

Abstract
BACKGROUND: In general emergency departments, advanced airway management of pediatric patients who are critically ill has been associated with increased adverse events given the varying exposure to pediatric patients and limited resources. Previous studies have shown significant improvement of simulated pediatric airway management in general emergency departments. The aim of this retrospective study was to determine the effect of an in situ simulation-based collaborative intervention program on the actual care of pediatric airway management in general emergency departments.
METHODS: This was a retrospective study of pediatric subjects who were critically ill and required intubation at a diverse set of general emergency departments before referral to the academic medical center. The primary outcome was the quality of clinical care measured by adherence to best practices via a critical action checklist. Secondary outcomes included tracheal intubation associated adverse events and clinical outcomes.
RESULTS: A total of 135 pediatric subjects (48 pre- and 87 post-intervention) who were transferred to the academic medical center from 9 general emergency departments between May 2014 and August 2019 were included in the analysis. The use of a cuffed endotracheal tube improved, from 44% to 72% (P = .001), whereas there was no significant change in the appropriate endotracheal tube size. Overall, severe tracheal intubation associated adverse events decreased, from 18.8% to 9.2% (P = .03), and post-intubation cardiac arrest events decreased, from 6.3% to 0% (P = .02).
CONCLUSIONS: A simulation-based collaborative intervention program led to improvement in pediatric airway management and subject outcomes in general emergency departments. This model demonstrated the transfer of improvement from a simulated setting to a clinical setting and may be targeted in other clinical settings.
Introduction
Pediatric advanced airway management is a challenging and potentially life-threatening procedure that is frequently associated with adverse events, particularly in unprepared settings.1 The anatomic and physiologic characteristics of pediatric airways differ from those of the adult airway and contribute to an increased frequency of adverse events compared with adults.2 Ninety percent of children who are acutely ill and children who are injured initially present to general emergency departments, where advanced airway management is sometimes needed.3 These general emergency departments are less prepared to care for children who are critically ill given their lower pediatric patient volumes and lack of pediatric resources and expert personnel.4,5
There are national data of a wide range of tracheal intubation-associated adverse events, ∼20%, and certain tracheal intubation associated adverse events, such as esophageal intubation or mainstem bronchial intubation, are more commonly seen in general emergency departments than in pediatric tertiary centers.6-8 Furthermore, deviations from best practices, for example, the use of uncuffed tracheal tubes, were noted in most children transferred from general emergency departments to pediatric centers.6 These variations in practice and process of care between general emergency departments and pediatric centers have resulted in disparities in patient outcomes, in which children with respiratory failure who presented to lower-volume general emergency departments had higher odds of mortality compared with higher-volume pediatric emergency departments.9
To address these gaps in the general emergency department setting in the United States, several state and national initiatives have been implemented to improve the process of care provided to children who are acutely ill and those who are injured. Examples include the National Pediatric Readiness Project established by the Emergency Medical Services for Children to ensure that all United States emergency departments have essential resources, guidelines, and equipment to provide high-quality care to children.4 Most recently, the implementation of an airway safety bundle across a network of pediatric emergency departments and urgent care sites has resulted in a decrease in severe tracheal intubation associated adverse events in participating sites.10 In parallel, we previously reported a collaboration program between our pediatric academic medical center and a group of general emergency departments statewide.11-15 This collaboration, through in situ simulation, education, and quality improvement, aimed to optimize pediatric emergency readiness and quality of care provided in general emergency departments. Participating general emergency departments demonstrated significant improvement in the process of care provided to children in acute care scenarios, including advanced airway management in a simulated setting.12 However, little is known about the impact of our collaborative program on the process of clinical care provided in participating general emergency departments and patient outcomes.
The primary aim of this retrospective study was to examine the effectiveness of a collaborative intervention program in improving pediatric advanced airway management in patients presenting to participating general emergency departments. The secondary aim was to assess the impact of our intervention on subject outcomes. We hypothesize that participation in our collaborative program will be associated with improvement in the process of advanced airway management, as demonstrated by a critical action intubation checklist, in addition to improvement in patient outcomes.
QUICK LOOK
Current Knowledge
A collaborative intervention program can improve the quality of simulated pediatric airway management in general emergency departments. It remains unclear whether this simulation-based improvement is associated with improvements in actual patients’ clinical care downstream.
