

Abstract
BACKGROUND: During noninvasive ventilation (NIV), leak around the mask may cause inadequate ventilatory support or patient-ventilator asynchrony such as auto-triggering. Some NIV ventilators may be better than others at compensating for leak.
METHODS: We bench studied 3 NIV ventilators (Vision, Carina, and Trilogy100) and 2 ICU ventilators (Puritan Bennett 840 and Evita XL) to assess how they coped with 2 leak levels and zero leak during NIV. With a 2-bellows-in-a-box lung model we simulated spontaneous breathing with tidal volumes of 300 mL and 500 mL, at pressure support of 0 and 10 cm H2O and PEEP of 5 and 10 cm H2O. We affixed the airway opening of the lung model to the mouth of a mannequin head and secured a mask on the mannequin face. We created a medium leak and a large leak with different size holes, and measured PEEP in the presence of leak. We also measured the actual pressure-support values and calculated the deviations from the set pressure-support value and the pressure-time product (PTP) of the airway opening pressure below and above baseline.
RESULTS: With the medium leak only the Vision and Carina maintained the set PEEP and pressure support. With the large leak the pressure support was decreased with all the tested ventilators. With the larger leak and pressure support of 10 cm H2O the PTP below baseline for triggering increased with 2 ventilators, and the PTP above baseline for supporting the patient's inspiratory effort decreased with all 5 ventilators. The larger tidal volume increased the PTP below baseline with all 5 ventilators and at all leak sizes.
CONCLUSIONS: Some of the ventilators compensated for leak better than others. With the larger leak none of the ventilators maintained the set PEEP or pressure support.
Introduction
During noninvasive ventilation (NIV), leakage around the mask is inevitable. Leakage is likely to decrease the PEEP, the pressure support, or other ventilatory assistance,1–4 and to cause patient-ventilator asynchrony such as auto-triggering.5–7 Recently, several ICU ventilator models have added NIV modes, but the effects of leak on the assistance provided by these ventilators have not been fully clarified. In a bench study we simulated different amounts of leak during NIV and evaluated how well 3 NIV ventilators and 2 ICU ventilators coped with the leak. Our hypothesis was that the ventilators' leak-compensation abilities would differ.
Methods
Tested Ventilators
We tested 5 ventilators: BiPAP Vision (Respironics, Murrysville, Pennsylvania), Carina (Dräger Medical, Lübeck, Germany), Trilogy100 (Respironics, Murrysville, Pennsylvania), Puritan Bennett 840 (in its NIV mode) (Puritan Bennett/Covidien, Carlsbad, California), and Evita XL NIV plus (Dräger Medical, Lübeck, Germany). We used no humidification. We used smooth-bore single-limb circuits with the Vision, Carina, and Trilogy100, and we used smooth-bore double-limb circuits (#5000, Intersurgical, Berkshire, United Kingdom) with the Puritan Bennett 840 and Evita XL.
Each ventilator was tested in CPAP mode, with set PEEP of 5 or 10 cm H2O, set pressure support of 0 or 10 cm H2O, and FIO2 of 0.21. We adjusted the triggering sensitivity and termination criteria to avoid simulator-ventilator asynchrony such as auto-triggering and inappropriate cycling (Table 1).1–3 By adjusting triggering sensitivity we were able to eliminate auto-triggering with most of the ventilators. When auto-triggering was observed, we collected data only from breaths without auto-triggering. Inspiratory rise time was set at the minimum available value. Manufacturer information on the leak-compensation ability of each ventilator is also summarized in the Table 1.
