

Abstract
BACKGROUND: In this study, we examined the association between 25-hydroxyvitamin D (25(OH)D) concentration and successful weaning from mechanical ventilation in a cohort of ICU survivors requiring prolonged mechanical ventilation.
METHODS: This was a retrospective cohort study of ICU survivors admitted to a long-term acute care hospital. Demographic data were extracted from medical records, including 25(OH)D concentrations drawn on admission. Subjects were divided into 2 groups based on their 25(OH)D concentrations (deficient, < 20 ng/mL; not deficient, ≥ 20 ng/mL), and associations between 25(OH)D concentration and successful weaning were calculated.
RESULTS: A total of 183 subjects were studied. A high prevalence of 25(OH)D deficiency was found (61%, 111/183). No association was found between 25(OH)D concentration and weaning from mechanical ventilation. Increased comorbidity burden (Charlson comorbidity index) was associated with decreased odds of weaning (odds ratio of 0.50, 95% CI 0.25–0.99, P = .05).
CONCLUSIONS: Vitamin D deficiency is common in ICU survivors requiring prolonged mechanical ventilation. Surprisingly, there was no significant relationship between 25(OH)D concentration and successful weaning. This finding may be due to the low 25(OH)D concentrations seen in our subjects. Given what is known about vitamin D and lung function and given the low vitamin D concentrations seen in patients requiring long-term ventilatory support, interventional studies assessing the effects of 25(OH)D supplementation in these patients are needed.
Introduction
Survivors of catastrophic critical illness often require extended care outside of the ICU. These patients have been referred to as chronically critically ill or having protracted critical illness.1,2 Many of these patients require ventilatory support, as they cannot be weaned during their ICU stay. A long-term acute care (LTAC) hospital provides the specialized care required for prolonged mechanical ventilation, as well as treatment for severe malnutrition, physical deconditioning, and decubitus wounds present in these patients recovering from sequelae of critical illness.3,4 At LTAC hospitals, critical illness survivors receive multidisciplinary care. Typically, each nurse cares for 5 or 6 patients, a number that is well above the 2:1 patient-to-nurse ratio that is typically seen in ICUs. LTAC patients receive treatment designed to promote ventilator weaning and to decrease morbidity and mortality.5–9 Although only 10% of all ICU patients are discharged to an LTAC hospital, they utilize ∼40% of all critical care resources for an annual cost of ∼20 billion dollars.10
Although its primary role is to help regulate the mineralization and calcification of bone, vitamin D is a steroid hormone with multiple physiologic effects. Vitamin D receptors are present in almost all tissues in the human body,11 and vitamin D plays an important role in angiogenesis, apoptosis, cell differentiation and proliferation, and immunomodulation. The presence of vitamin D receptors on CD4, CD8, B cells, neutrophils, and a host of other immune cells suggests that it plays an integral part of the body's immune response.12
Vitamin D concentration has been associated with lung development, function, and other pulmonary-associated measures. In mouse models, incomplete lung development with resulting decreased volume has been shown to be directly associated with vitamin D deficiency.13 Vitamin D concentration has been shown to be directly correlated with spirometry and gas exchange in subjects with interstitial lung disease.14 Subjects with COPD who had mild vitamin D insufficiency15 and who engaged in rehabilitation demonstrated higher functional gains when vitamin D supplementation was added to their rehabilitation regimen.16 Furthermore, COPD subjects with severe vitamin D deficiency (< 10 ng/mL) had a significantly lower rate of COPD exacerbations with supplementation compared with those without.17
Our retrospective cohort study of ICU subjects in an LTAC hospital tested the hypothesis that 25-hydroxyvitamin D (25(OH)D) concentration is inversely associated with the odds of successful weaning from prolonged mechanical ventilation. To accomplish this, we studied 183 subjects previously admitted to an LTAC facility and followed their progress for 60 d or until discharge home, transfer out of the facility, or death.
QUICK LOOK
Current knowledge
Vitamin D concentrations have been associated with lung development, function, and other pulmonary-associated measures. Vitamin D concentrations have been shown to be directly correlated with spirometry and gas exchange in patients with interstitial lung disease. Patients with COPD and mild vitamin D insufficiency have shown a significantly lower rate of exacerbations when given supplementation.
What this paper contributes to our knowledge
Vitamin D deficiency was a common finding in ICU survivors requiring prolonged mechanical ventilation. There was no significant relationship between 25-hydroxyvitamin D concentrations and successful weaning. A number of subjects had very low vitamin D levels, and the role of vitamin D supplementation remains unknown.
