

Introduction
Rosai-Dorfman disease (RDD), also known as sinus histiocytosis with massive lymphadenopathy, is a benign proliferation of histiocytes. It was first described in 1969 by Rosai and Dorfman.1 This disease mainly affects superficial and deep lymph nodes. Involvement of extranodal tissues has been reported in 43% of cases with RDD,2,3 but involvement of the lower respiratory tract is rare.4 Here we report a case of RDD affecting the lung.
Case Summary
A 44-year-old man was admitted with a 4-month intermittent fever in June, 2006. He had been well, with no major medical problems. Physical examination did not reveal palpable lymphadenopathy. Routine hematological examination showed anemia and leukocytosis (20.41 × 109 cells/μL), with increased neutrophil differentiation (81.7%) and decreased lymphocyte differentiation (9.5%). Laboratory investigations also revealed high erythrocyte sedimentation rate (42 mm/h) and hypergammaglobulinemia (21.1%). No abnormalities were found by ultrasonography of the abdomen. Computed tomography scans of the thorax showed a 50 × 40 mm soft tissue mass in the left lower lobe of the lung (Fig. 1). The presumptive diagnoses considered were lung abscess or malignancy.
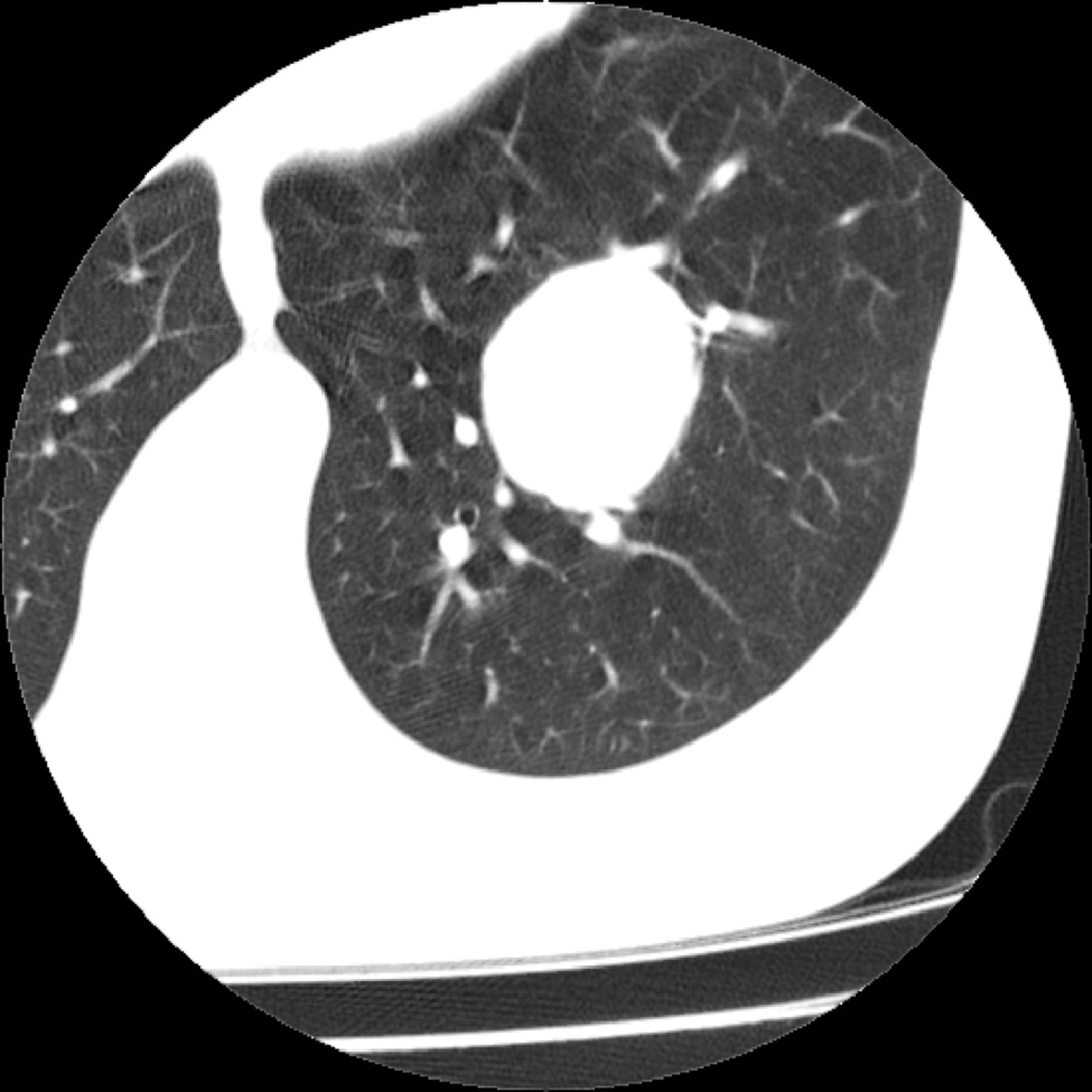
Well circumscribed mass within the left lower lobe of the lung on computed tomography scan.