Ventilator Settings
Lung Model, Masks, and Leak
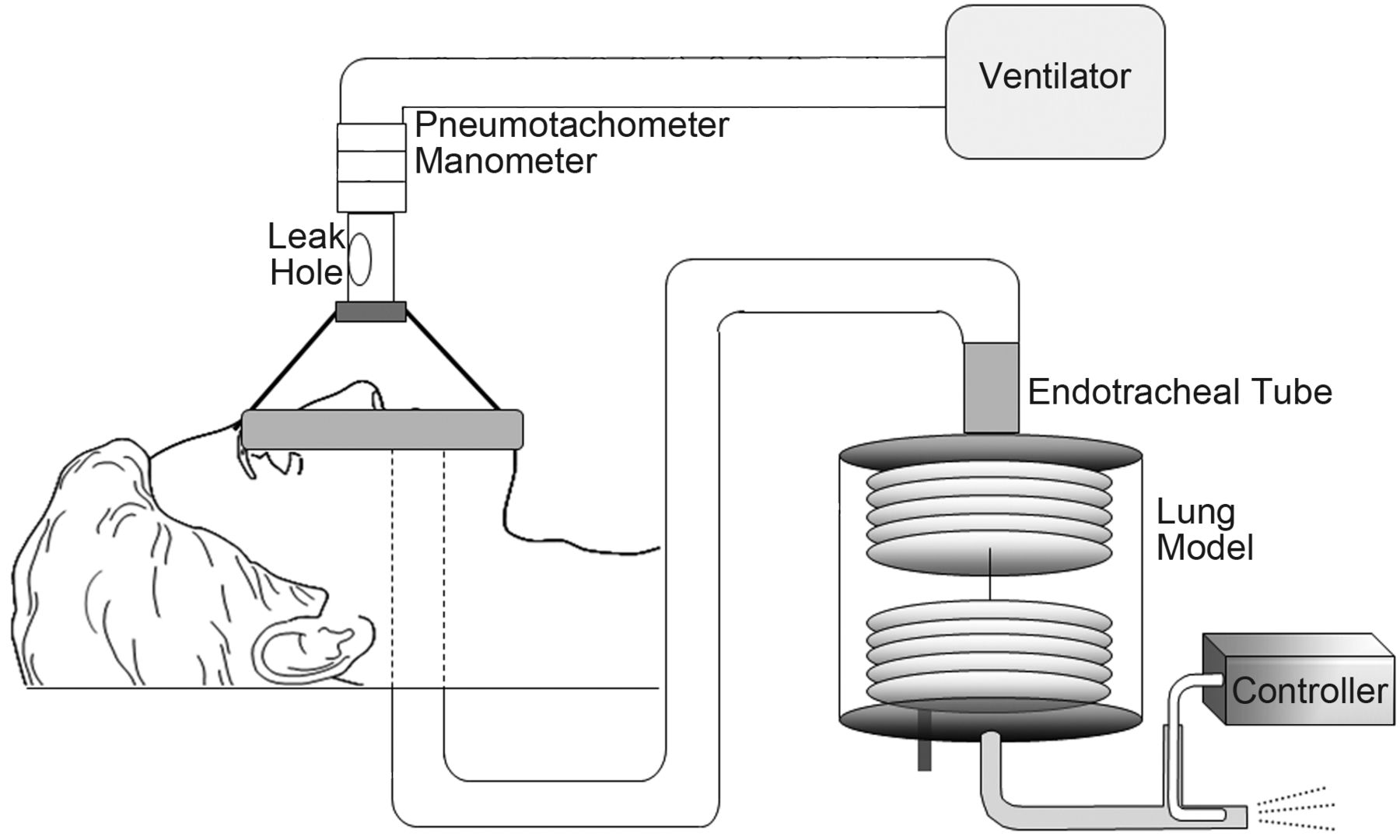
We used a 2-bellows-in-a-box type lung model (Fig. 1) that has been described elsewhere.8,9 The lung model comprises 2 bellows in a plastic airtight box. The upper bellows simulates the lung, the lower bellows simulates the diaphragm, and the space between the bellows and box simulates the pleural cavity. The diaphragm bellows is connected to a T-tube, and jet flow is injected into it to create negative pressure in the bellows. This jet flow is created with a wall gas source and a pressure regulator, regulated by a computer and a proportional solenoid valve. The movement of the diaphragm bellows inflates the lung bellows. During the expiratory phase the diaphragm bellows opens to the atmosphere and returns to its original position. For the experiments we inserted a 7-mm inner-diameter or 9-mm inner-diameter endotracheal tube in the box, resulting in measured resistances of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L, respectively. The lung model was connected to the mouth of a fiberglass mannequin head with a single smooth-bore 120-cm long, 22-mm inner-diameter tube. With the Vision and Trilogy100 we used an NIV mask (Comfort Full 2, lot 061128 1004950, Respironics, Murrysville, Pennsylvania). With the Carina, Puritan Bennett 840, and Evita XL we used a standard ventilator mask (NovaStar, lot 50010862, size L, Dräger Medical, Lübeck, Germany).

