

Abstract
BACKGROUND: It is well established that the work rate increment size affects the duration of test and physiological responses to exercise during cycling in patients with COPD. However, this has never been tested for incremental step tests.
OBJECTIVE: To compare the exercise tolerance time, cardiopulmonary stress, and perception of effort between the Chester step test (CST) and a modified incremental step test (MIST).
METHODS: Thirty-two subjects with COPD (FEV1 50 ± 15% of predicted) were randomized to perform the CST and MIST on the same day, an hour apart, on a single step (20 cm high). During tests, pulmonary gas exchange was measured continuously by a portable metabolic system.
RESULTS: CST had shorter duration and also lower number of steps, in comparison with MIST. However, similar cardiopulmonary responses were observed at exercise peak: oxygen uptake (V̇O2) 1.22 ± 0.59 L/min vs 1.24 ± 0.55 L/min, minute ventilation (V̇E) 30.8 ± 12.7 L/min vs 30.0 ± 11.7 L/min, heart rate 86 ± 13 beats/min vs 85 ± 13 beats/min, and SpO2 87 ± 7% vs 87 ± 6%. Dyspnea and leg fatigue scores when correcting for exercise duration were higher for CST.
CONCLUSIONS: The slower the work rate increment during step test, the higher the exercise tolerance. Regardless of the work rate increment, cardiopulmonary stress and exertion effort at peak exercise were equivalent between tests.
Introduction
Reduced functional capacity is one of the most important systemic consequences of COPD.1 Therefore, the assessment of exercise tolerance has become a relatively routine procedure in evaluation of patients with COPD. Field tests have been widely used to measure functional capacity in pulmonary rehabilitation programs.
Among the most common field tests, the step test stands out for its low cost, simplicity, and portability, the latter being an advantage over walking tests. Similarly to walking tests such as the 6-min walk test (6MWT) and the shuttle walk test, step tests can be either self-paced2,3 or externally paced.4–6 In addition, as well as the cycle ergometer and treadmill protocols, step test can be performed with constant4–6 or incremental work rate.7
The Chester step test (CST) combines the characteristics of being a test both externally paced and with an incremental pattern, which makes it suitable for evaluation of exercise tolerance. Although CST was originally developed to assess aerobic capacity in healthy subjects,7 it has recently been used in lung diseases.8–10 In subjects with COPD, our group has recently shown that the CST had a very short duration (< 4 min), and just 22% of the subjects (7/32) were able to complete 3 out of 5 stages of the CST.10 Moreover, we have speculated that the initial cadence associated to the work load incremented at each stage makes the original CST a difficult protocol to be performed by subjects with COPD, who present a wide range of exercise tolerance at similar levels of pulmonary impairment.
Therefore, this study aimed to test a modified version of the CST for use in subjects with COPD. The modification consisted in reducing both the initial cadence and the increment rate (number of steps/min) throughout the test.11 This adaptation was based on studies that demonstrated the influence of the work rate increment on the duration of exercise,12–16 but this effect has never been tested with incremental step test protocols. We then hypothesized that the exercise tolerance (the duration and the maximum work load) is higher during the modified incremental step test (MIST) than during the CST with equivalent cardiopulmonary responses at peak exercise,17 because both tests are limited by symptoms in patients with COPD. The objective of this study, therefore, was to compare the exercise tolerance time, cardiopulmonary stress, and perception of effort between the CST and a MIST in subjects with COPD.
QUICK LOOK
Current knowledge
Among the most common field tests for assessment of pulmonary disability, the step test is often used, owing to low cost, simplicity, and portability, compared to walking tests. These tests can be self-paced or externally-paced, and cycle ergometer and treadmill protocols can be performed with constant or incremental work rate.
What this paper contributes to our knowledge
In a group of COPD patients, metabolic, cardiovascular, and respiratory responses during the Chester step test and a modified incremental step test were similar at peak exercise, but differences in increment size result in a longer duration and higher total number of steps during the modified incremental step test. The slower the work rate in the incremental step results in a higher exercise tolerance.