What This Paper Contributes to Our Knowledge
This study demonstrated the translation of simulation-based improvements in some elements of clinical care as revealed by the improvement in adherence to pediatric airway management best practices in a set of general emergency departments.
Methods
Study Design and Subject Population
This study was a retrospective cohort analysis that was conducted at Riley Hospital for Children at Indiana University Health. The Indiana University’s institutional review board reviewed and approved the study. Riley Hospital is the only pediatric academic medical center in the state of Indiana, with 316 pediatric beds, including 36-bed medical-surgical pediatric ICU. Inclusion criteria were all pediatric subjects < 18 years of age who required advanced airway management, that is, placement of an endotracheal tube (ETT), performed by a participating general emergency department provider before transfer to the Riley Hospital pediatric ICU by the Indiana University Health transport team between 2014 and 2019. The exclusion criteria were patients who were intubated by the Indiana University Health transport team or at Riley’s emergency department, patients who needed other types of advanced airway management (including tracheostomy, laryngeal mask airway, or laryngeal tube), patients who were intubated during the intervention period, and the patients who died in general emergency department before transfer to academic medical center pediatric ICU. The timeline of intervention and data collection is shown in Supplementary Figure 1 (see the supplementary materials at http://www.rcjournal.com).
Collaborative Intervention Program
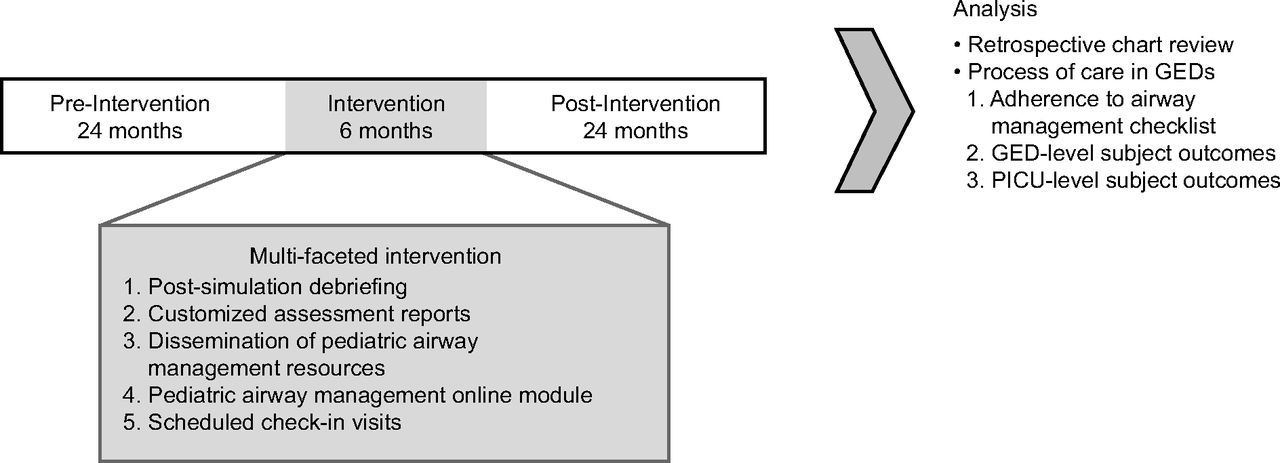
This program involved an academic medical center that works with a set of general emergency departments across the state of Indiana to improve the quality of care for children who are acutely ill. The multifaceted intervention was guided by a multi-professional team of experts in pediatric emergency medicine, pediatric critical care medicine, pediatric critical care transport nursing, and pediatric respiratory therapy from Riley Hospital for Children at Indiana University Health. Each participating general emergency department designated a pediatric champion who functioned as a pediatric emergency care coordinator to help implement and execute the program’s components. The multifaceted collaborative intervention extended over 6 months and is detailed in our previous publications.11,12 Briefly, it included the following phases: (1) pre-intervention assessment of inter-professional team performance in a simulated setting; (2) a multifaceted intervention phase that consists of post-simulation debriefing, customized assessment reports (including the team's performance and areas of improvement), dissemination of pediatric airway management best practices and clinical resources in the general emergency department setting, pediatric airway management online module, and scheduled check-in visits at 2 months and 4 months; and (3) post-intervention assessment, repeated measurement of simulation-based performance of all participating general emergency departments (Fig. 1).

