

Abstract
BACKGROUND: In the United States, care for COPD patients is frequently delivered by respiratory therapists (RTs). After implementing a therapist-driven protocol for COPD treatment, we sought to improve identification of COPD patients. We hypothesized that using an electronic medical record screening tool to identify subjects with COPD combined with a therapist-driven protocol would positively impact length of stay (LOS) and readmission rates.
METHODS: Utilizing the electronic medical record to search the provider's admission notes for the terms COPD/Asthma, a report was generated. Subjects already receiving RT services were removed. An RT evaluated identified subjects using a therapist-driven protocol combining clinical assessment and FEV1 to calculate an air-flow obstruction score. Scores ≥7 received 24 h of bronchodilator therapy by RTs. Scores <7 received assessment by RTs but bronchodilator therapy administered by nursing staff. An RT performed medication reconciliation and education for both groups. ICD-9 discharge codes identified primary and secondary diagnoses of COPD. LOS and 30-d readmission rates were measured for a 14-month period. Respiratory-triggered rapid response data were also collected.
RESULTS: The pre-intervention period was from December 2013 to June 2014, and the post-intervention period was from July 2014 to January 2015. There were 142 subjects in total, 68 pre-intervention and 74 post-intervention. For primary COPD, mean LOS decreased from 4.37 to 2.96 d (P = .10), and 30-d readmission rates decreased from 13.6 to 6.1%. Respiratory-triggered rapid response data were as follows: The pre-intervention span was from January 2014 to June 2014, and post-intervention was from July 2014 to December 2015. For primary COPD, there were 61 pre-intervention subjects and 63 post-intervention with a decrease in respiratory-triggered rapid responses from 21 pre-intervention (34.4%) to 8 post-intervention (12.7%) (P = .004). For secondary COPD (1,168 pre-intervention, 1,267 post-intervention), there was a change from 318 (27.2%) pre-intervention to 296 (23.4%) post-intervention (P = .03).
CONCLUSION: Utilization of the electronic medical record to identify subjects with likely COPD combined with a therapist-driven protocol directed by RT assessment was associated with a trend toward decreased LOS and reduction in readmission rates. There was a significant reduction of respiratory-triggered rapid responses in subjects with a primary diagnosis of COPD.
Introduction
As of 2010, COPD had been identified as the third leading cause of death in the United States, and it is currently rising.1,2 As a longstanding concern for caregivers and health systems, COPD has contributed over the years to escalating health-care costs for everyone, health systems and patients alike.3 These costs come from a variety of sources, such as rapid response initiation and escalation of care, prolonged ICU and hospital lengths of stay, and, with the addition of COPD to the Centers for Medicare and Medicaid Services (CMS) readmissions penalties list, potential readmission penalties to health-care systems.3,4
With the passing of the United States Patient Protection and Affordable Care Act, a pay for performance initiative was launched by CMS that tied patient outcomes to reimbursement. In addition, it included a penalty program for hospitals that had readmission rates deemed to be excessive for specific disease processes. Current disease processes included in this bundle are acute myocardial infarction, congestive heart failure, pneumonia, and exacerbation of COPD.3,4 For hospitals that are out of compliance, this penalty program allows for a 1% decrease in payments for all patients covered by CMS in the first year with escalating percentage penalties in subsequent years. Currently, this program is at a 3% penalty phase for all cause, unplanned readmissions within 30 d in patients previously admitted for one of these conditions.
For the COPD population in the United States, the respiratory therapist (RT) often plays an important role in care, particularly in the in-patient hospital setting. Many therapies are delivered under the guidance of established clinical care guidelines and therapist-driven protocols, and have been shown to be very cost-effective and efficient for many health systems.5–7 In order to implement any protocol or treatment guideline, appropriate patient identification must happen. Pollack et al8 demonstrated nicely how leveraging the electronic medical record can improve this identification. By utilizing the electronic medical record to flag subjects appropriate for influenza vaccine screening, they were able to demonstrate an improvement in influenza vaccines given to hospitalized subjects.8
In a regional, level one trauma center and safety net facility, we sought to capitalize on the expertise of our existing respiratory therapy staff by implementing a therapist-driven protocol that utilized a scoring tool and an accompanying assessment and treatment protocol. The goal was to improve quality of care for patients with COPD and potentially show cost avoidance benefits.