Methods
Study Subjects
We prospectively studied 32 consecutive subjects with COPD (FEV1 < 70% of predicted), who were ages 50–87 years and who were not dependent on oxygen supplementation at rest. No subjects were receiving medications, such as β blockers, vasodilators, diuretics, digitalis, or anti-arrhythmics, that could affect exercise responses. Patients who had exacerbation, who had cardiovascular conditions that could limit their exercise participation, and who were unable to perform tests on any locomotor or neurological conditions were excluded. The study was previously approved by the institutional ethics committee, and all subjects signed a consent form.
Protocol
This was a prospective, cross-sectional study. Both the CST and MIST were performed on the same day, 1 hour apart, in a randomized order. The randomization was performed with the use of sealed and opaque envelopes that contained a card indicating either the CST or the MIST. A researcher randomly selected one of these envelopes, which determined which test would be performed first (CST or MIST). After a detailed explanation of the protocol, the subjects were familiarized with the randomized test that was to be performed first. The familiarization procedure lasted for about a minute and was undertaken just to verify whether the subjects were able to follow the pace imposed by the sound stimulus, and to ensure that they understood how the tests would be performed. On a subsequent day, the 6MWT was conducted according to American Thoracic Society guidelines,18 and the test with the longest distance was used for correlation with the CST and the MIST. Supplementary oxygen was not administered during any of the tests.
Chester Step Test
CST was performed on a 20 cm high single step. The rhythm was dictated by sound signals previously recorded on a compact disc. Briefly, the CST starts with a pace of 15 steps per minute (stage 1), which increases every 2 min to 20 (stage 2), 25 (stage 3), 30 (stage 4), and 35 steps (stage 5) per minute7 (Fig. 1). Therefore, the total time of CST is 10 min. In the original description, the test was finished when the subject reached a heart rate 80% of predicted maximum (220 – age in years). However, the majority of patients with COPD stopped the exercise prematurely without reaching that level of heart rate. The test was interrupted either by the subject because of symptoms (dyspnea and/or leg fatigue) or by the physiotherapist when the subject was unable to follow the rhythm for a period of 15 seconds.10 The work performed in the test was estimated by the following equation:
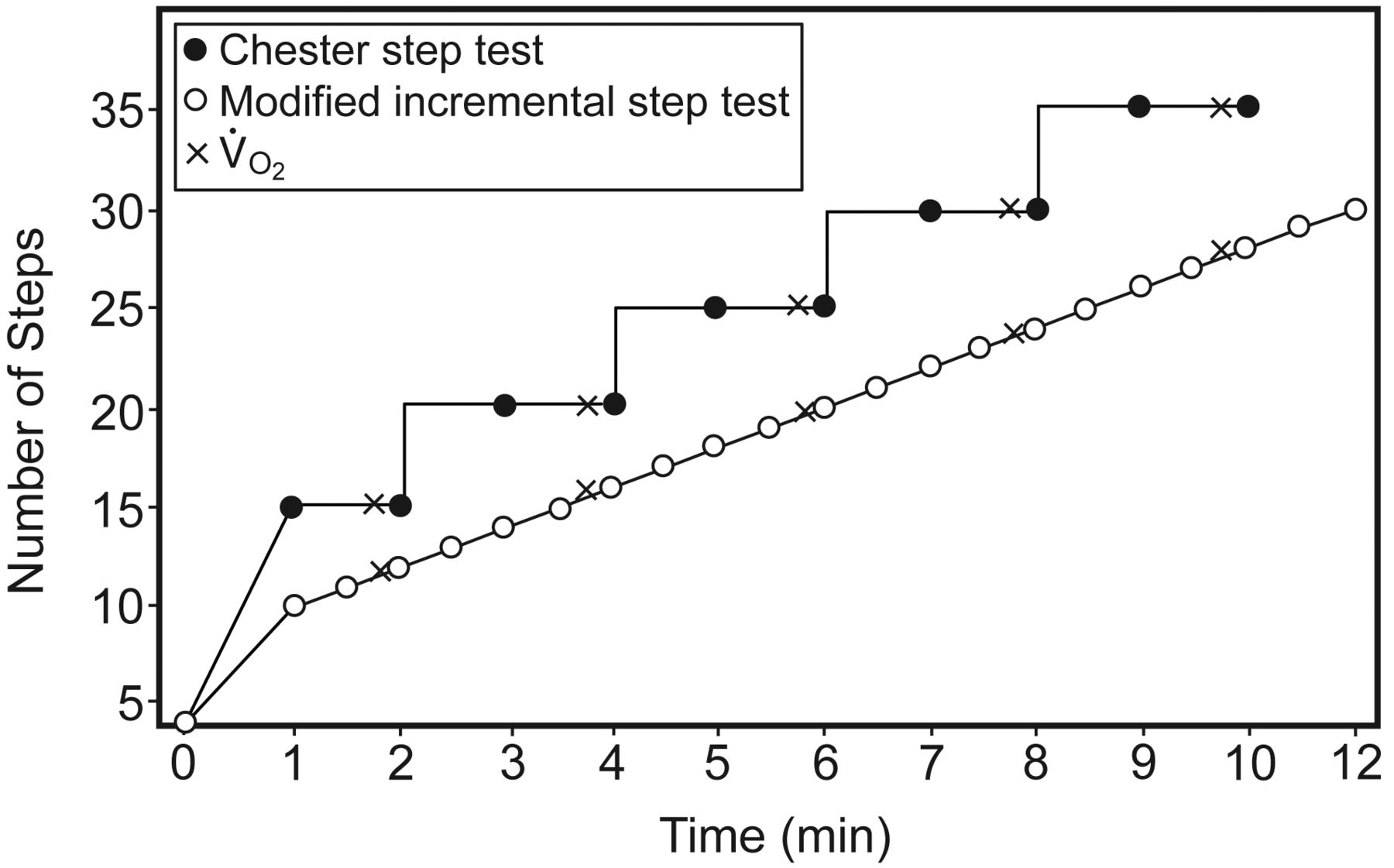
Number of steps versus test time in the Chester step test and the modified incremental step test, with the expected oxygen consumption (V̇O2) for each protocol.
The work was expressed in watts.19
Modified Incremental Step Test
The MIST protocol was modified through a reduction in both the initial step rate and the incremental size throughout the test. We selected an initial step rate of 10 steps per minute because in a previous study on COPD patients,6 subjects completed less than 5 min of the test, despite the constant stepping rate during the step test at 15 steps per minute. The CST also began with 15 steps per minute and had a short duration in this population.10 Additionally, the CST has progressive increments every 2 min, at 5 steps per minute; we assumed that this large increment would be another aspect of the CST responsible for its early disruption in patients with COPD.10 Therefore, we also reduced the work rate increment during the test (ie, 2 steps per minute, with one step distributed every 30 s, see Fig. 1). The stepping rate was determined by an audio signal played on a compact disc. The criteria for stopping the test were the same as described in CST, and the work was also calculated.
Cardiopulmonary Parameters and Perceived Exertion
During step tests, gas exchange parameters, including oxygen uptake (V̇O2), carbon dioxide output (V̇CO2), and minute ventilation (V̇E), were measured by a portable metabolic system (VO2000, Medical Graphics, St Paul, Minnesota). The subject breathed through a face mask. According to the manufacturer's instructions, the system was calibrated before each test by automatic calibration. Heart rate (Polar Precision Performance, Polar Electro, Kempele, Finland) and SpO2 (9500, Nonin, Plymouth, Minnesota) were measured at rest and every minute during the test. Maximum predicted heart rate was calculated (220 –age in years). Change in SpO2 between rest and exercising ≥ 4% was considered desaturation.20 Subjects were asked to rate dyspnea and leg effort at exercise cessation by using the 0–10 Borg category-ratio scale.21
Statistical Analysis
The Shapiro-Wilk test was used to verify the adherence of the data distribution to normality curve. The baseline characteristics and the cardiopulmonary measurements were expressed as mean and SD. Dyspnea and leg fatigue were expressed as median and interquartile range.