The multifaceted intervention program model. GED = general emergency department; PICU = pediatric ICU.
Data Collection
Airway management data were collected by a retrospective chart review of paper documentation of medical records from general emergency departments handed to the transport team at the time of transport and from transport team documentation. The documentation was scanned into the academic medical center electronic medical records (Cerner Corporation, North Kansas City, Missouri). Pediatric ICU outcome measures were collected from the academic medical center electronic medical records and virtual pediatric ICU systems (VPS, Los Angeles, California). One of the authors (MM) collected all the data and was blinded to the intervention period for all general emergency departments.
Outcome Measures
The primary outcome measure was the process of care provided in participating general emergency departments as assessed by the critical action checklist items used during in situ simulation that were feasible to collect from a chart review.12 These included medications used for sedation and neuromuscular blockade to facilitate intubation, the number of intubation attempts, ETT size and type (cuffed vs uncuffed), and ETT insertion depth. Appropriate ETT size was defined per the 2010 American Heart Association Pediatric Advanced Life Support guidelines,16 in which a deviation of 0.5 mm above or below the recommended size was still considered the appropriate size. The appropriate ETT depth was defined by using the same guidelines, in which deviations of 0.5 cm above or below the recommended depth were still considered the appropriate depth.
General emergency department and pediatric ICU subject outcomes were used as secondary outcomes. General emergency department-level subject outcomes were assessed by using the incidence of adverse tracheal intubation–associated events classified as severe and non-severe events.17 We included only cardiac arrests that occurred after intubation in a general emergency department and before transfer to an academic medical center. Hypoxemia was defined as  < 90%. Pediatric ICU-level subject outcome data included ETT exchange by academic medical center teams, post-extubation upper-airway obstruction (defined as development of stridor, use of racemic epinephrine or heliox), extubation failure (defined as the need for re-intubation within 48 h of extubation), the need for new tracheostomy during hospital admission, duration of mechanical ventilation, pediatric ICU length of stay, hospital length of stay, and mortality.
< 90%. Pediatric ICU-level subject outcome data included ETT exchange by academic medical center teams, post-extubation upper-airway obstruction (defined as development of stridor, use of racemic epinephrine or heliox), extubation failure (defined as the need for re-intubation within 48 h of extubation), the need for new tracheostomy during hospital admission, duration of mechanical ventilation, pediatric ICU length of stay, hospital length of stay, and mortality.
Statistical Analysis
Descriptive statistics were used, and data were summarized as numbers (%) or medians (25th – 75th percentiles). Pre- and post-intervention variables were compared by using the Wilcoxon rank-sum test for continuous variables and the chi-square test or the Fisher exact test for categorical variables. All statistical analyses were performed by using Stata Statistical Software Release SAS 9.04 (SAS Institute, Cary, North Carolina). P < .05 was considered statistically significant.
Results
General Emergency Departments and Subject Demographics
Nine general emergency departments in the state of Indiana participated in the collaborative intervention program. Three (33.3%) had a medium annual pediatric volume (1,800–4,999), and 6 (66.7%) had a medium-to-high annual pediatric volume (5,000–9,999). Eight general emergency department hospitals (88.9%) had in-patient pediatric units (pediatric ward or neonatal ICU). The median (interquartile range) distance of general emergency departments from the state academic medical center was 53 (23.9–66.9) miles. Three of these general emergency departments (33.3%) were affiliated with the academic medical center.
Overall, 207 pediatric patients on mechanical ventilation were transferred to the academic medical center pediatric ICU between 2014 and 2019 from the 9 general emergency departments. Of these, 135 pediatric patients who were intubated met the inclusion and exclusion criteria: 48 subjects in the pre-intervention period and 87 subjects in the post-intervention period (Supplementary Fig. 2 [see the supplementary materials at http://www.rcjournal.com]). There was no statistically significant difference in the demographics between the pre-intervention group and the post-intervention group except in race and/or ethnicity. The most common reasons for intubation were respiratory illnesses, mostly secondary to lower airway disease, seizure, and toxin and/or poison. Subject demographics and primary diagnosis are shown in Table 1.
