

Introduction
Tuberculous pleural effusion occurs in approximately 5% of patients with Mycobacterium tuberculosis (TB) infection1 and accounts for 4% of all TB cases in the United States.2 Diagnosis is challenging, with 48–96% of tuberculous pleural effusions negative by sputum acid-fast bacilli (AFB) stain and culture. Thoracentesis is frequently performed and shows an exudative, lymphocytic pleural effusion in more than 90% of cases,3 but direct examination reveals AFB in less than 10% of cases.4 As AFB stain and cultures are often negative and biomarkers cannot guide therapy, more invasive diagnostic measures are usually required. The following case illustrates the clinical presentation and diagnostic approach in a typical case of suspected tuberculous pleural effusion in an elderly man.
Case Summary
A 75-year-old Chinese man with well controlled hypertension and type 2 diabetes presented to clinic with a 4 week history of cough, for which he had previously been prescribed azithromycin. His cough was mostly dry, with occasional white frothy sputum and no blood. He additionally complained of night sweats over the past few days, and dyspnea on exertion. He had subjective weight loss over the past 10 days due to loss of appetite, but no shortness of breath at rest, chest pain, fevers, or sick contacts. He had never smoked and had no known past exposures to TB. He had worked as a tailor his entire life. He was born in China, lived there for 14 years, lived in Hong Kong for 40 years, and then moved to the United States 22 years prior to presentation. He had not traveled in the past few years.
The patient was afebrile, with normal blood pressure, a heart rate of 110 beats/min, and SpO2 of 96% while breathing room air. Physical examination revealed dullness to percussion and decreased breath sounds throughout his right hemithorax, with normal lung sounds on the left. His white blood cell count was 8.360 × 103 cells/mL, with 73% neutrophils and 14% lymphocytes, and platelets 550 × 103 cells/mL. Basic chemistry was normal with the exception of a serum sodium of 130 mEq/L and glucose of 197 mg/dL. A chest radiograph (Fig. 1) revealed a large right pleural effusion. Human immunodeficiency virus (HIV) test was negative. Expectorated sputum revealed 3 negative stains and cultures for AFB, in addition to being polymerase chain reaction (PCR) negative. The quantiferon TB test was indeterminate.

Upright portable chest radiograph obtained on hospital admission, showing a right-sided pleural effusion occupying most of the hemithorax.
Thoracentesis removed 750 mL of clear yellow fluid that had 3,319 red blood cells/μL, and 1,205 white blood cells/μL, with 1% neutrophils, 94% lymphocytes, and 5% macrophages and mesothelial cells. The glucose was 144 mg/dL, albumin 2 g/dL, amylase 45 units/L, pH 7.47, total protein 4.9 g/dL, and lactate dehydrogenase 300 units/L. Adenosine deaminase was elevated at 84.9 units/L. Serum total protein was 7.5 g/L and serum lactate dehydrogenase 194 units/L. An AFB stain of the pleural fluid was negative.