Of the total sample (n = 32), the cardiopulmonary responses in the group formed by the same subjects who completed the sixth minute of both tests (n = 6) were compared with the use of 2-way (test and time) repeated measures analysis of variance. Differences at peak exercise between CST and MIST were analyzed with a paired t test. Peak V̇O2, V̇E, heart rate, SpO2, and the total number of steps were also analyzed by the Bland-Altman plots.
The Pearson correlation coefficient (r) was used for association between work performed on CST and MIST with age, FEV1, FVC, V̇E, and SpO2. The Spearman correlation coefficient was used for correlating dyspnea and leg fatigue with work for both tests. The level of significance was set at P < .05. The analyses were performed with statistics software (SPSS 14.0, SPSS, Chicago, Illinois).
The number of steps was the main outcome used to calculate the sample size. We considered a difference of 48 steps between CST and MIST,10,11 with a standard deviation of 6011 and error I and II types of 5% and 20%, respectively. With an assumption of a 20% dropout rate, 30 subjects needed to be recruited.
Results
Most subjects presented with moderate to severe air-flow obstruction (n = 11 and n = 17, respectively), 3 subjects were classified as mild air-flow obstruction, and only one had a very severe obstruction. Table 1 summarizes the baseline characteristics of the studied group.
Baseline Characteristics (n = 32)
All subjects were able to perform both tests on the same day. The frequency of subjects and the number of steps according to the progression of both tests are presented in Table 2. As expected, due to the greater number of steps performed every 2 min in the CST, a higher demand was observed throughout the CST, but with no significant difference at peak exercise between tests (see Table 2). Heart rate achieved > 80% of the maximum of the predicted value for both tests (CST 86 ± 13%, MIST 85 ± 13%). The work was significantly higher for the MIST (229 ± 164 watts) than for the CST (178 ± 138 watts). The magnitude of the fall in SpO2 was equivalent between tests (CST −7 ± 7, MIST −7 ± 6). No difference in Borg scores for dyspnea (CST 4.5 [1–9], MIST 5 [1–9]) and leg fatigue (CST 4 [0–8], MIST 4 [0–8]) was observed at peak exercise. However, when correcting the scores of dyspnea and leg fatigue for the test duration, a higher index was observed for the CST (1.44 [0.67–2.18], 1.09 [0.55–2.08], respectively, P < .001) in relation to the MIST (0.86 [0.51–1.64], 0.75 [0.35–1.24], respectively, P < .001).
Number of Patients, Absolute and Cumulative Step Rates, and Cardiopulmonary Responses During Chester Step Test and Modified Incremental Step Test
A Bland-Altman analysis showed that the mean bias (95% CI) of the peak V̇O2, V̇E, heart rate, and SpO2 differences between the CST and MIST were −0.02 L/min (−0.58 to 0.54 L/min), 0.80 L (−9.24 to 10.84 L), 0.88 beats/min (−9.87 to 11.62 beats/min), and 0.72% (−5.32% to 6.76%), respectively (Fig. 2).