A unique assessment scoring tool developed by the respiratory therapy department and embedded into our electronic medical record documentation was used to help determine levels of air-flow obstruction or general patient risk for air-flow obstruction during an in-patient stay. This scoring tool was built to encompass basic clinical assessment with the addition of an FEV1 (Fig. 1) that was accomplished using a basic, handheld spirometer (Lung Monitor, Vitalograph, North Buckinghamshire, United Kingdom). An assessment and treatment algorithm that utilized this score for the treatment pathway was created. Assignment to the different treatment pathway was dependent upon the initial score of the subject. The 2 treatment pathways were bronchodilator therapy and assessment by RT or assessment by RT and bronchodilator delivery by nursing; both groups received medication reconciliation and brief education by respiratory therapy staff as well (Fig. 2). Our facility's traditional approach to bronchodilator therapy was a model of physician-driven and nursing-delivered therapy.
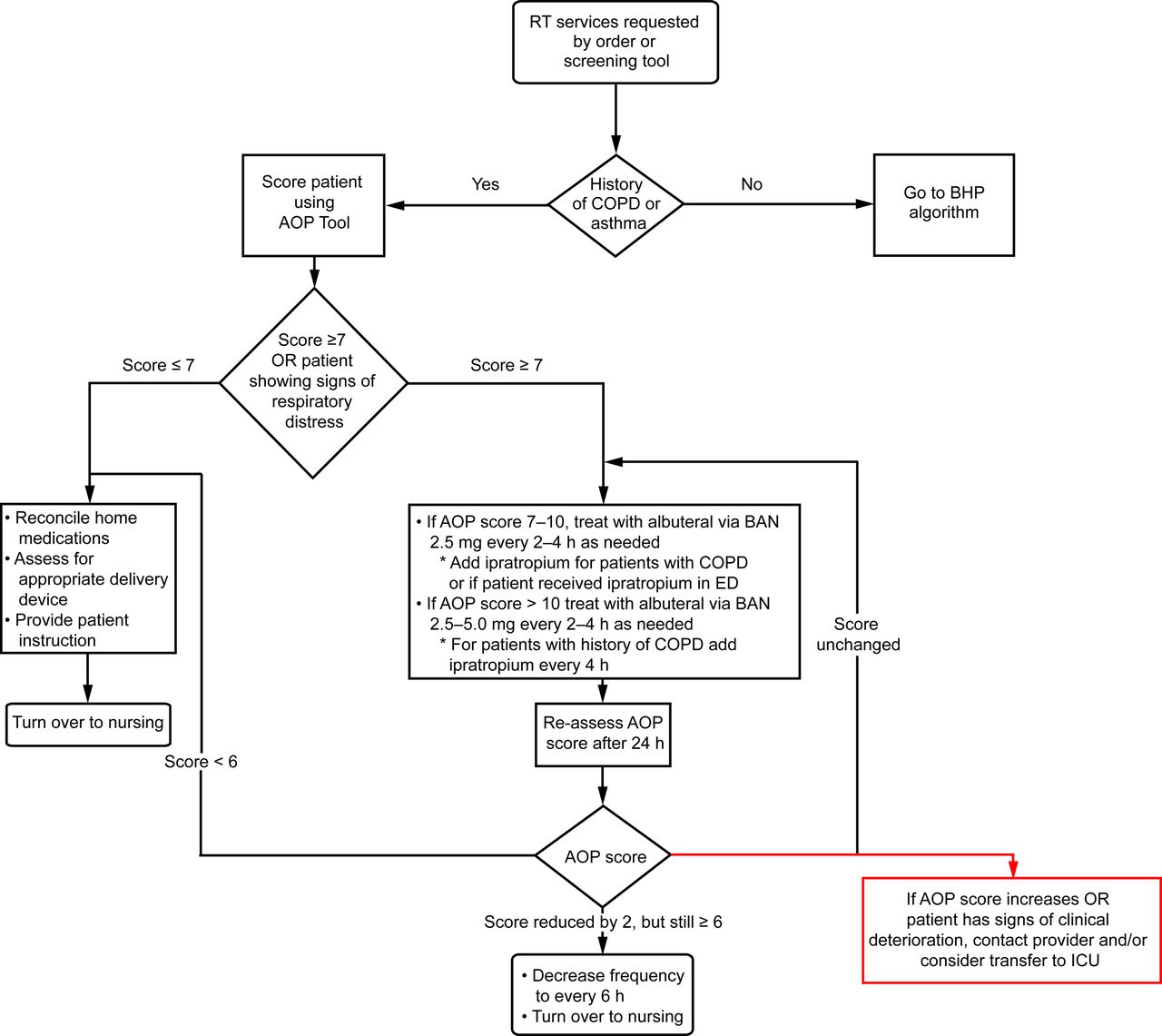
Airflow obstruction protocol (AOP) algorithm. RT = respiratory therapy, BHP = bronchopulmonary hygiene protocol, ED = emergency department, BAN = breath-actuated nebulizer.
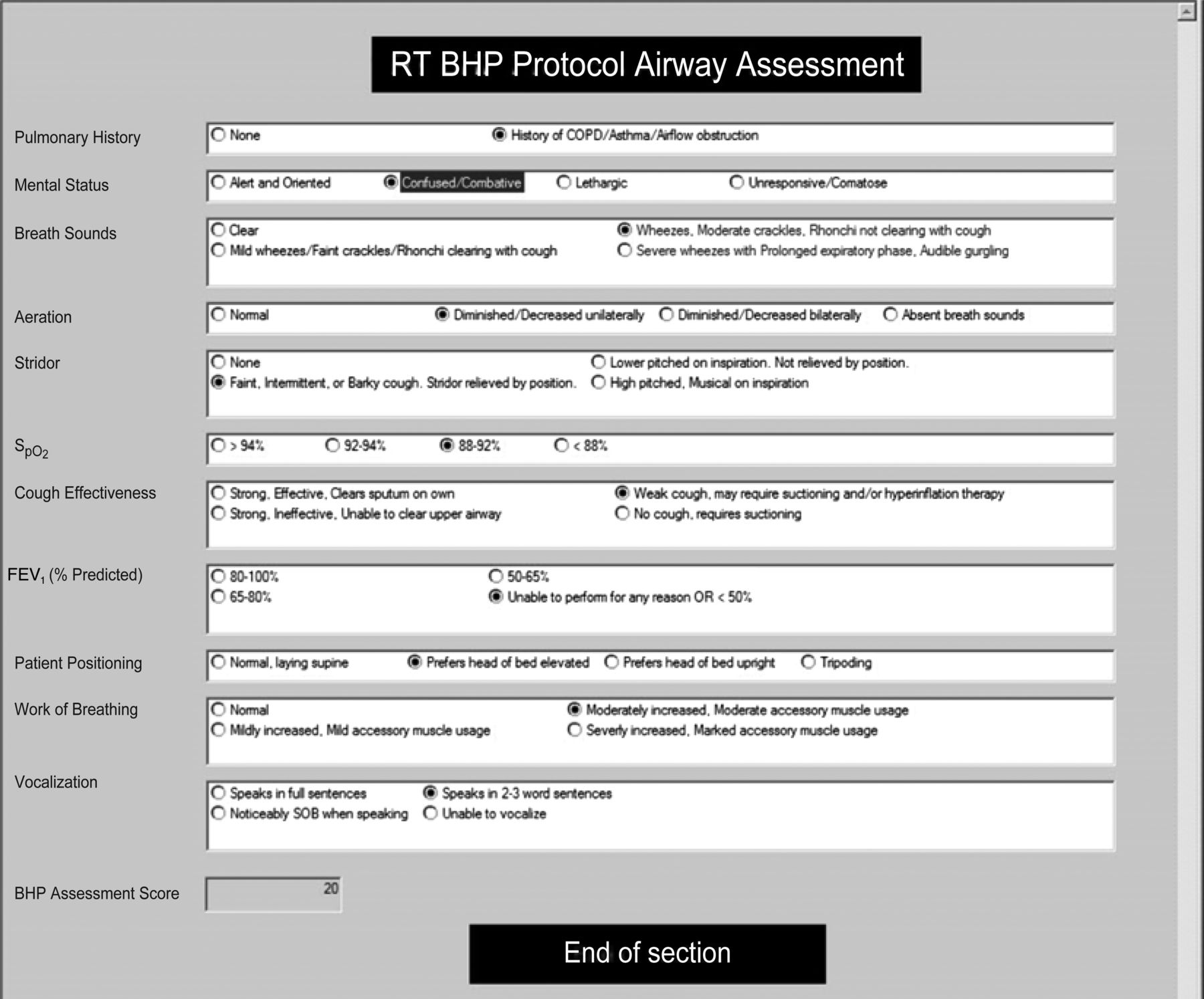
Electronic medical record showing the air-flow obstruction scoring tool.
We found this new process straightforward for those patients who were admitted for exacerbation; however, the initial data collection did not show any impact on our beginning measures of rapid response triggering for respiratory etiology. We suspected that we were missing a portion of patients