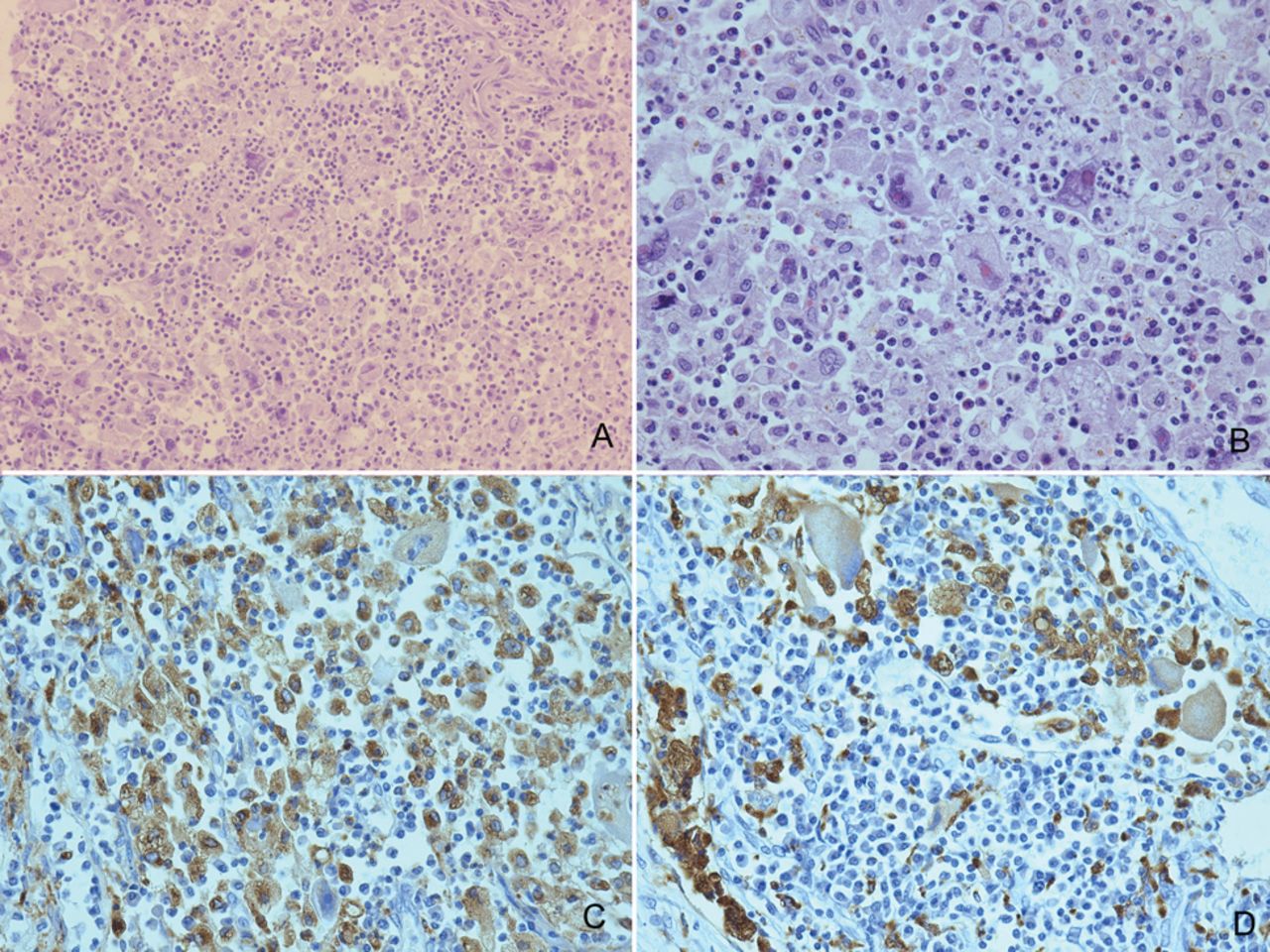
The left lower lobectomy was carried out. The mass measured 50 × 40 × 35 mm. It was relatively circumscribed, with a yellow-white color. There was caseous necrosis in the center. Histologically, the lesion displayed diffuse aggregates of large histiocytoid cells mixed with lymphocytes, plasma cells, neutrophils, and eosinophils (Fig. 2). The histiocytoid cells had abundant cytoplasm, vesicular nuclei, and prominent nucleoli (see Fig. 2). Emperipolesis of lymphocytes, plasma cells, neutrophils, and erythrocytes was found in the cytoplasm of these cells. In the adjacent tissue the alveolar wall thickened and type II epithelium proliferated. The alveolar spaces were filled with foamy cells. There were 8 hilar lymph nodes measuring 4–8 mm in diameter. All were diagnosed as reactive hyperplasia.

A: Lesion showing diffuse aggregates of large histiocytoid cells with abundant cytoplasm that admixed with lymphocytes, plasma cells, and neutrophils (hematoxylin and eosin, magnification × 100). B: Histiocytoid cells with intact lymphocytes, neutrophils, and erythrocytes within the cytoplasm (hematoxylin and eosin, magnification × 400). C: Immunohistochemistry showed S-100 positively (Envision, magnification × 400). D: Immunohistochemistry showed CD68 positively (Envision, magnification × 400).