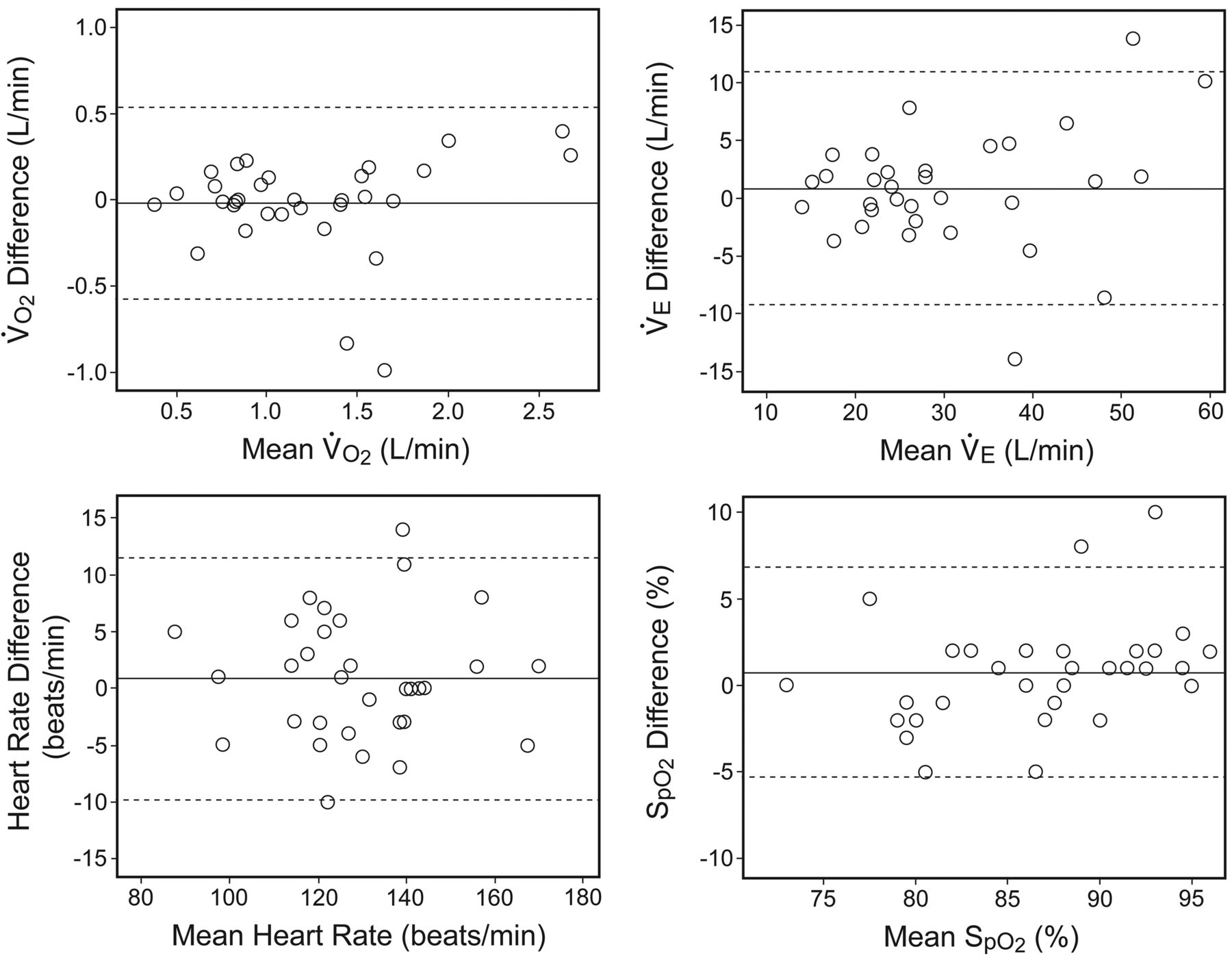
Bland-Altman plots for difference in oxygen uptake (V̇O2), minute ventilation (V̇E), heart rate, and SpO2 at peak exercise.. The dark horizontal lines correspond to the mean differences and the dotted lines to the 95% limits of agreement.
The work performed in the CST and the MIST presented a stronger correlation with peak V̇O2 (r = 0.90, P < .001 for both tests) than with pulmonary function (FEV1 0.60, P < .001 and .58, P < .001; FVC 0.52, P = .002 and .49, P = .005), peak V̇E (r = 0.84 and 0.77, P < .001), and the 6MWT (r = 0.65 and 0.66, P < .001 for both tests). A negative correlation occurred between work and age (r = −0.31, P = .08 and r = −0.40, P = .025), and no correlation was observed for work and desaturation for both tests.
Discussion
The present study has demonstrated that exercise tolerance (exercise time) and performance (number of steps) were higher in the MIST, compared to the CST. Differences in the pattern of increment, which were faster in the CST and slower in the MIST, determined lowest submaximal cardiopulmonary responses during MIST, which were comparable at exercise peak. In addition, the work performed in both tests presented correlation with pulmonary function (FEV1 and FVC), the functional (6MWT), and aerobic capacities (V̇O2).
