

Abstract
Transfusion-related acute lung injury is a serious complication of blood transfusions. Herein is a report on a 32-year-old woman who developed diffuse pulmonary infiltrates and acute respiratory compromise after blood transfusion. Non-cardiogenic pulmonary edema was diagnosed based on data calculated by the hemodynamic monitoring system, but severe hypoxemia persisted despite conventional pressure-control ventilation with 100% oxygen, low tidal volume, and high PEEP. The refractory hypoxemia was improved by high-frequency oscillatory ventilation. This experience suggests that high-frequency oscillatory ventilation may be beneficial for patients with transfusion-related acute lung injury and severe refractory hypoxemia.
Introduction
Transfusion-related acute lung injury (TRALI) is a rare but life-threatening complication of blood transfusions. It usually occurs with the development of acute respiratory distress, non-cardiogenic pulmonary edema, and hypoxemia during or within 6 hours of transfusion.1 Treatment is mainly supportive, including oxygen support, noninvasive ventilation, or intubation with conventional mechanical ventilation.2
High-frequency oscillatory ventilation (HFOV) is an alternative mechanical ventilation used as rescue therapy for adult patients with acute lung injury (ALI) and acute respiratory distress syndrome (ARDS). Some observational studies have shown improved oxygenation in patients with refractory hypoxemia.3,4 A recent Cochrane review concluded that HFOV may be a rescue therapy for improving survival in ARDS patients.5
Herein is a case of TRALI with persistent hypoxemia under pressure-control ventilation mode with 100% oxygen, low tidal volume, and high PEEP. The refractory hypoxemia was effectively corrected by shifting to HFOV.
Case Report
A 32-year-old woman with insulin-dependent diabetes mellitus, hypertension, and chronic renal insufficiency was admitted to the gastroenterology ward due to hematemesis after intermittent nausea and vomiting for 5 days. Diagnostic esophagogastroscopy revealed gastroesophageal reflux and possible Mallory-Weiss tear. Before admission, no aspiration episode was described by the patient. After treatment with intravenous omeprazole 40 mg/d, the hematemesis stopped 2 days later. She was transferred to the nephrology ward for progressively elevated blood urea nitrogen and serum creatinine. Before admission, the baseline serum blood urea nitrogen, creatinine, and daily urine amount were 52 mg/dL, 4.1 mg/dL, and 1,000–1100 mL. Compared with baseline renal function, there was no sudden decline in renal function on admission. Her serum blood urea nitrogen and creatinine were 55 mg/dL and 4.2 mg/dL, respectively, on admission, but increased to 92 mg/dL and 5.0 mg/dL, respectively, after 3 weeks. Under the diuretics treatment with oral furosemide 80 mg/d, her daily urine amount was between 950 mL/d and 1,150 mL/d during admission. Suggested arteriovenous shunt creation for renal replacement therapy was declined.
Because of anemia (hemoglobin 7.5 g/dL), 2 units of packed red blood cells (packed RBC) were transfused, without adverse reaction. Chest radiograph taken the following day was unremarkable. Her hemoglobin was 7.8 g/dL 6 days after the first blood transfusion, so another 2 units of packed RBC were transfused to keep the hemoglobin above 8.0 g/dL. During these 6 days no other acute event or ongoing hemorrhage occurred. Thirty minutes after completing the transfusion, she experienced shortness of breath and her respiratory rate increased to 24 breaths/min. At the time of symptom onset, heart rate was 92 beats/min and blood pressure was 148/86 mm Hg. Bedside echocardiography revealed adequate left ventricle systolic function, with ejection fraction 66% by M mode and normal early wave/atrial wave (E/A) ratio (E > A) of mitral valve flow by Doppler. The serum troponin-I and creatine kinase-MB fraction level were within normal range (0.11 ng/mL and 1.7 ng/mL).