Subject Demographic and the Primary Diagnosis
Quality of Pediatric Advanced Airway Management in General Emergency Departments
The use of cuffed ETT significantly improved, from 43.8% to 72.4% (P = .001) (Fig. 2A). The increase in cuffed ETT use was noted in respiratory, seizure, trauma, and toxin and/or poison subjects but did not reach statistical significance (Supplementary Table 1 [see the supplementary materials at http://www.rcjournal.com]). The appropriate ETT size changed, from 66.7% in the pre-intervention group to 79.3% in the post-intervention group, but did not reach statistical significance (P = .16) (Fig. 2B). There was still a high percentage of ETTs that were inserted too deep in both groups, with 72.9% in the pre-intervention group compared with 69.0% in the post-intervention group (P = .57) (Fig. 2C).

Changes in endotracheal tube (ETT) utilization pre- and post-intervention. A: ETT type; B: ETT size; and C: ETT depth.
The most common sedative medications used in both groups were midazolam, etomidate, fentanyl, and ketamine. At least one neuromuscular blocking agent was used in 37 of 48 subjects (77.1%) in the pre-intervention group compared with 59 of 87 subjects (67.8%) in the post-intervention group (P = .26). The decrease of neuromuscular blocking agent use was noted in subjects with seizure, trauma, and toxin and/or poison, but none of these changes reached statistical significance. Most subjects were intubated from the first or second attempt, whereas 5 of 48 (10.4%) and 14 of 87 (16.1%) required ≥3 intubation attempts pre- and post-intervention, respectively (P = .64). Medications used for airway management in general emergency departments in addition to the number of intubation attempts are shown in Table 2.
Medications Used for Airway Management in General Emergency Departments
General Emergency Departments and Pediatric ICU–Level Subject Outcomes
There was a decrease in the severe tracheal intubation associated adverse events from 9 of 48 (18.8%) in the pre-intervention group to 8 of 87 (9.2%) in the post-intervention group (P = .03), with a significant decrease in the post-intubation cardiac arrest events for subjects who survived, from 3 of 48 (6.3%) to 0 of 87 (0%) (P = .02). Non-severe tracheal intubation associated adverse events were similar between the groups: 60.4% versus 49.4% pre- and post-intervention, respectively. The most common non–severe tracheal intubation associated adverse events identified was right main stem intubation, with a 31% incidence in the pre-intervention group compared with 21% in the post-intervention group. The second most common non-severe tracheal intubation associated adverse event was pain and/or agitation, which occurred in 21% in the pre-intervention group compared with 16% in the post-intervention group (Table 3). Sinus tachycardia and hypoxemia frequently occurred in both groups. When compared with the pre-intervention group, the subjects in the post-intervention group had similar ETT exchange rates and lower extubation failure rates, fewer subjects who needed a new tracheostomy, shorter duration of mechanical ventilation, shorter pediatric ICU and hospital stay, and lower mortality, but none of these changes were statistically significant. Pediatric ICU-level subject outcomes are shown in Table 4.
Tracheal Intubation Adverse Events
Pediatric ICU-Level Subject Outcomes
Discussion
Our study demonstrated improvement in some elements of pediatric advanced airway management in a set of general emergency departments by following a collaborative intervention program. These improvements were mainly in adherence to the recommended ETT type and in decreasing severe tracheal intubation associated adverse events. We attribute the improvement to the multifaceted approach of the intervention that included in situ simulation and post-simulation debriefing coupled with providing general emergency departments with feedback and pediatric specific resources from the academic medical center. Simulation has been shown to be an effective method of training to enhance pediatric knowledge and skills in the acute care setting; it has been associated with improvements in the cognitive, technical, and behavioral skills of health-care providers.18,19 A series of recent studies successfully demonstrated the effect of in situ simulation on the skills and confidence of health-care providers in general emergency departments in treating various simulated pediatric critical conditions, such as diabetic ketoacidosis, airway management, and supraventricular tachycardia.11-15
In this study, simulation was used as a tool to assess and improve the process of care provided by interprofessional teams and identifies gaps and opportunities for improvements in the system of care in the general emergency department setting. Subsequently, simulation was used as an improvement tool with which these gaps were addressed with general emergency department leadership through the development of customized performance reports. An example was the common use of uncuffed ETT in the general emergency department during the simulations, which highlighted the need for pediatric-specific guidelines and best practices to be readily available and disseminated among general emergency department providers. For example, the distribution of ETT tag cards through each general emergency department pediatric champion, potentially resulted in the improvement noted in the use of cuffed ETT in the clinical setting after the intervention.20 This is an important finding and a clinically relevant component of this intervention because cuffed ETT is now recommended by the American Heart Association instead of uncuffed ETT as cuffed ETT decreases the chance of ETT exchange and facilitates ventilation, especially in children with poor lung compliance.21
Our study findings were consistent with previous results of the study by Andreatta et al,22 which demonstrated improvement of cardiac arrest outcomes after integration of a formal code program into the residency curriculum. When comparing the current study with our previous study in a simulated setting, the cuffed ETT use in follow-up simulation was 71%, which translated to a similar percentage in actual patient care in the current study; however, the ETT size and depth did not have similar improvement.12 One potential explanation for the lack of improvement in the recommended ETT depth is that the general emergency department team and transport team might be less willing to adjust the ETT before transfer to an academic medical center unless the patient has ventilation issues.