Methods
Study Design and Subject Selection
We conducted a retrospective cohort study of 183 subjects 18 y of age or older who were discharged from June 1, 2010 to May 31, 2012 from the ICU directly to the University Specialty Hospital, an urban LTAC facility affiliated with the University of Maryland Medical Center. To be eligible for our study, the subjects could not have received prolonged ventilatory support before their ICU admission, but subsequent to being admitted to the ICU and before being admitted to the LTAC facility, they must have required mechanical ventilation for ≥ 21 d. All subjects had a tracheotomy and were medically stable, having recovered from the disease or condition that precipitated their initial hospitalization. To be eligible for admission to the LTAC facility, the patients had to be able to tolerate at least 1 h of therapy (physical therapy, occupational therapy, or speech/language pathology) per d. Therapy consisted of basic mobility training and retraining in the activities of daily living, speech, and swallowing. None of the subjects in our study received vitamin D supplementation, as the study was conducted before the importance of measuring vitamin D concentration and supplementing patients with low concentrations became general medical practice. The subjects were followed from the time of their admission to the LTAC hospital for 60 d or until they were discharged home, were transferred out of the facility, or died. Subjects who were discharged from the LTAC hospital to an acute care facility or another location contributed data to our analysis up until the time that they were discharged. If they were subsequently readmitted to the LTAC facility, their additional follow-up experience was not included in our analysis. This study was approved by the University of Maryland School of Medicine institutional review board.
Data Collection
Data extracted from a subject's electronic medical record included demographic information, presence of indwelling lines (central venous catheters, Foley catheters), feeding tubes, prior site and unit of hospitalization (medical, surgical, trauma, neurologic, or cardiac ICU), presence of decubitus ulcers, LTAC stay, nursing and respiratory notes, radiography reports, and laboratory results (microbiology culture, creatinine, prealbumin, albumin, hemoglobin, complete blood count, vitamin D concentration). Subjects were placed into one of 2 groups based upon their 25(OH)D concentration: deficient (< 20 ng/mL) or not deficient (≥ 20 ng/mL) following the Endocrinology Society guidelines for interpreting 25(OH)D concentrations.11 Comorbidity burden was determined using the Charlson comorbidity index with the Deyo modification.18 The Charlson comorbidity index is a weighted scoring system that estimates 1-y mortality based on comorbid conditions as defined by Internal Classification of Diseases, 9th Revision codes. Higher Charlson comorbidity index values represent greater comorbidity and higher probability of 1-y mortality.
Outcome Measures
Our outcome measure was weaning status 60 d after entry into the study or at time of death or discharge from the LTAC hospital if death or discharge occurred before day 60. Successful weaning was defined following National Association of Medical Direction of Respiratory Care guidelines, which include the ability to tolerate a tracheostomy collar for 48 h without mechanical ventilatory support or for 7 d requiring only nocturnal ventilation for ≤ 8 h.19 Weaning status was recorded as weaned or not weaned.
Statistical Analysis
Thirty-four candidate predictor variables were tested for an association with weaning. Variables are listed in Table 1. These variables are in addition to the 16 variables that compose the Charlson comorbidity index. Those variables that on bivariate analysis demonstrated a significant relation to weaning and 25(OH)D concentration and thus were potential predictors or confounders (P < .20) of the relationship between 25(OH)D concentration and weaning were included in a multivariable logistic regression predicting weaning. As a result of these analyses, 25(OH)D, age, race, serum albumin concentration, and presence of comorbid conditions (assessed by the Charlson comorbidity index) were included in our multivariable logistic regression predicting weaning. One additional variable, renal function (requiring vs not requiring dialysis), was included in the model, as renal function has been shown to be a predictor of weaning in other studies. Each covariate's range of values was divided into 2 groups based on values published in medical literature. We chose ≥ 65 y old as defining older versus younger, as 65 y is well established as designating older individuals. The Charlson comorbidity index was divided into ≤ 5 versus > 5, as subjects with a Charlson comorbidity index of ≤ 5 were demonstrated by Charlson to have a mortality of 85%.18 A serum albumin concentration of ≥ 2.4 g/dL was used as a discriminator value to designate an adequate versus inadequate level. Race was characterized as black versus non-black. The Pearson chi-square test was used to compare categorical variables, and analysis of variance was used to compare means between the 2 strata of 25(OH)D. Continuous variables are presented as mean ± SD, and categorical variables are presented as counts and percentages unless indicated otherwise. We used the traditional definition of a 2-tailed P ≤ .05 for statistical significance.