Immunohistochemically, the histiocytoid cells were positive for S-100, CD68 (see Fig. 2), and vimentin. Immunohistochemical stain for CD1a, CD20, CD30, CD45RO, CD79a, CK, TTF-1, synaptophysin (Syn), cgA, SMA, MyoD1, HMB45, and melan-A were negative. Special staining was performed, including acid-fast stain and periodic acid Schiff reaction, which showed no acid-fast bacilli or fungi. Epstein-Barr virus (EBV) was evaluated by in situ hybridization, with a negative result.
The final diagnosis was RDD of the lung. Fifty-nine months following the diagnosis, the patient remained free of the disease, without any other therapy.
Discussion
RDD is a rare disease with a benign nature. The definite etiology of RDD remains unknown. Of reported cases, serologic evidence of EBV was found in 3 of 6 cases, but latent or lytic EBV infection was not found within the histiocytes.5 Our case was also negative for EBV detection.
Most patients present with bilateral massive painless cervical lymphadenopathy, accompanied by fever and weight loss. Laboratory investigations may also reveal anemia, leukocytosis, high erythrocyte sedimentation rate, and polyclonal hypergammaglobulinemia.6 In approximately 43% of the cases, different extranodal sites have been reported to be involved, such as skin, nasal cavity, orbit, salivary gland, central nervous system, kidney, liver, pancreas, oral cavity, breast, and bone marrow, 23% of which have extranodal involvement only.2,3 Involvement of the larynx, lung, and pleura has been reported in only a few cases.7 Only 2% of the cases have lower respiratory tract involvement.4 Cartin-Ceba et al found intrathoracic manifestations of RDD were relatively common and included mediastinal lymphadenopathy, airway disease, pleural effusion, cystic, and interstitial lung disease. They identified mediastinal lymphadenopathy as the most common intrathoracic manifestation of RDD (66%).8 However, our patient showed pulmonary mass with no mediastinal lymphadenopathy. Three cases of RDD with detailed data on the lung have been reported.2,3,9 Their clinical features are summarized in the Table. All the 3 cases, together with ours, are middle-age or elder adults with no smoking history. These patients presented with no specific symptoms of the lung. All of them have a good prognosis without any additional treatment. Anemia, leukocytosis, high erythrocyte sedimentation rate, and hypergammaglobulinemia were also found in our case, while the other 3 cases showed no hematological abnormalities.
Four Cases of Rosai-Dorfman Disease of the Lung: Clinical Manifestations and Follow-up Data
The morphological features of RDD show infiltration of large histiocytoid cells admixed with lymphocytes, neutrophils, and plasma cells. The histiocytoid cells have abundant cytoplasm, vesicular nuclei, and prominent nucleoli. Variable numbers of intact lymphocytes, plasma cells, neutrophils, and erythrocytes are seen within the cytoplasm of these histiocytoid cells, which was called emperipolesis. The disease needs to be differentiated from carcinoma, melanoma, lymphoma, Langerhans cell histiocytosis, and tuberculosis. The expression of S-100 and CD68 is useful in making the diagnosis. Our case displayed sheets of large histiocytoid cells intermittent with lymphocytes, plasma cells, and neutrophils. Focal phagocytosis was seen in the histiocytoid cells. These histiocytoid cells were merely positive for S-100, CD68, and vimentin. Our case met the diagnostic criteria of RDD.
Local surgery, radiotherapy, steroids, and cytotoxic drugs had been used in the treatment of RDD.10 The disease showed a benign course. Some reports show that pulmonary RDD has a worse prognosis, compared with the nodal form, with death occurring in approximately one third of the cases, and a progressive condition in more than one third.3 However, Cartin-Ceba et al found the prognosis of patients with RDD and intrathoracic manifestations was relatively good.8 The prognosis of all these 4 RDD cases of the lung is good. All of them have received only lobectomy or biopsy, without any further therapies.
In conclusion, RDD is a rare disorder in the lung, which might be misdiagnosed on computed tomography scan. An accurate pathologic diagnosis is of great importance in that it can help avoid any unnecessary treatment.
Teaching Points
RDD is a benign proliferation of histiocytes. Involvement of the lung is rare, and might be misdiagnosed as abscess or tumor based on computed tomography scanning.
The diagnosis is made on the basis of characteristic histological findings in combination with immunohistochemical features in tissue biopsy specimens. The key pathological feature of RDD is empripolesis. The expression of S-100 and CD68 is useful in making diagnosis.
The prognosis of patients with RDD of the lung is relatively good.
Acknowledgments
We thank Junqing Dang for help in revising the paper.
Footnotes
- Correspondence: Dong Tian MB, Department of Pathology, Affiliated Hospital of Binzhou Medical College, Binzhou Medical College, Binzhou, Shandong, China, 256600. E-mail: zoupingzb{at}sina.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}