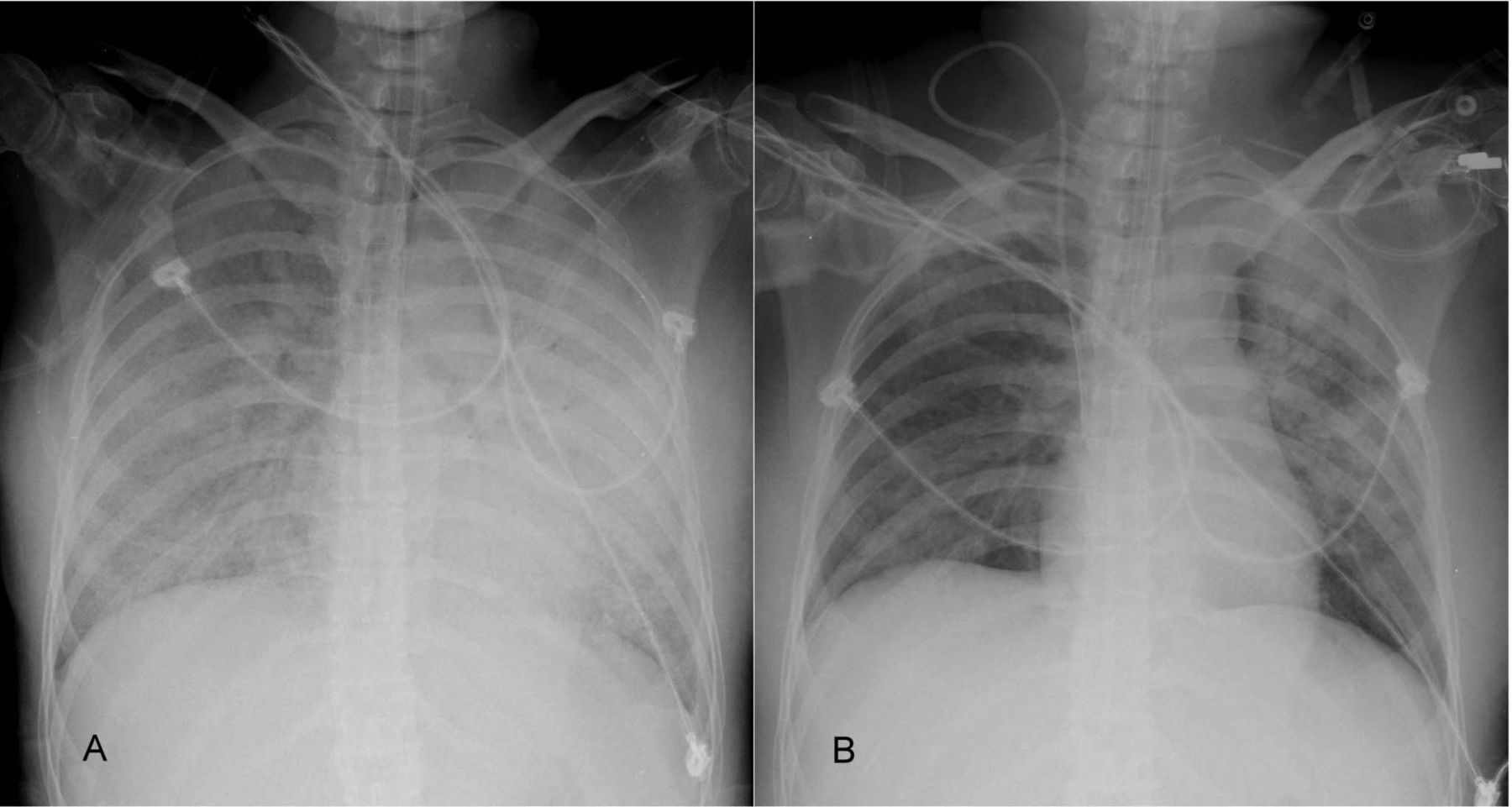
On physical examination there were fine inspiratory crackles in both lungs. Initial examination of arterial blood gases revealed pH 7.38, PaO2 66 mm Hg, and PaCO2 32 mm Hg on FIO2 of 0.5. In the 6 days between transfusions there was no mental change or aspiration episode. Because the respiratory distress did not respond to intravenous furosemide, she was intubated for mechanical ventilation. Post-transfusion hemogram showed hemoglobin 12 g/dL, with white cell count of 7,300/mL. The discordant high concentration level of hemoglobin was caused by volume contraction due to diuresis. Chest radiograph after intubation revealed diffuse bilateral pulmonary infiltrates, indicating acute pulmonary edema (Fig. 1A).