Baseline Characteristics of Mechanically Ventilated ICU Survivor Cohort by 25(OH)D status
Results
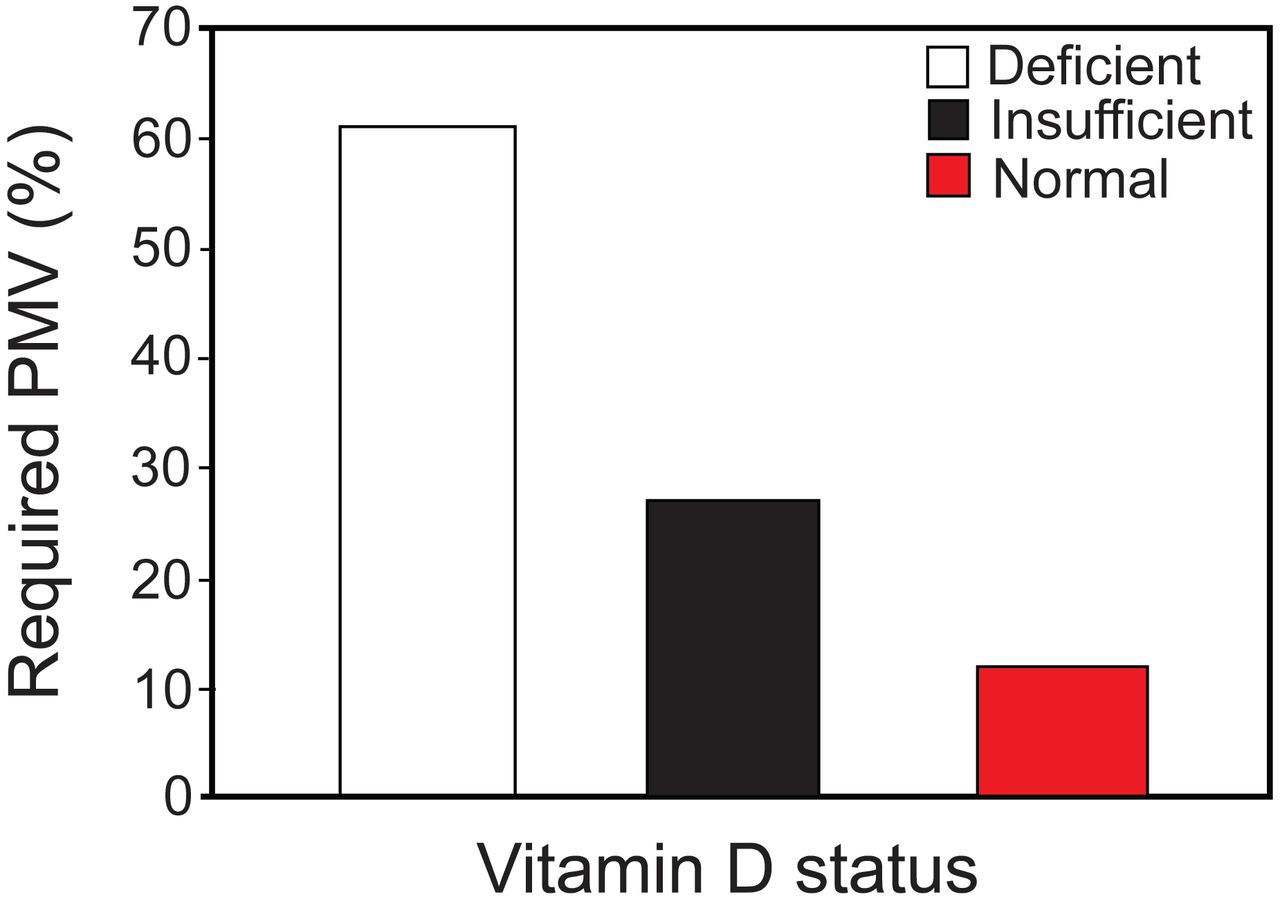
A total of 183 subjects were divided into 2 groups based on 25(OH)D concentration: < 20 ng/mL and ≥ 20 ng/mL (see Table 1). The median 25(OH)D concentration of the cohort was 16.3 ng/mL, with an interquartile range of 10.1–24.2 ng/mL (range of 4.0–71.7 ng/mL). The mean age of the subjects was 58 ± 15 y (range of 18–87 y), and 47% were black. Half of the subjects had decubitus ulcers (51%), and 89% received feeding via a percutaneous gastrostomy tube. Comorbidity burden was high, and the mean Charlson comorbidity index was 5.0 ± 3.0. Average stay in the ventilator weaning unit was 57 ± 62 d (range of 4–168 d). During follow-up, 66 of 183 subjects were weaned: 41% (45/111) of the deficient 25(OH)D group (< 20 ng/mL) and 29% (21/72) of those with insufficient or normal concentrations (≥ 20 ng/mL) successfully weaned. By the end of follow-up, the status of our 183 subjects was as follows: 32/183 (17%) went home, 96/183 (53%) were transferred to an acute care facility, 47/183 (26%) were discharged to a skilled nursing facility, and 8/183 (4%) died. The vitamin D concentrations in our subjects were quite low, as the majority of the subjects' concentrations were in the deficient range (Fig. 1): 61% (111/183) of our subjects were deficient, 27% (49/183) were insufficient, and 12% (22/183) had levels in the normal range. Subjects with deficient 25(OH)D concentrations (< 20 ng/dL) were more likely to be black (55% vs 36%, P = .01), had a significantly shorter hospital stay (46 ± 34 vs 71 ± 92 d, P < .001) and a lower 25(OH)D concentration (11 ± 4 vs 29 ± 10 ng/dL, P < .001), were more likely to be hemodialysis-dependent (17% vs 5%, P = .02), and had lower hemoglobin (9.2 ± 1.7 vs 9.7 ± 1.7 g/dL, P < .04). All subjects admitted to the LTAC hospital had to be hemodynamically stable, and thus, transfusion upon admission to the LTAC hospital was extremely rare. On those few occasions when a subject received a transfusion, the blood product transfused was frequently packed red blood cells that contained little (if any) vitamin D. Furthermore, none of the subjects received vitamin D supplementation, as our study was conducted before the importance of testing for and supplementing with low 25(OH)D concentrations was common medical practice. Thus, the 25(OH)D levels we report are accurate estimates of the subjects' 25(OH)D concentrations.