Experimental setup.
We evaluated 3 leak levels: no deliberate leak, medium leak, and large leak. To create medium and large leaks we inserted adaptors with different-size holes into the circuit. At airway pressure of 10 cm H2O the medium leak was 28 L/min and the large leak was 52 L/min.
Measurement and Calibration
After a 5-min stabilization period we started the measurements. We measured flow at the airway opening and between the lung model and the mannequin head, with a pneumotachometer (3700A, Hans-Rudolph, Shawnee, Kansas) and a differential pressure transducer (TP-602T [± 5 cm H2O], Nihon-Koden, Tokyo, Japan) (see Fig. 1). We measured the pressure at the airway opening and pressure in the simulated pleural cavity with a differential transducer (TP-603T [± 50 cm H2O], Nihon-Koden, Tokyo, Japan). We used a water manometer to calibrate the pressure transducers at 0 and 20 cm H2O. All signals were amplified, sent to an analog-to-digital converter, and recorded at 50 Hz with data-acquisition software (WINDAQ, Dataq Instruments, Akron, Ohio). We analyzed the data with analysis software (WINDAQ playback system, Dataq Instruments, Akron, Ohio).
Experimental Protocol
We set the lung model respiratory rate at 12 breaths/min and the inspiratory time at 1.0 s. Each ventilator was tested with the jet flow adjusted to create tidal volumes of 300 mL and 500 mL.
We used the pressure tracing from the simulated pleural cavity to determine the start and end of inspiratory effort (Fig. 2). When there was leak from the ventilator circuit, PEEP decreased. We defined ΔPEEP as the decrease in PEEP caused by leak. Similarly, leak affected pressurization during the inspiratory phase. The actual pressure support was defined as the pressure at the airway opening from end-expiration to end-inspiration. We defined ΔPS as the difference between the actual pressure support and the set pressure support.

Definitions of measured and calculated ventilatory variables. The dashed vertical lines indicate the start and end of inspiratory effort. PTP = pressure-time product.
As an indicator of ventilatory assistance we calculated the pressure-time product (PTP) at the airway opening (see Fig. 2). We defined trigger PTP as the area under the pressure-time curve between the onset of inspiratory effort and the return to PEEP.3,9,10 Trigger PTP reflects both the sensitivity of the ventilator in detecting inspiratory effort and the ventilator's ability to deliver high flow at the onset of inspiration.3,9 We defined inspiratory PTP as the area of the pressure-time curve above baseline during the inspiratory phase. Inspiratory PTP quantifies the speed of pressurization and the ventilator's capacity to maintain the set pressure during the inspiration. A low inspiratory PTP corresponds to under-assistance, impaired pressurization rate, and an increase in patient inspiratory effort.
Statistical Analysis
With each ventilator we analyzed data from 3 consecutive breaths. Data are expressed as mean ± SD. We used analysis of variance for comparison. Differences were considered significant when P < .01. All statistical analysis was performed with a statistics software (SPSS 11.01, SPSS, Chicago, Illinois).
Results
ΔPEEP
At each successive leak level, ΔPEEP significantly increased with all 5 ventilators (Fig. 3). Compared to the other ventilators, ΔPEEP was significantly less with the Vision and Carina. There was no difference in ΔPEEP between the tested tidal volumes, PEEP settings, or airway-resistance settings.