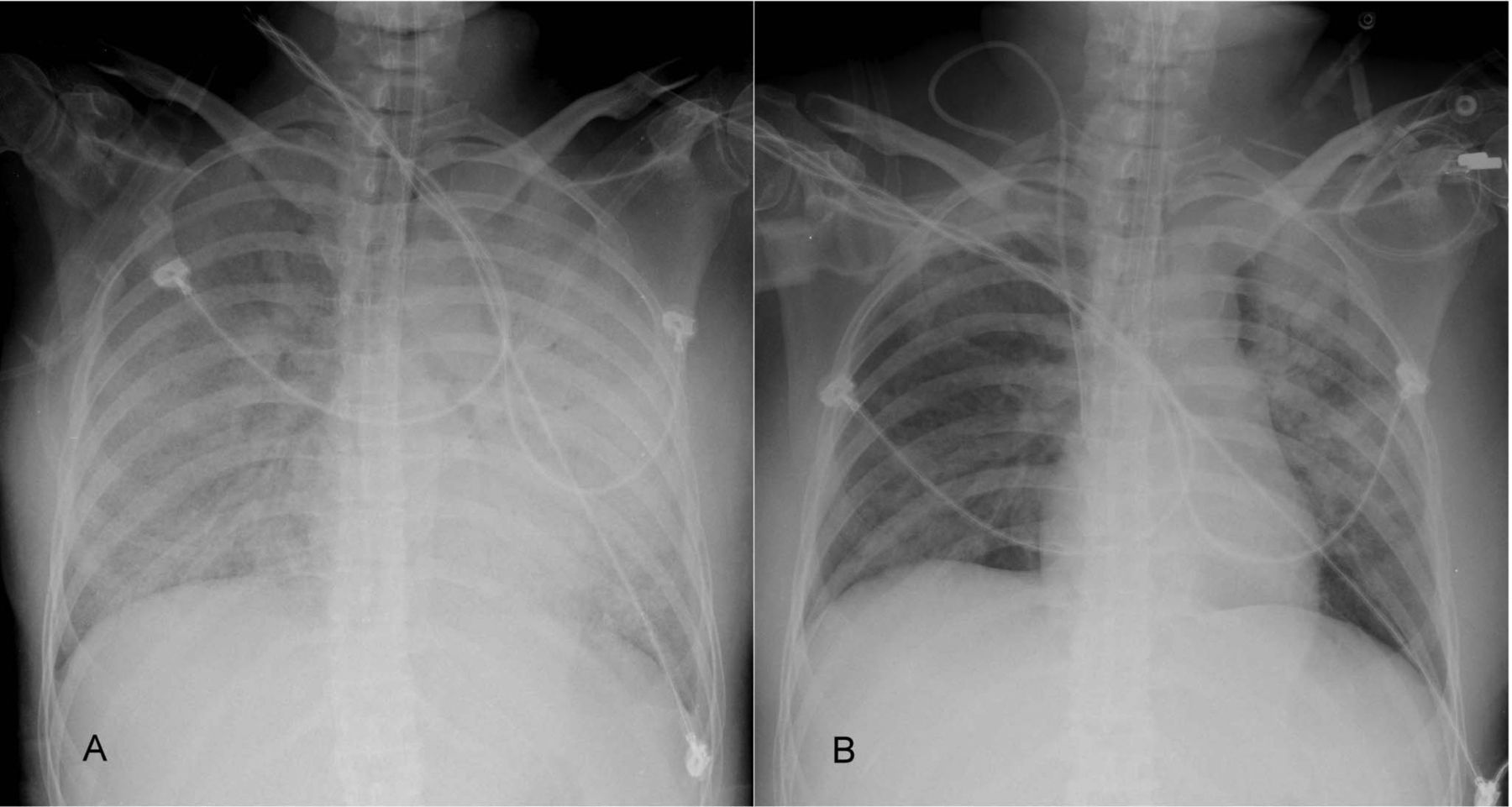
A: Diffuse bilateral pulmonary infiltration indicating acute pulmonary edema after intubation. B: Improvement of the diffuse bilateral pulmonary infiltrates after 2 days of high frequency oscillatory ventilation (HFOV).