admitted for COPD as well as a larger patient population with admission for reasons other than COPD but still at risk for exacerbation while admitted for other care or procedures. In response, an automated screening tool was created for patient identification through the electronic medical record system using admission and emergency department notes. We hypothesized that by using an electronic medical record-based screening tool to identify patients with COPD, we could impact hospital metrics such as length of stay (LOS), readmissions, and rapid response.
QUICK LOOK
Current knowledge
In today's health-care environment, there is an increased focus on hospital stay, readmission rates, and costs incurred due to rapid response initiations. Some specific disease processes, such as COPD, are under even more intense scrutiny with significant financial implications for health-care systems if predetermined quality metrics are not met. Many evidence-based tools, such as therapist-driven protocols, already exist and have shown beneficial for patients with COPD; however, finding these patients in a timely fashion to make a positive impact can prove to be a challenge.
What this paper adds to our knowledge
In a large, level one trauma center utilization of the electronic medical record to identify subjects with COPD was combined with a therapist-driven protocol and demonstrated a trend in decreased readmissions and stay. In addition, a significant reduction in rapid responses triggered for respiratory-specific reasons was also identified in the COPD population.
Methods
Utilizing the scoring tool and the algorithm, identified subjects were assessed by respiratory therapy staff and given a score (Fig. 1). To establish the threshold score, we previously analyzed 50 patients who were scored in the emergency department and correlated post-treatment score with emergency department disposition. The threshold score was 7. For our algorithm, subjects scoring <7 received an initial RT assessment, drug reconciliation, and brief education, with bronchodilator therapy delivered by nursing staff using a traditional nebulizer delivery system (MicroMist nebulizer, Hudson RC, Research Triangle Park, North Carolina). Those with a score ≥7 were deemed at risk and received bronchodilator therapy by the respiratory therapy department utilizing the AeroEclipseII BAN (Monaghan Medical, Plattsburgh, New York) for a minimum of 24 h with a re-assessment and new score at the 24-h mark (Fig. 2). Subjects in both groups received the same home medication reconciliation and brief education by the RT. Therapists then discussed recommendations with ordering physicians and sought additional therapies if clinically indicated. The automated screening tool utilized a database that searched admission notes and emergency department notes for key words (Table 1). In addition, this report pulled LOS, date to last admission, admitting service, and the presence of the air-flow obstruction score completed by an RT. This report was then filtered for subjects who were already receiving respiratory care services as detected by the RT Bronchopulmonary Hygiene Protocol/air-flow obstruction protocol score presence (Fig. 3). Once subjects were identified, the list was distributed to bedside respiratory therapy staff, who then assessed using the scoring tool and treated subjects according to the algorithm (see Fig. 2).