The decrease in severe tracheal intubation associated adverse events was another example of translating the simulation experience to actual patient care. During the in situ simulation, the focus was to train the team to (1) collect all needed equipment for airway management, including the appropriate ETT, laryngoscope, suction catheter, bag, and mask; (2) perform a timeout, correct bag mask ventilation and intubation; and (3) correctly verify ETT placement.12 In situ simulation provided higher realism when compared with the simulation conducted in simulation center or classroom because it allows general emergency department providers to deliver care in their actual clinical environment, which involves real-world interprofessional provider teams, equipment, and resources. This has potentially helped the team to have a shared mental model through the intubation process, which, subsequently, resulted in a more efficient process and ultimately decreased the incidence of tracheal intubation associated adverse events.
This use of simulation for team training in emergency departments has been extensively established and successful in improving team performance and communication in the acute care setting.23-25 For non-severe tracheal intubation adverse events, the most commonly reported events were right main bronchial intubation and pain and/or agitation. Our study’s severe tracheal intubation associated adverse event pre-intervention rate is comparable with a recent report by Neubrand et al.10 Although non-severe events were higher than what was reported by Nishisaki et al,6 this could be attributed to the inadequate documentation of the events by general emergency departments in their study.
We also hypothesize that better airway management in general emergency departments will translate to improvement in patients’ clinical outcomes, such as extubation failure, duration of mechanical ventilation, pediatric ICU, and hospital stay. These outcomes did not significantly change in the post-intervention period compared with the pre-intervention period. It should be noted that these outcomes were affected by multiple confounders that were difficult to control for in a retrospective study with small sample size.
This study had a few limitations in addition to the relatively small sample size. This was a retrospective study that used a chart review, with a potential lack of or inaccurate documentation by the general emergency department teams. Another limitation of this study included incomplete or missing data within the medical record and the variability of documentation among the providers in general emergency departments. We did not include patients who died in a general emergency department before transfer to an academic medical center pediatric ICU, which might affect the tracheal intubation associated adverse event rates in both periods of the study. During the review process, it was noted that some physicians documented that, during intubation, certain tools or the appropriate size equipment was not available in their hospital, which could have negatively impacted the effectiveness of our intervention and confounded the findings of this study. Last, given the retrospective nature of our study, we could not conclude which of the collaborative program components had the most significant impact on the improvement. Future prospective controlled studies are needed to address this issue further.
Conclusions
Our study showed that a multifaceted intervention program between the academic medical center and general emergency departments can lead to improvement in best practices in pediatric advanced airway management. This model of collaboration that involves simulation, sharing resources, and ongoing communication can be used to improve the quality of care of children who present to general emergency departments and potential downstream patient outcomes.
Acknowledgments
We thank the team members and pediatric emergency care coordinators of the general emergency departments for participating in and facilitating the study. We also appreciate the feedback provided by members of the International Network for Simulation-based Pediatric Innovation, Research and Education to shape this project.
Footnotes
- Correspondence: Samer Abu-Sultaneh MD, Division of Pediatric Critical Care, Department of Pediatrics, Riley Hospital for Children at Indiana University Health, Indianapolis, Indiana. E-mail: sultaneh{at}iu.edu
The project was funded by an Indiana University Health Values grant (VFE-332 [Dr Lutfi], VFE-342 [Dr Abu-Sultaneh]).
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2021 by Daedalus Enterprises





{kind=link}
{kind=link}