With large leak (versus medium leak) the difference between the set PEEP and the measured PEEP (ΔPEEP) significantly increased (P < .01) with all 5 ventilators, but ΔPEEP was significantly less with the Vision and Carina. This figure shows the pooled results from tests with PEEP of 5 cm H2O and 10 cm H2O, pressure support of zero and 10 cm H2O, tidal volumes of 300 mL and 500 mL, and airway resistance of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L.
Difference Between Set and Actual Pressure Support
At each successive leak level, ΔPS significantly increased with all the ventilators (Fig. 4). Compared to the other ventilators, in the absence of intentional leak and with medium leak, ΔPS was less with the Vision and Carina. With all 5 ventilators ΔPS was significantly greater with the larger tidal volume. The PEEP setting and airway-resistance levels did not affect ΔPS.

Difference between the set pressure support and the measured pressure support (ΔPS) with no leak, medium leak, and large leak. ΔPS significantly increased (P < .01) with each ventilator, but was less with the Vision and Carina. This figure shows the pooled results from tests with PEEP of 5 cm H2O and 10 cm H2O, tidal volumes of 300 mL and 500 mL, and airway resistance of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L.
Trigger PTP at Pressure Support of 10 cm H2O
Trigger PTP values were greater with the Vision and Trilogy100 than with the other ventilators (Fig. 5). At each successive leak level, trigger PTP increased with the Trilogy and Evita XL, but not with the other ventilators. With all the ventilators trigger PTP was significantly greater at 500 mL than at 300 mL. The PEEP settings and airway-resistance levels did not affect trigger PTP.

Trigger pressure-time product (PTP) with pressure support of 10 cm H2O, with no leak, medium leak, and large leak. This figure shows the pooled results from tests with PEEP of 5 cm H2O and 10 cm H2O, tidal volumes of 300 mL and 500 mL, and airway resistance of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L. Trigger PTP was greater with the Vision and Trilogy100 than with the other ventilators. At each successive leak level, trigger PTP significantly increased (P < .01) with the Trilogy and Evita XL, but not with other ventilators.
Inspiratory PTP at Pressure Support of 10 cm H2O
At each successive leak level, inspiratory PTP decreased with all the ventilators (Fig. 6). The PEEP settings and airway-resistance levels did not affect inspiratory PTP.
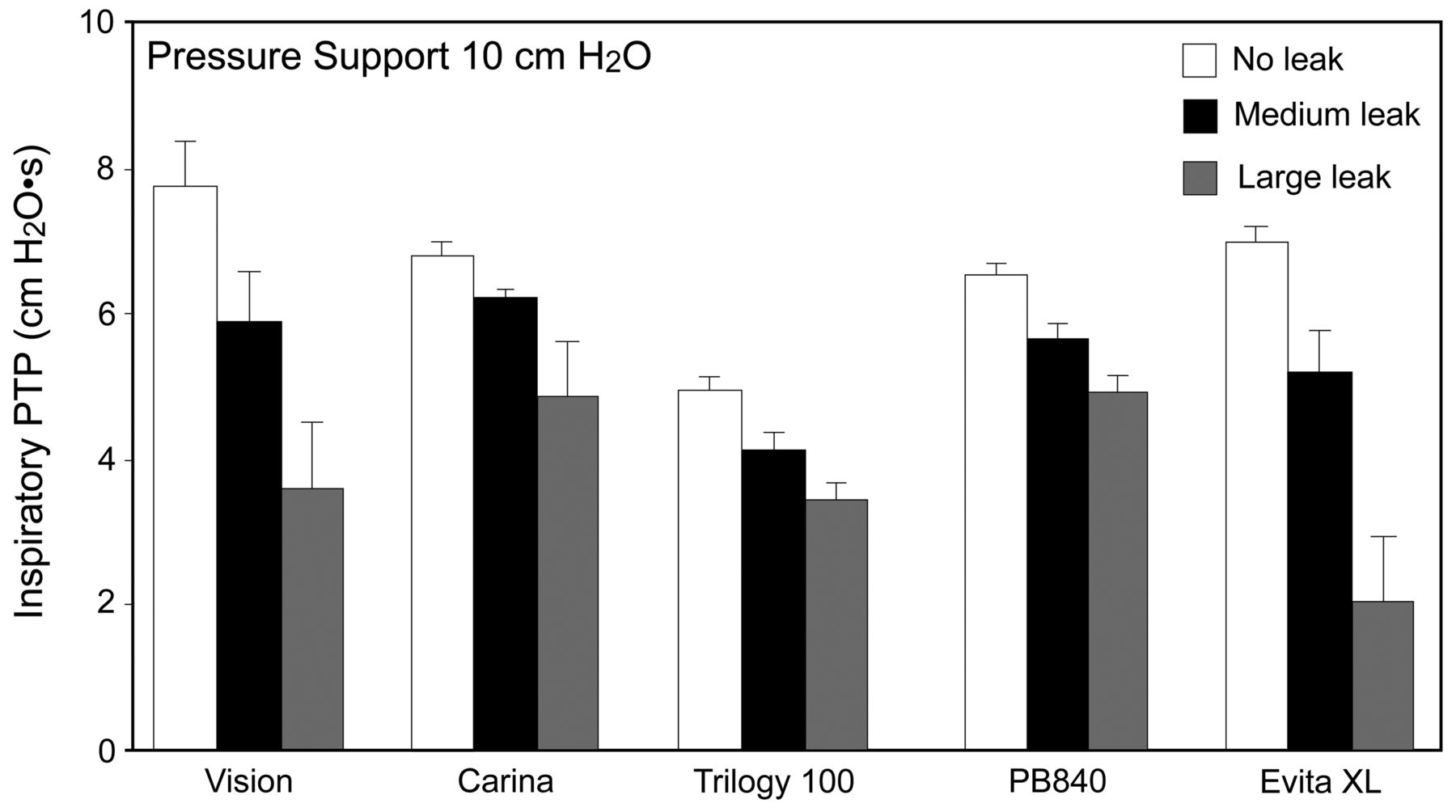
Inspiratory pressure-time product (PTP) with pressure support of 10 cm H2O, with no leak, medium leak, and large leak. This figure shows the pooled results from tests with PEEP of 5 cm H2O and 10 cm H2O, tidal volumes of 300 mL and 500 mL, and airway resistance of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L. At each successive leak level, inspiratory PTP significantly decreased (P < .01) with all the ventilators.
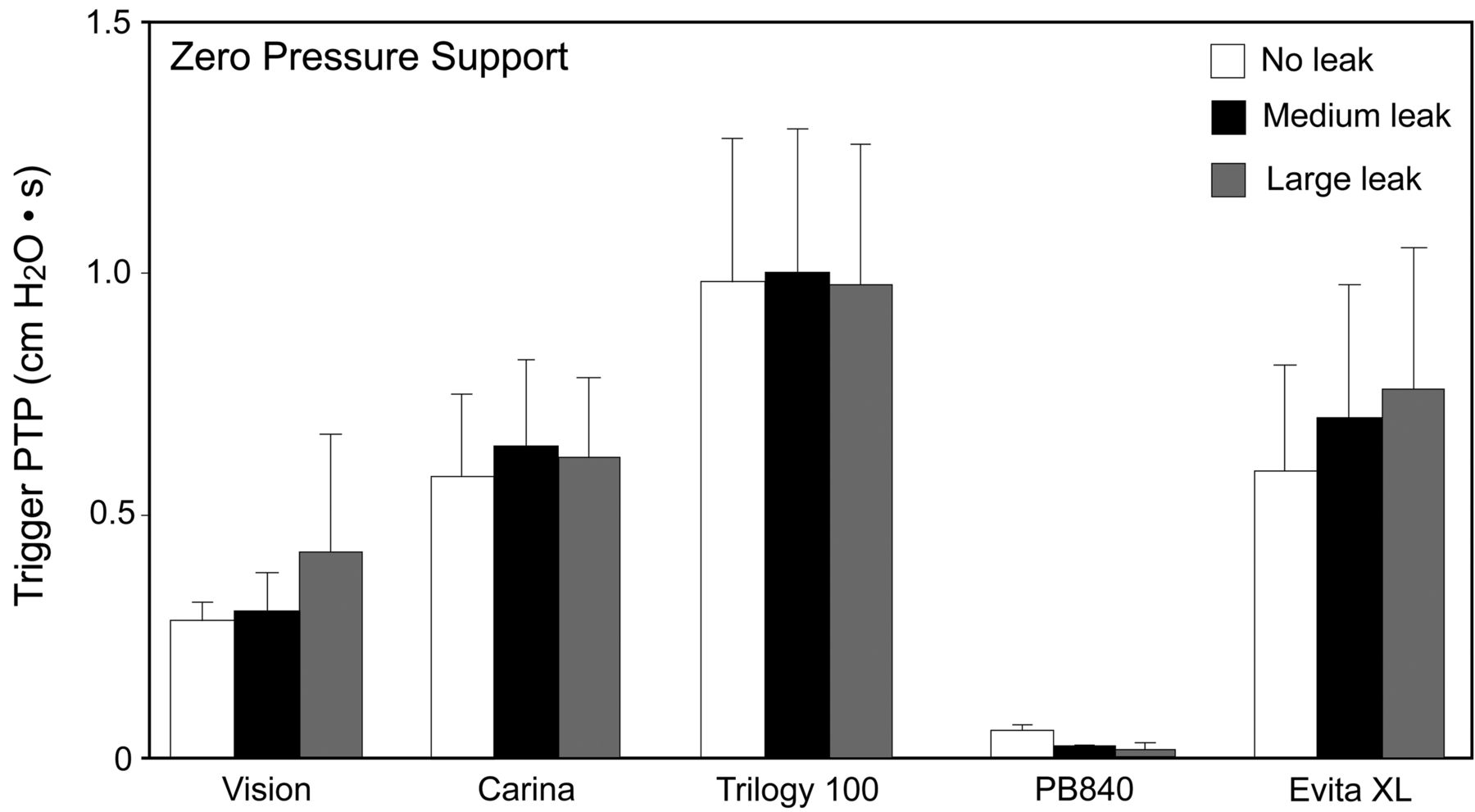
