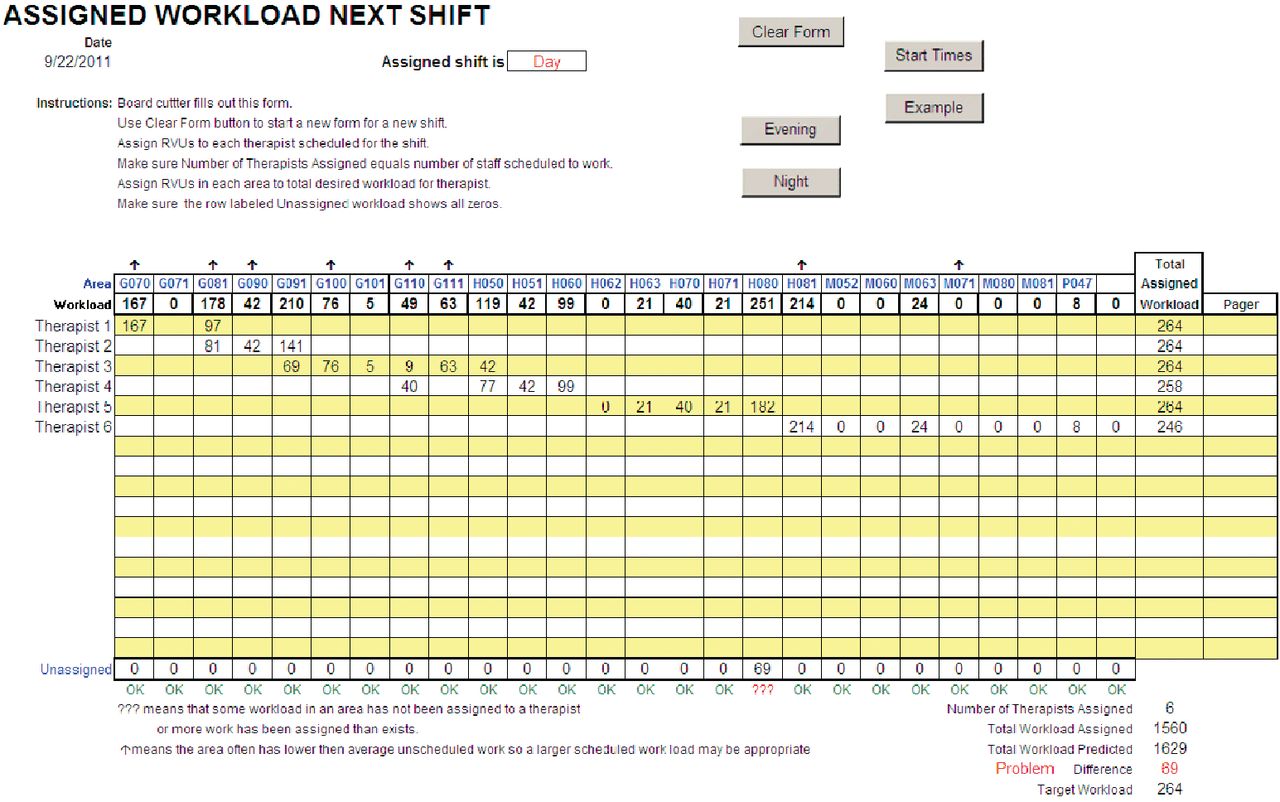
A product of this analysis was our spreadsheet work-assignment tool (Fig. 5), which is linked to the hospital's MediLinks database. The spreadsheet can be automatically populated with assignment-area work loads, allowing the RT supervisor to easily and efficiently assign work load in geographically proximate areas to achieve an appropriate average scheduled work load (264 min in the current case). This strategy greatly reduces the time required to assign work. For example, the assignments in Figure 5 were made in less than 5 min and required no special training or experience. One of us (RLC) had developed and used this tool successfully in another hospital, without a link to a work-load database. Instead, the tool was linked to another spreadsheet that was populated by asking staff from the previous shift to estimate the number of treatments of each type they expected for the next shift in each assignment area. Those treatment volumes were then automatically converted to work loads, using standard treatment times, and the resulting area work loads were automatically ported to the work-assignment tool.

Work-assignment tool implemented in a spreadsheet. Work load in each area is accumulated to achieve a scheduled work load of approximately 264 minutes. Areas with zero scheduled work load are nevertheless assigned to specific therapists so that any unscheduled work that arises will be accommodated. Note that the tool indicates that 69 minutes of scheduled work are still unassigned for work area H080. This indicates that the work in that area must be shared with another therapist.
Limitations
First, our results depend heavily on the standard treatment times we used, which were a mixture of times from the American Association for Respiratory Care Uniform Reporting Manual3 and our own data from the Cleveland Clinic. Thus, while we are confident that these treatment-time standards accurately reflect needs in our setting, their generalizability will require replication by others in different settings.
Also, a potential impediment to others adopting work-rate-based assignment is that the data on ordered therapies must be available quickly and conveniently in electronic form, which generally requires a management information system (eg, MediLinks) that facilitates RT work assignment. Developing the Crystal Reports data-collection interface between MediLinks and Excel required approximately 40 hours of custom programming.
Finally, our findings are preliminary; further work is needed to validate the concept of work rate as a method for assigning RT work. For example, future study must establish in actual practice settings (or in a cohort study) that work-rate-based assignment is effective. Specifically, can work assignments be made more easily and in less time? Does work-rate-based assignment improve the timeliness of treatments? Does work-rate-based assignment affect clinical outcomes? And is RT staff satisfaction improved? Our work-rate assignment concept and the software we developed for this study provide a basis for those future studies.
Conclusions
This preliminary study suggests that making RT work assignments based on work rate offers potential benefits. Further study and validation are needed.
Footnotes
- Correspondence: Robert L Chatburn RRT-NPS FAARC, Respiratory Therapy, M-56, The Cleveland Clinic, 9500 Euclid Avenue, Cleveland OH 44195. E-mail: chatbur{at}ccf.org.
-
Mr Chatburn presented a version of this paper at the 56th International Respiratory Congress of the American Association for Respiratory Care, held December 6–9, 2010, in Las Vegas, Nevada.
-
Mr Chatburn has disclosed relationships with IngMar, Hamilton, Covidien, and Dräger. The other authors have disclosed no conflicts of interest.
-
Supplementary material related to this paper is available at http://www.rcjournal.com.
-
See the Related Editorial on Page 1864
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}