Mock screening report. MRN = medical record number, LOS = length of stay, SOB = shortness of breath, MVC = motor vehicle crash, UTI = urinary tract infection, BHP = Bronchopulmonary Hygiene Protocol/Airflow Obstruction Score.
Key Words Used for Electronic Medical Record Search Tool
Data were collected using International Classification of Diseases, 9th Revision (ICD-9) discharge codes identifying COPD. Data for stay and readmission rates were collected within a 14-month period of time, 7 months pre-intervention and 7 months post-intervention. Additional data for the ICU stay and 7- and 10-d readmission rates were also made available for analysis. Respiratory-triggered rapid responses were tracked through a database that searched template notes for data fields describing reason for rapid response initiation. Respiratory-triggered rapid responses were identified and tallied for each time frame. Subjects were then separated according to ICD-9 discharge codes into COPD as a primary or secondary diagnosis for secondary analysis. The time frame for this data collection was slightly shorter than the LOS and readmissions data time. Gathered data considered quality metrics as reported to the University Health System Consortium evaluating hospital performance and therefore, not subject to the institutional review board.
Results
The pre-intervention time period occurred from December 2013 to June 2014, and post-intervention was from July 2014 to January 2015. There were a total of 142 subjects: 68 pre- and 74 post-intervention. Mean LOS for primary diagnosed COPD decreased from 4.37 to 2.96 d (P = .10) (Table 2). Thirty-day readmission rates for COPD as the primary diagnosis decreased from 13.64 to 6.06%1 (Table 2). In addition, there was a downward trend in 10-d readmission, but no change in 7-d readmission rates was seen. All data collected were based on values reported to and evaluated by the University Health System Consortium Clinical Database/Resource Manager, used by permission of the University Health System Consortium. Rapid responses triggered for respiratory reasons in the primary COPD group were as follows: pre-intervention 21 (34.4%) and post-intervention 8 (12.7%) (P = .004). The secondary group saw a change from 318 (27.2%) pre-intervention to 296 (23.4%) post-intervention (P = .030) (Table 2). An overall decrease of nearly 17% in the number of respiratory-triggered rapid responses for all in-patients regardless of admission diagnosis was also observed (Fig. 4 and Table 2).
All Length of Stay, Readmission, and Rapid Response Data by Primary or Secondary Diagnosis With Pre-/Post-Intervention

Respiratory (RT)-triggered rapid responses in 2014.
Discussion
Utilizing the electronic medical record to screen for subjects with COPD, in combination with assessment by an RT using a unique scoring tool and accompanying algorithm, we identified a trend toward a decrease in our LOS and 30-d readmissions. In addition, we noted a significant decrease in respiratory-triggered rapid responses, which can be associated with theoretical cost avoidance. Before our study, RTs in our facility did not routinely administer bronchodilator treatments or provide assessment of this population outside of the ICU or an emergent or rapid response scenario. We suspect that having the RT do a routine, expert assessment with symptom recognition, paired with home medication reconciliation, effectively functioned as a safety net for these at-risk subjects. We believe that this intervention played a large role in decreasing the opportunity for rapid responses for respiratory occurrences, thus lowering our measured respiratory-triggered rapid response events as well as our LOS and readmissions data.
Protocolized care is a very well established and accepted strategy in health care today and is practiced frequently in respiratory therapy departments. An early study by Ford et al7 demonstrated a reduction in the number of treatments delivered to study subjects by utilizing a therapist-driven protocol with no change in subject outcomes. A more recent retrospective medical record review study by Werre et al5 compared therapist-driven protocols with physician-guided therapy for subjects with COPD admitted for acute pneumonia and demonstrated that the RT protocol arm was associated with a significant decrease in 30-d readmissions. There was no significant difference noted between groups for LOS. Our study is similar in nature because we utilized a therapist-driven protocol in comparison with physician-guided therapy and measured outcomes of LOS and readmissions. Several differences exist with our study, including the addition of a method to screen for patients independent of physician orders and the design of a pre- and post-intervention analysis. We saw similar results, however, in our 30-d readmission trends.
