

To the Editor:
Almost 50 years after its birth in respiratory physiology,1,2 we are seeing a growing interest in the airway-occlusion pressure at 0.1 s (P0.1) parameter as an expression of the mechanical output of the respiratory drive and, therefore, of the inspiratory effort made by the patient. The assessment of P0.1 in patients with acute hypoxemic respiratory failure may help in decision making regarding mechanical ventilation and sedation, with the aim to protect the patient from self-induced lung and diaphragm injury.3,4 The measurement of P0.1 is offered by a few mechanical ventilators according to different technologies: either a short patient-triggered occlusion performed on demand by closure of the ventilator valves or a continuous breath-by-breath analysis of airway pressure during the short interval preceding inspiratory trigger activation.
In turn, continuous P0.1 monitoring is based on two different methods. The mini-occlusion method was designed in the 1990s and is based on the measurement and extrapolation to 100 ms of the maximum slope of the airway-pressure drop during the short—but full—occlusion associated with pressure-triggering.5,6 It was shown to provide accurate P0.1 assessments even on trigger intervals < 100 ms.6 The non-occlusive method was developed later for the pneumatics of modern ventilators with flow-triggering associated with a substantial, adaptive flow-by during expiration and no occlusion during the trigger interval.
Continuous P0.1 monitoring provides obvious advantages over performing punctual measurements, especially if we consider the breath-by-breath variability of spontaneous breathing and thus of P0.1. However, 3 studies found relevant accuracy limitations for continuous P0.1 monitoring, contrarily to P0.1 measurements from occlusions on demand. The non-occlusive continuous method resulted in significant underestimation of P0.1 both on the bench4 and in a clinical study.7 These results have been recently confirmed by the bench study of Katayama et al,8 who found a relevant underestimation for the non-occlusive method and also an overestimation for the mini-occlusion method, both proportional to the magnitude of the P0.1 value.
Wondering whether the attractive concept of continuous P0.1 monitoring be destined to fatally die as affected by insufficient accuracy, we performed additional bench tests. We analyzed two different ventilators: a Hamilton-G5 for the mini-occlusion method and a Hamilton-C6 for the non-occlusive method (Hamilton Medical, Bonaduz, Switzerland). Of note, the P0.1 measurement algorithm of Hamilton-C6 has been recently modified (software v1.2.3). Using an ASL 5000 simulator (IngMar Medical, Pittsburgh, Pennsylvania) and the ventilator settings as published by Katayama et al,8 we reproduced the same 42 scenarios (normal model and obstructive model, with sinusoidal wave pattern of muscular pressure).
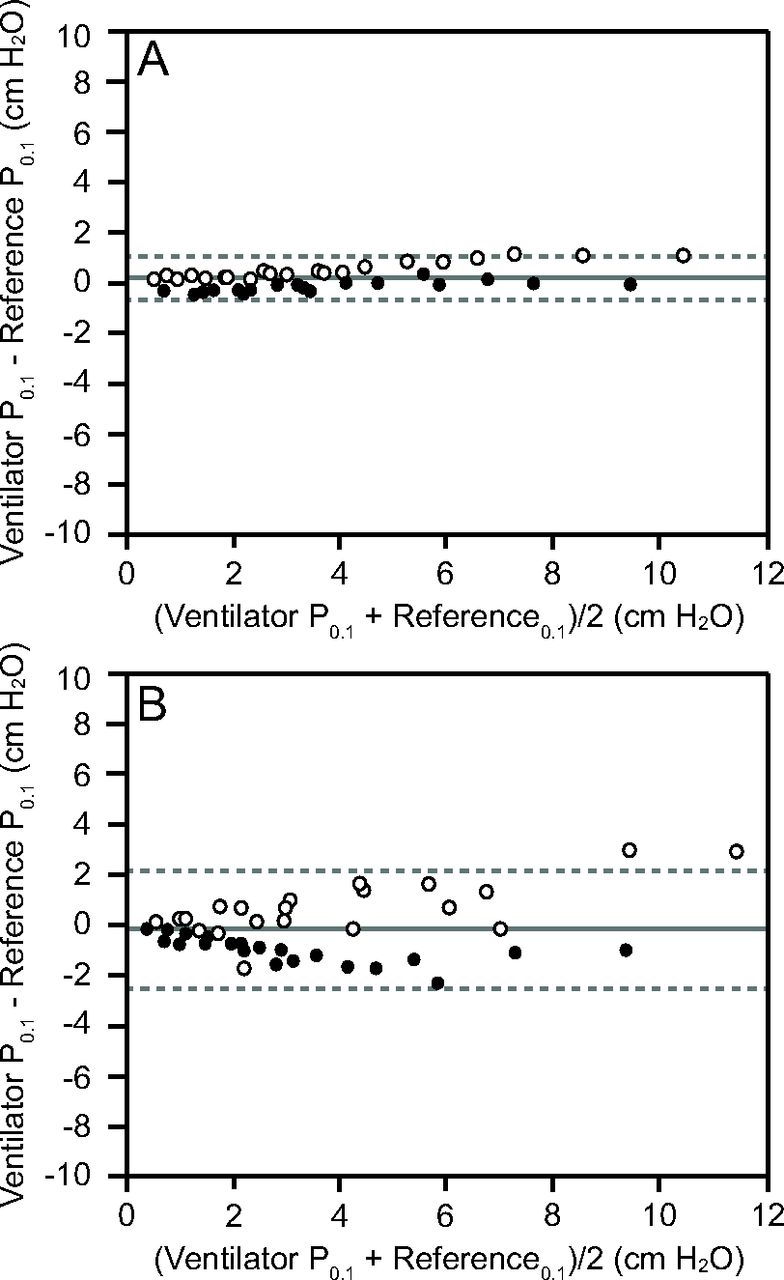
In the comparison with reference P0.1 measurements obtained by formal end-expiratory occlusion maneuvers, the bias of continuous P0.1 was 0.20 cm H2O with 95% limits of agreement (as an expression of precision) of ± 0.86 cm H2O as performed by Hamilton-G5 with the mini-occlusion method (Fig. 1 panel A) and −0.04 cm H2O with 95% limits of agreement of ± 2.35 cm H2O as performed by Hamilton-C6 with the non-occlusive method (Fig. 1 panel B). Among the different simulation scenarios, the plots show no relevant dependence of the bias on the magnitude of P0.1. The mini-occlusion method maintains a good precision within the entire explored range, while the non-occlusive method shows a moderate decrease in precision with increasing P0.1 values. This is primarily caused by a tendency toward an overestimation with the normal simulation model and a slight underestimation with the obstructive model.