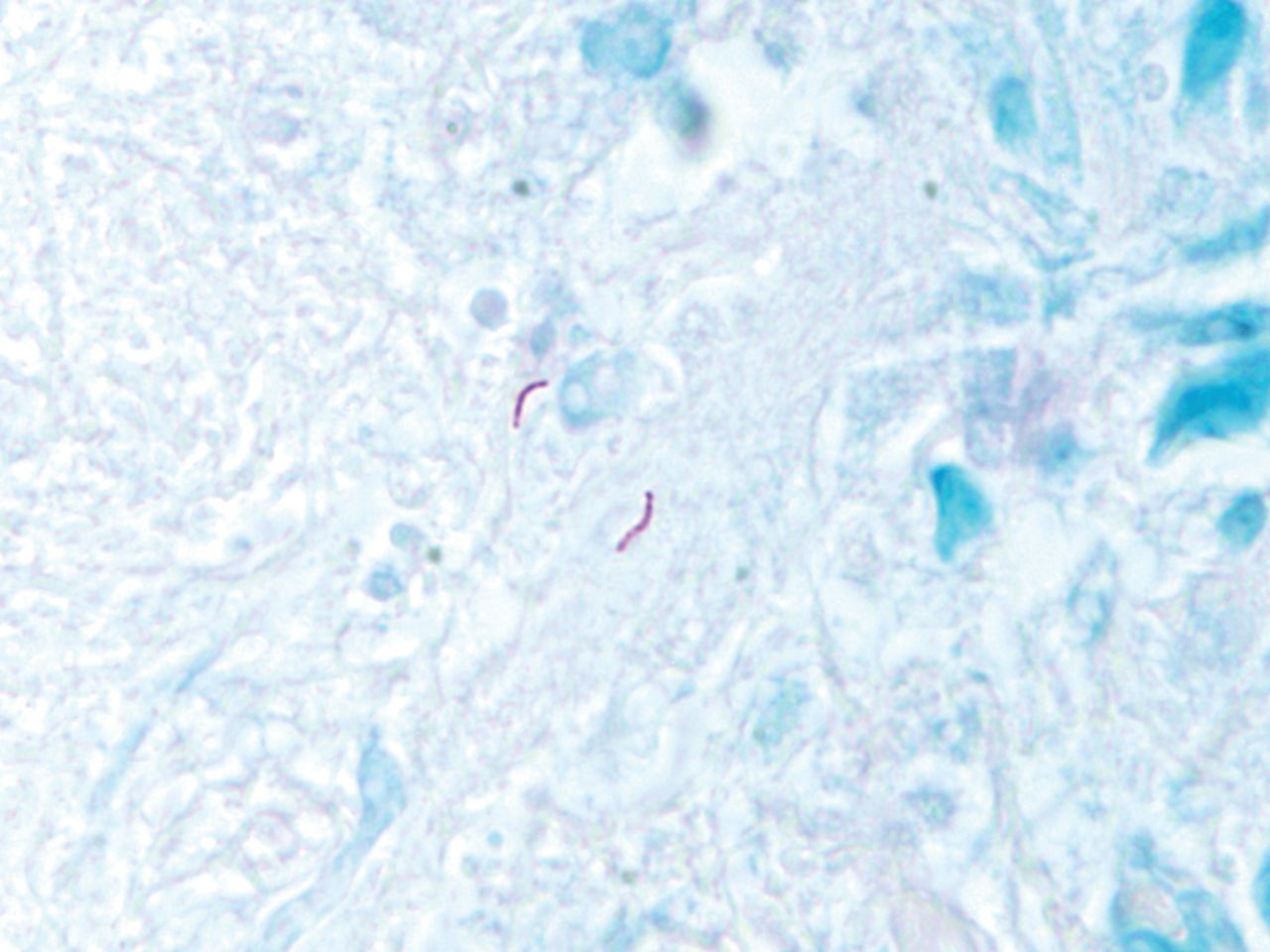
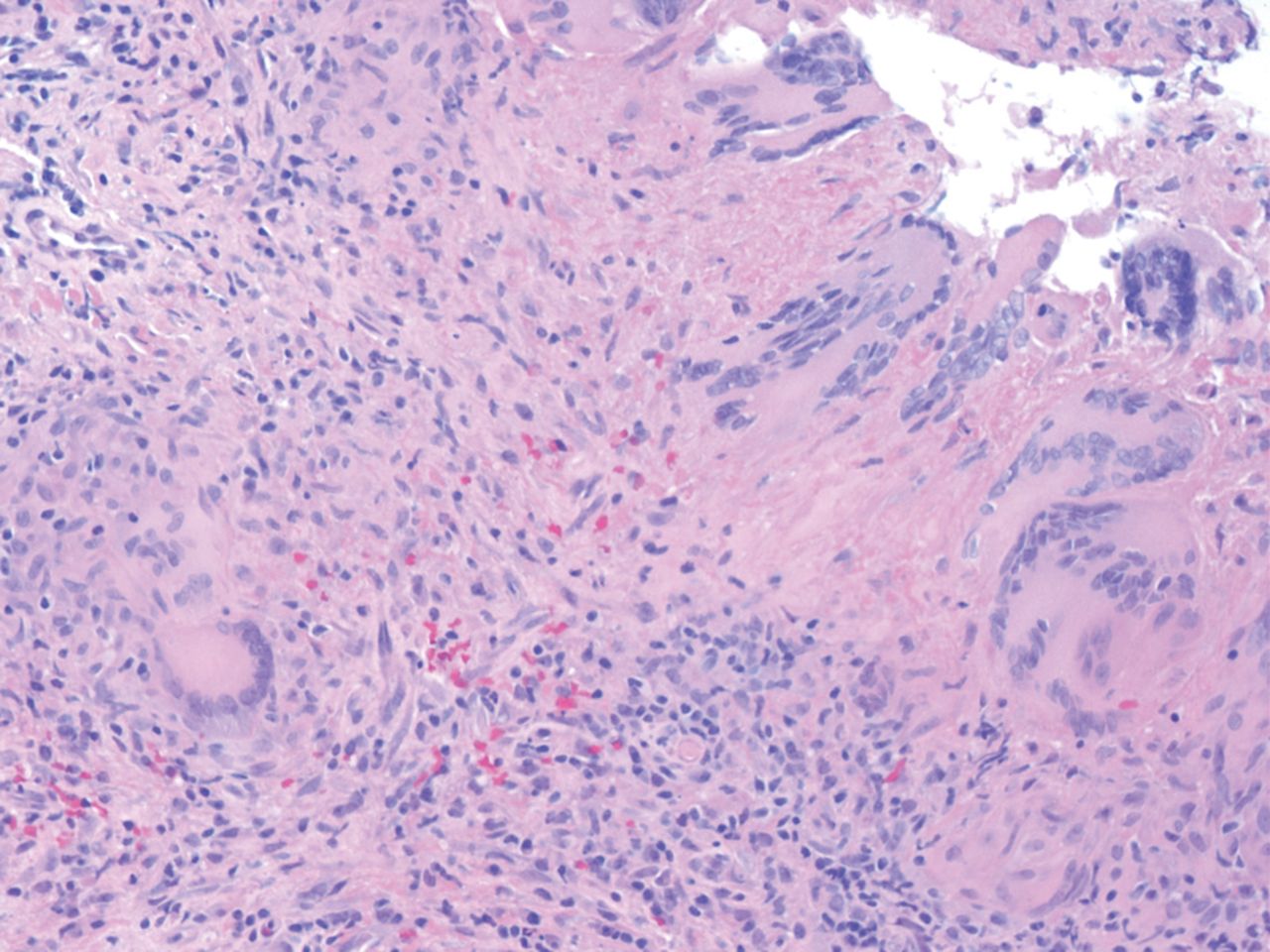
A percutaneous, closed pleural biopsy was performed, using an Abrams needle, yielding 6 pieces of pleural tissue that revealed granulomatous pleuritis with focal necrosis, positive by AFB stain (Figs. 2 and 3) and PCR (hsp65 DNA probe).

Ziehl-Neelsen (acid-fast bacilli) stain of tissue obtained from pleural biopsy. Two acid-fast bacilli are seen in the center of the field.

Hematoxylin and eosin stain of tissue obtained from pleural biopsy. Multiple red-staining organisms are seen, surrounded by granulomatous inflammation.
After the pleural biopsy was performed, the pleural fluid from the thoracentesis was PCR positive (hsp65 DNA probe) and Mycobacterium tuberculosis grew in the pleural fluid culture. Additionally, during hospitalization the patient was found to have elevated liver enzymes, which resulted in a new diagnosis of hepatitis B. Anti-tuberculosis therapy was begun with isoniazid, rifampin, ethambutol, and pyrazinamide, anticipating a total course of treatment of 6–9 months.