Trigger PTP at Pressure Support of Zero
Variation in the amount of leak, PEEP, or airway resistance did not affect trigger PTP (Fig. 7). With the Puritan Bennett 840 trigger PTP was less than with other ventilators. With all the ventilators the trigger PTP values were significantly greater at 500 mL than at 300 mL.

Trigger pressure-time product (PTP) with zero pressure support, with no leak, medium leak, and large leak. This figure shows the pooled results from tests with PEEP of 5 cm H2O and 10 cm H2O, tidal volumes of 300 mL and 500 mL, and airway resistance of 9.9 cm H2O·s/L and 7.8 cm H2O·s/L. Change in the amount of leak did not significantly affect trigger PTP. With the Puritan Bennett 840 the trigger PTP was less than with other ventilators.
Discussion
Our main finding is that the 3 NIV ventilators maintained PEEP and pressure support even when there was moderate leak. Leak from the ventilator circuit or mask causes patient-ventilator asynchrony11,12 and loss of PEEP and pressure support,3 which are risk factors for NIV failure.12 PEEP and pressure support decreased with leak, but the ΔPEEP and ΔPS ranged widely between the 5 ventilators. While the NIV ventilators compensated for leak better than did the ICU ventilators in their NIV modes, their capabilities were different. Although with medium leak the Vision and Carina maintained PEEP and pressure support better than did the ICU ventilators (see Figs. 3 and 4), with the large leak even the Vision and Carina did not maintain the set pressure support.