Vitamin D status of ICU survivors requiring prolonged mechanical ventilation (PMV). Deficient, < 20 ng/mL 25-hydroxyvitamin D (25(OH)D); insufficient, 20–29.9 ng/mL 25(OH)D; normal, ≥ 30 ng/mL 25(OH)D.
Unadjusted logistic regression comparing subjects who successfully weaned with those who did not failed to demonstrate an association between 25(OH)D concentration and successful weaning. In multivariable logistic regression (Table 2), no association was found between successful weaning and 25(OH)D concentration (deficient vs not deficient, odds ratio [OR] = 0.62, 95% CI 0.32–1.22, P = .17). When analysis was performed assessing the relationship between the vitamin D classifications deficient (< 20 ng/mL), insufficient (20–29.9 ng/mL), and normal (≥ 30 ng/mL), the results were similar (< 20 ng/mL, OR = 1.0 [reference]; 20–29.9 ng/mL, OR = 2.38, 95% CI 0.37–15.23; ≥ 30 ng/mL, OR = 1.82, 95% CI 0.27–12.35). In the model, the OR for a Charlson comorbidity index of ≥ 5 compared with < 5 was 0.50 (95% CI 0.25–0.99, P = .05) (Table 2), indicating a lower likelihood of successful weaning for those with a higher Charlson comorbidity index. When 25(OH)D concentration was entered into the model as a continuous covariate or when the Charlson comorbidity index was added to the model as a continuous covariate, the inferences drawn were essentially unchanged (25(OH)D as continuous variable, OR = 1.00, 95% CI 0.97–1.03; Charlson comorbidity index as continuous variable, OR = 0.91, 95% CI 0.81–1.01).
Multivariable Logistic Regression Examining Factors Associated With Weaning From Prolonged Mechanical Ventilation
Discussion
This study demonstrates the high prevalence of 25(OH)D insufficiency and deficiency in ICU survivors receiving prolonged mechanical ventilation and that higher comorbidity burden (higher Charlson comorbidity index) decreases the odds of successful weaning. Surprisingly, given what is known about vitamin D and its immunologic, anti-inflammatory, and antibacterial idiosyncratic effects, we were unable to find any relationship between 25(OH)D concentration and ventilator weaning success.