Discussion
This is a classic case of tuberculous pleural effusion, as it presented subacutely in a man with a cough, night sweats, weight loss, dyspnea, and a unilateral pleural effusion. The male-to-female ratio of tuberculous pleural effusions is 2:1, and it presents subacutely in 70% of patients. Over 95% of TB pleural effusions are unilateral.2 Weight loss, initial leukocyte count under 11,000 per mL, and poor clinical response to empirical antibiotics are all independent factors suggesting tuberculous pleurisy.3 Not typical in this patient, only 30% of patients are over age 65, and other common presenting complaints not present in this patient are fever and pleuritic chest pain. Additionally, less than 18% of TB pleural effusions occupy more than two thirds of the hemithorax.2 Though HIV testing was negative, all patients with extrapulmonary TB should be tested for HIV infection, as HIV has been associated with the doubling of the incidence of extrapulmonary TB.4
Central to the evaluation of patients with suspected pleural TB is the diagnostic approach. The initial step is sputum culture and stain for AFB. Though traditionally the yield of positive sputum stains and cultures has been low (under 10% in those with no evidence of pulmonary TB on chest radiograph), a recent study has demonstrated that sputum induction resulted in diagnosis in 52% of patients with normal chest radiographs.5
With unilateral pleural effusions that are negative by sputum Gram stain and culture, thoracentesis is the next step to distinguish among parapneumonic, malignant, and tuberculous pleural effusions. With tuberculous pleural effusions, pleural fluid is an exudate with lymphocytic predominance in 90% of cases.3 Unfortunately, direct examination of pleural fluid detects AFB in less than 10% of cases.4 Biomarkers that can help distinguish tuberculous pleural effusions from other causes of pleural effusions are adenosine deaminase (ADA) and interferon γ (IFNγ). Adenosine deaminase appears to be particularly useful as a screening test, with a cutoff of 35 units/L being 93% sensitive and 90% specific. However, false positives are frequent, with 70% of empyemas and 57% of lymphomas also producing elevated ADA levels.6 An ADA level under 40 units/L is said to virtually rule out the diagnosis of TB.2 IFNγ has also been used to aid in diagnosing tuberculous pleural effusions. A meta-analysis published in 2007 revealed a sensitivity of 89% and a specificity of 97%.7 DNA probes have additionally been used to reveal the presence of TB, but are marred by a low sensitivity of 62–76.5%, though specificity is 91–97%.8
Pleural biopsies resulted in diagnosis of 88% of those with tuberculous pleural effusions.9 Though pleural biopsy has fallen out of favor with the advent of medical thoracoscopy for tuberculous pleural effusions, when other factors such as training and cost are taken into account, the pleural biopsy continues to have a role in the diagnosis of tuberculous pleural effusion.10
With medical thoracoscopy, also known as pleuroscopy, complication rates are reported to be 2–5%, with diagnostic accuracy for tuberculous pleural effusions of 100%.11,12 This procedure may be especially useful for loculated pleural effusions or when lysis of adhesions is necessary.2
Figure 4 presents an algorithmic approach to diagnosing pleural TB. According to an algorithm published in Lung, a patient should be treated for TB without pleural biopsy in the case of a lymphocytic exudate, negative cytology, and elevated ADA, in an area of moderate to high incidence or low M. tuberculosis resistance, and should undergo pleural biopsy only if the incidence of TB is low in the region or the rate of multiple-drug-resistant M. tuberculosis is high.2 In this case, treating based on ADA levels and a pleural fluid lymphocytic exudate may have been enough to commit this patient to 6 months of a multidrug regimen without a tissue diagnosis. However, the use of biomarkers to aid in diagnosis leaves the possibility of treating multiple-drug-resistant TB inappropriately, and those with suspicion of multiple-drug-resistant TB should undergo further testing to distinguish the strain.

Algorithm for diagnostic evaluation of a suspected tuberculous pleural effusion. AFB = acid-fast bacillus. ADA = adenosine deaminase. IFNγ = interferon gamma. VATS = video-assisted thoracoscopic surgery.
Teaching Points
The diagnosis of tuberculous pleural effusion remains a challenge, with 48–96% of sputum and greater than 90% of pleural fluid negative for AFB stain and culture.
Biomarkers ADA and IFNγ can support the diagnosis, but definitive diagnosis with pleural biopsy or thoracoscopy is necessary in patients living in areas with low prevalence of TB or those suspected to have multiple-drug-resistant TB.
Pleural biopsy remains a reasonable diagnostic tool, though medical thoracoscopy is gaining favor.
Footnotes
- Correspondence: Alison M Bays MD MPH&TM, Department of Medicine, Harborview Medical Center, 325 Ninth Avenue, Box 359892, Seattle WA 98104. E-mail: alisonmb{at}uw.edu.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}