Even with the smaller leak the Trilogy100 did not maintain the set PEEP and pressure support. Because of the necessity of avoiding rebreathing, the baseline leak should be larger in NIV-specified ventilators than in ICU ventilators. In fact, with medium leak, with the Vision the baseline leak ranged from 55 L/min (at PEEP of 5 cm H2O) to 80 L/min (at PEEP of 10 cm H2O), whereas with those same conditions the baseline leak with the Puritan Bennett 840 was 23 L/min and 43 L/min, respectively. Mehta et al also reported that different NIV ventilators had markedly different leak-compensation abilities.11 Similarly, Borel et al studied the effects of leak on trigger PTP and other aspects of ventilator performance with ventilators designed for NIV.10 Vignaux et al studied the effects of leak on patient-ventilator asynchrony with a lung model2 and with patients.1,12 They first evaluated ICU ventilators and then ICU ventilators equipped with NIV modes. In contrast, we compared ventilator performance between ICU ventilators with NIV modes and ventilators designed for NIV and found wide differences between the ventilators.
During NIV, leak interferes with key ventilator functions. Comparing NIV with leak, conventional ventilation with leak, and conventional ventilation with no leak, Vignaux et al reported the effects of leak on trigger PTP with 8 ICU ventilators. Although leak increased trigger PTP with conventional ventilation, the NIV modes corrected that deficiency.2 However, that study did not evaluate the effects of larger leak. By studying 2 levels of leak, we further tested available ventilators and found that the effect of larger leak on trigger PTP differed between the NIV ventilators and the pressure-support settings. At pressure support of 10 cm H2O, trigger PTP increased with the Trilogy100 and the Evita XL, decreased with the Puritan Bennett 840, and did not significantly change with the Vision or Carina (see Fig. 5). Further study is needed to determine if those trigger-PTP changes affect clinical outcomes. With zero pressure support the trigger PTP was not affected by the amount of leak (see Fig. 7). Vignaux et al also compared the effects of leak on inspiratory PTP during conventional mode and NIV mode.2 We found that larger leak reduced inspiratory PTP with the 3 NIV ventilators (see Fig. 6). Ferrerira et al found that to avoid auto-triggering and ensure adequate ventilation in NIV mode, most of their tested ICU ventilators required adjustment of triggering sensitivity and cycling criteria.13 We also found that painstaking readjustment of triggering sensitivity and cycling criteria was necessary with the ICU ventilators, but not with the NIV ventilators.
Limitations
Our findings cannot be directly applied to clinical settings. During each of our test protocols the leak was constant, which is unlikely in clinical practice. The leaks we created were relatively large (28 L/min and 52 L/min at 10 cm H2O airway pressure), but previous studies also applied large leaks.10,11,13 To simulate the effect of increased airway resistance on ventilator performance in the presence of leak we investigated only 2 levels of system resistance, but a much wider range of lung mechanics would be observed in clinical practice. Although we investigated only 2 levels of pressure support, PEEP, and tidal volume, including higher pressure settings or drastically different tidal volumes would provide more insight into the performance of these ventilators. Also, this study could have been done with healthy human subjects, which would have made it more applicable to the clinical setting. However, our use of a lung model instead of human subjects made the study practical in a short period and with no human risk, to compare 5 ventilators under multiple simulated clinical situations.
Conclusions
PEEP and pressure support decreased when leak was greater during NIV, and some ventilators compensated for leak more effectively than others.
Footnotes
- Correspondence: Hideaki Imanaka MD, Emergency and Disaster Medicine, Tokushima University Hospital, 3-18-15 Kuramoto Tokushima, Japan 770-8503, E-mail: imanakah{at}clin.med.tokushima-u.ac.jp.
The authors have disclosed no conflicts of interest.
See the Related Editorial on Page 1857
- Copyright © 2011 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}