Even under pressure control ventilation with 100% of oxygen, the patient had a low SpO2 of approximately 80%. Under the impression of pulmonary edema with fluid overload, emergency hemodialysis was initiated after discussion with her family. Emergency intermittent hemodialysis was performed one time to remove 2,100 mL volume, but there was no substantial improvement on her oxygenation, which was 82% at the end of hemodialysis. There was no evidence of infection developed, including fever, cough with purulent sputum, pyuria, dysuria, or intra-abdominal pain. In addition, there was no new drug administered in the days preceding the second transfusion. Hemodynamic monitoring (PiCCO, Pulsion Medical Systems, Munich, Germany) after hemodialysis showed low cardiac index of 2.77 L/min/m2, low global end-diastolic volume index of 606 mL/m2, low intrathoracic blood volume index of 757 mL/m2, high extra-vascular lung water index of 37 mL/kg, and high pulmonary vascular permeability index of 8.2. These data indicated non-cardiogenic pulmonary edema, and TRALI was diagnosed.
The initial mechanical ventilator setting consisted of a tidal volume of 6 mL/kg of predicted body weight, ventilation rate 25 breaths/min, PEEP 12 cm H2O, and 100% oxygen. The PEEP level was gradually increased by 2 cm H2O, due to SpO2 below 90%. After increasing PEEP level to 18 cm H2O, the maximum plateau pressure was 32 cm H2O. A recruitment maneuver was performed as a sustained inflation with mean airway pressure of 45 cm H2O for 45 seconds before HFOV, but in vain. Due to persistent hypoxemia, despite 12 hours of pressure control ventilation support with 100% oxygen and 18 cm H2O PEEP, the ventilator was changed to HFOV (3100B, SensorMedics, Yorba Linda, California). The initial ventilatory rate of HFOV was 3.5 Hz, with mean airway pressure set at 30 cm H2O. Oxygenation improved with HFOV, and the FIO2 decreased gradually to 45% with adequate arterial oxygen saturation. During HFOV the hemodialysis was not continued. The daily net