We are unaware of any prior studies that examined the relationship between 25(OH)D concentration and weaning from mechanical ventilation. However, a growing body of literature demonstrates relationships between 25(OH)D concentrations and lung development13 and function,20,21 particularly in obstructive lung disorders such as asthma and COPD. 25(OH)D concentration has a direct relationship with severity of obstructive lung disease in patients with COPD; lower 25(OH)D levels are associated with worse FEV1 and FVC.22 In addition, increased frequency and severity of exacerbations in patients with both COPD17 and asthma23 are associated with lower 25(OH)D concentrations. In the critically ill, 25(OH)D deficiency has been associated with longer hospital stays,24–27 higher incidence of renal failure,28 and increased mortality.29,30
Lung function plays a role in successful weaning from prolonged mechanical ventilation.31,32 Thus, it is reasonable to expect that higher 25(OH)D concentrations would be associated with increased odds of weaning. We were not able to demonstrate this, as we found no association between successful weaning and 25(OH)D concentration. There are several possible explanations for this surprising finding. It is possible that 25(OH)D concentration is unrelated to weaning, but as noted above, this would not be expected given what is now known about the actions of vitamin D. A second explanation is type-2 error, that is, not having enough power to demonstrate vitamin D's effect on weaning. Although possible, our sample size (66 of 183 subjects were successfully weaned) should be sufficient to demonstrate a reasonably robust effect of vitamin D on weaning. It is also possible that the vitamin D concentrations seen in our population were too low to allow 25(OH)D to have an effect on weaning. Our study population did not receive vitamin D supplementation, as our subjects were hospitalized before the relatively recent recognition of the importance of looking for and treating low 25(OH)D concentrations. Sixty-one percent of our subjects were vitamin D-deficient (25(OH)D < 20 ng/mL). This is greater than the 41% prevalence demonstrated in large population-based studies.33 We believe that our study is the first to document the extremely high prevalence of deficient 25(OH)D concentrations in the long-term care, chronically mechanically ventilated population. We recently demonstrated that, at least for glucose and insulin metabolism, 25(OH)D needs to be above ∼26 ng/mL to have an effect on outcome.34 The same may be true for weaning.
Our analyses demonstrate that subjects with higher comorbidity burden, as represented by a Charlson comorbidity index of ≥ 5, had a lower likelihood of weaning. Despite the biological plausibility of this finding, few studies have shown a relationship between the Charlson comorbidity index, representing the number and type of comorbidities, and weaning.35
Limitations of our study include the fact that our study was not a randomized controlled trial and that the 25(OH)D concentrations in our subjects were quite low. We do not know what would have happened if our subjects had received vitamin D supplementation. Additionally, although we chose the cut points for our independent variables based on published literature and biological plausibility, the cut points we chose for age, race, serum albumin, and Charlson comorbidity index may affect the results. Despite these limitations, to the best of our knowledge, our study is the first to examine the relation of 25(OH)D concentration with the ability to wean from long-term ventilatory support.
Conclusions
In summary, we were not able to demonstrate a significant relationship between baseline 25(OH)D concentrations on admission to the LTAC facility and successful weaning from mechanical ventilation. Nevertheless, we did show a relationship between the Charlson comorbidity index and weaning. Given what is known about the multiple physiologic effects of vitamin D (the relationship of 25(OH)D concentration to lung development and pulmonary function in patients with pulmonary diseases such as asthma and COPD, in particular), our results are counterintuitive. Our results may indicate that there is no support for a prospective interventional trial to determine whether 25(OH)D supplementation facilitates weaning. However, given the low 25(OH)D concentrations in our subjects, it may be that the values were below a critical value needed to facilitate weaning, and thus, a clinical trial of vitamin D in patients on long-term ventilatory support may be indicated.
Acknowledgments
We thank Dr Eileen Steinberger for helpful feedback in review of this manuscript throughout the stages of its preparation.
Footnotes
- Correspondence: Avelino C Verceles MD, Division of Pulmonary and Critical Medicine, University of Maryland School of Medicine, 110 South Paca Street, Second Floor, Baltimore, MD 21201. E-mail: avercele{at}medicine.umaryland.edu.
This work was supported by National Institute on Aging Grant R03 AG045100 (to Dr Verceles), University of Maryland Claude D Pepper Older Americans Independence Center Grant P30 AG028747 from the National Institute on Aging and the Baltimore Veterans Affairs Geriatric Research, Clinical, and Education Center (to Drs Verceles, Goldberg, and Sorkin), and National Institutes of Health Grant 5R21AG045573-02 (to Dr Netzer). The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}