Although few debate the efficacy of evidence-based, protocolized care, the levels of benefit still lie in the appropriate patient identification for these strategies. In the age of electronic medical record systems, there is a vast array of data available that could be beneficial in this task. In the study by Pollack et al,8 an automated process was created by flagging subjects upon admission based on age and admitting service and then screening for eligibility to receive the influenza vaccine. Nursing then completed this screen at an appropriate time, since the tool was included in the electronic medical record documentation. For subjects who qualified to receive the vaccine, the screening form guided the nurse to further questioning and documentation, ultimately placing the order in the electronic medical record for the appropriate vaccine without requiring direct intervention from the physician or other providers. They found that this intervention improved the rate of vaccinations of hospitalized subjects as well as identifying children who had already been vaccinated before admission. Through the screening process, they were also able to find patients who had been offered the vaccine previously but declined, giving them some increased insight to the declination of vaccination in hospitalized children.8 We also leveraged our electronic medical record to screen for subjects with a history of COPD or medications that would indicate treatment for COPD. Much like the Pollack study,8 we created an electronic medical record-embedded assessment tool for decision making, which utilized clinical assessment as well as subject history. One difference was the outcome end points; Pollack et al were looking for improved compliance with a recommended guideline, whereas we were seeking improved direct patient care and measured cost avoidance. Both studies showed that the combination of initial identification and screening with an assessment tool proved to be beneficial.
We believe that our study is an example of how assessment by a trained RT can have a positive impact for patients with baseline pulmonary disease. In a busy level one trauma center such as ours, the prime utilization of RT skill sets is traditionally in the ICU setting with the clinical focus frequently on acutely deteriorating patient conditions, and crisis management. Shifting some of the focus of the RT out of the ICU and toward high-risk patients before respiratory crisis and using their critical care trained assessment skills to look for potential respiratory decline or the subtle signs of respiratory compromise may prove to be beneficial not just for patients but for cost avoidance in general.
We recognize that our study has several limitations. The time frame is relatively short, 7 months pre-intervention and 7 months post-intervention, and may not give a good reflection of seasonal illness, such as influenza, and how that impacts LOS and readmissions in this vulnerable population. A longer duration of data by matching months across years could potentially lead to stronger data and outcome conclusions. This was a single-center study in an institution that serves a unique population with a relatively low number of primary admissions for COPD but a much larger population of COPD as a secondary diagnosis. The scoring tool and algorithm has not been validated and may lack generalizability. Finally, the design was not randomized or blinded.
As COPD gains more attention and more health systems look for ways to improve care and decrease costs, the ability to find and target patients with COPD is increasingly more important. Despite our study's limitations, we have demonstrated that by leveraging the nearly instant access and patient identification abilities of the electronic medical record in combination with the critical care assessment skills of RTs and a protocolized way to assess and treat patients on an in-patient basis, meaningful cost avoidance practices can be achieved.
Many health systems have already implemented RT-trained COPD case managers to help address the complex issues surrounding this chronic disease population. We are moving forward with the implementation of an RT case manager program in our institution with the intention of improving overall disease management for this high-risk patient population.
Footnotes
- Correspondence: Karen D LaRoché RRT-ACCS, Respiratory Care Department, Box 3359761, Harborview Medical Center, 325 9th Avenue, Seattle, WA 98104. E-mail: klaroche{at}uw.edu.
Mr Hinkson has disclosed a relationship with Hamilton Medical. The other authors have disclosed no conflicts of interest.
Ms LaRoché presented a version of this paper as an Editors' Choice abstract at the AARC Congress 2015 held November 7–10, 2015 in Tampa, Florida.
See the Related Editorial on Page 1267
- Copyright © 2016 by Daedalus Enterprises









{kind=link}
{kind=link}
{kind=link}
{kind=link}