Bland-Altman plots comparing ventilator continuous airway-occlusion pressure at 0.1 s (P0.1) and reference P0.1 by end-expiratory occlusion for the Hamilton-G5 with software v2.91 (panel A) and Hamilton-C6 with software v1.2.3 (panel B). The solid line represents bias, and the dashed lines represent 95% limits of agreement. The white dots refer to the normal simulation model, the black dots to the obstructive model.
Continuous P0.1 measurement by mini-occlusion was designed when pressure-trigger was the only inspiratory synchronization technology available. Our results show that the subsequent evolution of ventilator pneumatics did not impede to maintain the good accuracy that was originally reported.6 However, the applicability of the mini-occlusion method is restricted to pressure-triggering, while flow-triggering is probably the most common choice in current clinical practice. Continuous measurement of P0.1 in the pneumatic condition of flow-triggering is obviously quite challenging, the ultimate goal being to obtain an occlusion pressure measurement while the ventilator circuit is open. Our results show that, although a true occlusion is lacking, the trigger interval can provide the information for a P0.1 calculation of sufficient accuracy to give the clinician an unequivocal understanding of the magnitude of inspiratory effort performed by the patient.
In conclusion, the accuracy of continuous P0.1 measurement is good with the mini-occlusion method and sufficient for clinical use with the non-occlusive method. Whereas the paradox of measuring an occlusion pressure without occlusion maneuver has been technically overcome, a semantic issue probably remains open. For sake of clarity, perhaps a different name should be used for this non-occlusive equivalent of P0.1.
Footnotes
- Correspondence: Giorgio A Iotti MD. E-mail: giorgio.a.iotti{at}gmail.com
Drs Iotti, Negri and Schranz disclose relationships with Hamilton Medical.
- Copyright © 2024 by Daedalus Enterprises





{kind=link}