intake/output volume state was positive 300 mL, and positive 250 mL during these 2 HFOV days. The PaO2/FIO2 and alveolar-arterial oxygen difference before and after HFOV are shown in Figure 2. Mechanical ventilation was changed to conventional pressure control ventilation after 2 days of HFOV, and chest radiograph showed improvement of the diffuse bilateral pulmonary infiltration (see Fig. 1B).
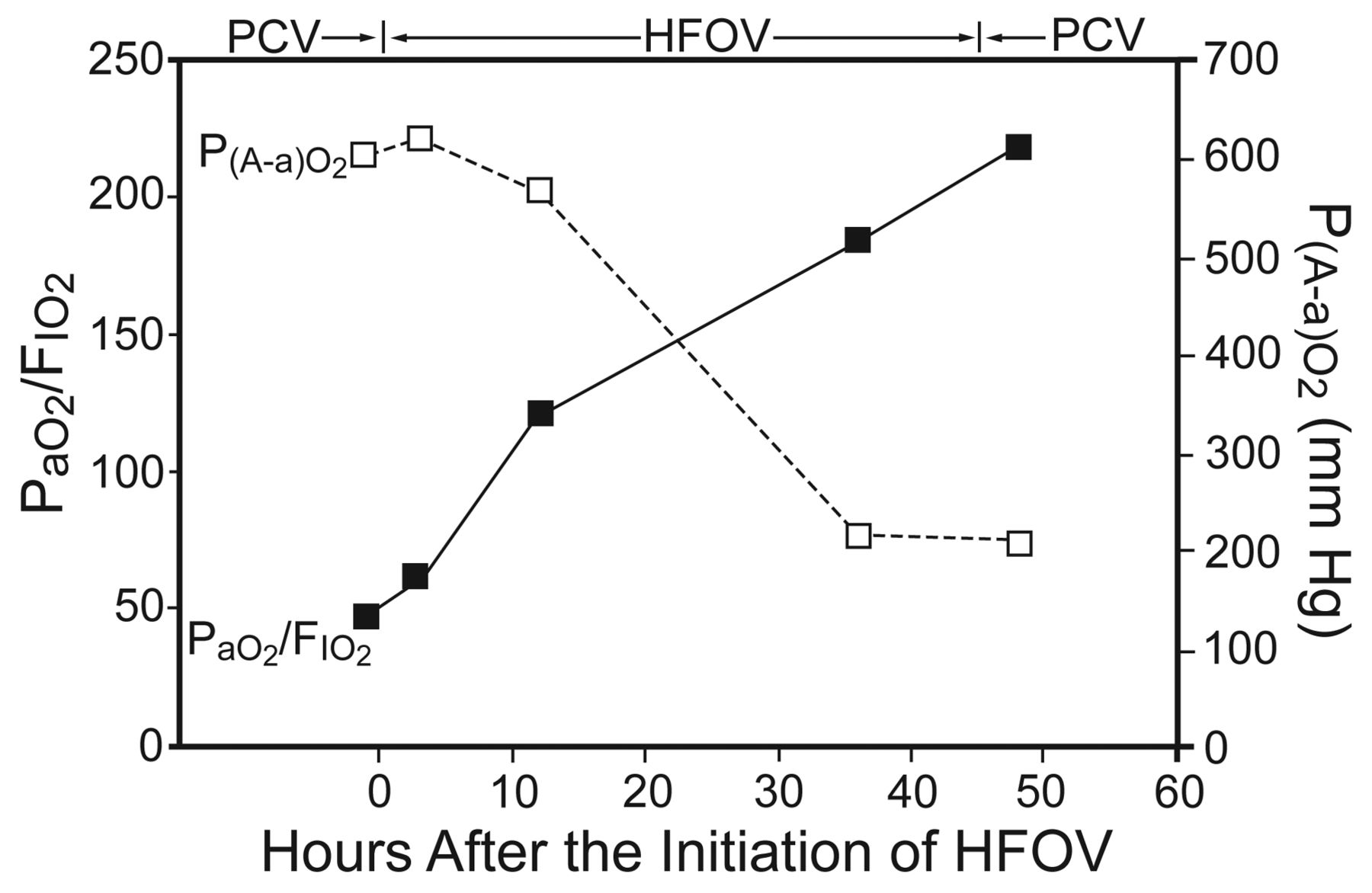
The PaO2/FIO2 and alveolar-arterial oxygen difference (P(A-a)O2) before and after high-frequency oscillatory ventilation (HFOV). PCV = pressure control ventilation.
The patient received 2 weeks of mechanical ventilation. Ten days after extubation she was transferred to the nephrology ward in stable respiratory condition.
Discussion
TRALI is a form of ALI defined as the presence of ALI within 6 hours of transfusion, in the absence of other risk factors for ALI.6 Critically ill patients with gastrointestinal bleeding are at a risk of developing TRALI, especially those with prior end-stage liver disease.7 The exact mechanism is unknown, although there is rising evidence that TRALI is immune-mediated. Its pathogenesis has been implied as 2 immunologic triggers: the infusion of antibodies directed against a cognate antigen in the recipient, and the infusion of biological response modifiers.8 In this case the first transfusion with packed RBC was tolerated without any complication. However, 6 days later, the ALI developed after the second transfusion with packed RBC. It may possibly be explained by the above 2-hit mechanism. In one of the largest series of TRALI cases reported, all of the patients required oxygen support, with 72% requiring mechanical ventilation.9 Nonetheless, 80% had substantial clinical improvement within 96 hours of onset of symptoms, while the remaining 20% either had a prolonged clinical course or succumbed to the disorder. The mortality rate is estimated to be between 5% and 15%. Once clinical symptoms resolve, no permanent sequelae have been associated.
This young diabetic woman developed acute respiratory failure with severe hypoxemia (PaO2/FIO2 132 mm Hg) and diffuse bilateral infiltrates on chest radiograph 30 min after second blood transfusion. The other risk factors for ALI or ARDS were excluded by clinical history and course. In TRALI, patients are more likely to exhibit hypotension, low pulmonary arterial occlusion pressure, and unresponsiveness to diuretics, which indicate non-cardiogenic pulmonary edema.10,11 The TRALI diagnosis hinges on exclusion of other entities, including transfusion-associated circulatory overload. There is no sentinel characteristic that distinguishes TRALI from transfusion-associated circulatory overload. However, the clinical symptoms and signs, fluid status, cardiac function (including measurement of brain natriuretic peptide), and leukocyte antibody testing are applied to differentiate these 2 disorders.8 In this case, although we did not undertake serum brain natriuretic peptide level and serological examination such as human leukocyte antigen class I or II antibodies or neutrophil specific antibodies, hemodynamic monitoring showed low cardiac index, low global end-diastolic volume index, low intrathoracic blood volume index, high extra-vascular lung water index, and high pulmonary vascular permeability index. These data indicated non-cardiogenic pulmonary edema, and TRALI was diagnosed.
For ALI and ARDS patients, lung-protective strategies with small tidal volume and adequate PEEP, as investigated in the ARDS Network trial, are associated with significantly more ventilator- and organ-failure-free days. There is also a 22% reduction in mortality, compared to higher tidal volumes.12 Management of TRALI is largely supportive, with more than 70% requiring mechanical ventilation.2,13 However, mechanical ventilation may be a risk factor for the onset of TRALI and may aggravate the injury by the use of injurious ventilator settings as shown in an animal study.14 For severe TRALI patients, strategies other than conventional mechanical ventilation, including prone position, nitric oxide inhalation, or extracorporeal membrane oxygenation, have been successfully applied to improve oxygenation.15–17 However, there is no report of HFOV in severe TRALI patients.
Theoretically, HFOV can achieve the goals of a lung-protective strategy.18 It can deliver very small tidal volumes at extremely rapid rates, thus avoiding large alveolar pressures and volume excursions typical of conventional ventilation. In addition, HFOV applied at a relatively high mean airway pressure can maintain lung requirements more effectively than PEEP levels that are typically set during conventional mechanical ventilation. Some studies of HFOV use for adult ARDS patients with severe hypoxemia and high plateau airway pressures have verified significant improvement in oxygenation and suggest that early initiation may have better outcomes.3,4,19 It has also been shown that HFOV is effective and safe in correcting oxygenation failure associated with ARDS in surgical patients.20
In this severe TRALI case, severe hypoxemia persisted despite pressure control ventilation support with 100% oxygen and PEEP of 18 cm H2O for 12 hours. After shifting the conventional mechanical ventilation to HFOV with higher mean airway pressure, the refractory hypoxemia was effectively corrected and the PaO2/FIO2 gradually improved from 50 to 200 mm Hg. After 50 hours the patient was successfully weaned from HFOV to conventional mechanical ventilation. Currently, HFOV for adult ARDS is considered a rescue therapy if conventional mechanical ventilation fails. However, the timing of HFOV initiation remains controversial. Furthermore, the optimal lung-protective HFOV strategy has not been investigated, and there is no validated standard algorithm proposed for patients receiving HFOV.
The majority of TRALI cases are self-limited and will resolve spontaneously with adequate support. Here we report a case of severe TRALI successfully supported by HFOV after conventional mechanical ventilation failed. We suggest that HFOV may be considered earlier as a rescue therapy for severe TRALI patients not responding to conventional mechanical ventilation.
Footnotes
- Correspondence: Kuo-Chin Kao MD, Department of Respiratory Care, Chang Gung University College of Medicine, 5 Fu-Shing Street, Kwei-Shan, Taoyuan, Taiwan, E-mail: kck0502{at}adm.cgmh.org.tw.
The authors have disclosed no conflicts of interest.
Dr Kao presented a version of this paper at the 56th International Respiratory Congress of the American Association for Respiratory Care, held December 6–9, 2010, in Las Vegas, Nevada.
- Copyright © 2012 by Daedalus Enterprises Inc.









{kind=link}
{kind=link}