The MIST and the CST had 3 specific differences: the initial stepping rate, the increment in the stepping rate, and the time period for each increment. Regardless of the lower initial step rate, the slower increment in the stepping rate and the shorter intervals of increment during the MIST determined lower stepping rate at any isotime compared with the CST (see Table 1). This finding explains the longest duration and the lowest cardiopulmonary responses every 2 min of the exercise for MIST (see Table 2). Therefore, our results show that a slower and progressive increment in work rate during step test is better tolerated by subjects with COPD. This assertion is in accordance with previous studies performed on cycle ergometer, which have shown that the larger the increments in work rate, the shorter the exercise duration.12,13 Another explanation for the longer duration in the MIST is that the abrupt and intermittent increment in work load that occurred in the CST may be better perceived by the subject than the continuous increment that occurred in the MIST; therefore, the exercise performance is influenced.16,22
Considering an incremental exercise test, it has been recommended that the incremental phase should last 8–12 min.23 This recommendation is based on tests conducted on healthy subjects14 but may not be applicable to patients with moderate-severe COPD because of exercise intolerance due to inactivity during daily life, peripheral muscle dysfunction, and ventilatory limitation. In addition, it would be expected that step tests have a shorter duration, in comparison with walking tests performed in the corridor, due to increased work resulting from the displacement of body weight against gravity throughout the test.6 Moreover, increased production of lactate and pronounced pulmonary hyperinflation were higher during stair climbing than 6MWT in subjects with severe COPD.24 In the present study, the CST and MIST had a shorter duration than that recommended by the American Thoracic Society/American College of Chest Physicians.23 However, MIST had, on average, a similar duration (≈ 6 min) to other field tests such as the 6MWT and shuttle walk test, which have been commonly used to assess exercise intolerance in patients with COPD. This finding may be attributed to the adaptation of MIST from the CST in which the initial rhythm and the increments in work (number of steps/min) were reduced. Therefore, the test could be tolerated by subjects severely impaired and also would not exceed a testing time over 12 min in mild subjects.
Although the tests have different adjustment in the work rate increment, both tests showed similar cardiopulmonary responses at peak exercise. These findings are in line with previous studies performed on cycle ergometer in subjects with COPD and pulmonary hypertension, which have demonstrated that variations in work rate determine equivalent peak values for V̇O2,12,13,15,16 V̇E,12,13,15,16 heart rate,12,13,15,16 and SpO2.13,15,16 Field tests also result in similar values of V̇O2,25 heart rate,25,26 and dyspnea26 at peak exercise, compared to incremental cycle ergometer test. Future studies comparing the responses at peak exercise between the MIST and cycle ergometer are needed to confirm whether this test leads to a maximum cardiopulmonary response. In relation to cardiac stress, CST and MIST determined a heart rate at peak exercise, on average, corresponding to 85% of predicted maximum heart rate. Similar results were observed when other field tests, 6MWT25,26 and shuttle walk test,26 were compared to maximal cardiopulmonary exercise testing. The work performed on CST and MIST showed similar correlation coefficients for variables of pulmonary function and exercise capacity. The negative correlation observed between work and age was expected due to structural and functional decline with aging. The strength of association between work in both tests and lung function was close to that described for 6MWD and shuttle walk test with FEV1.27–29 FEV1 is a traditional index used to classify the severity of COPD. Although it does not express the changes in lung volumes during exercise, it is still a reasonable marker of the mechanical changes by which COPD reduces exercise tolerance. Furthermore, FEV1 is a predictor of the maximum ventilation reached in exercise.30 Therefore, low values of FEV1 lead to reduced ventilatory capacity and consequently reduced exercise capacity. This finding explains the correlation between work and V̇E at peak of exercise found in our data, which agrees with a prior study with the distance covered in the shuttle walk test and peak ventilation.27 In addition, the correlation observed between work (as obtained from the CST and the MIST) and the distance walked on the 6MWT was very close to that observed between the distances covered on the shuttle walk test and the 6MWT.31
The adaptation of the CST in MIST resulted in a longer test, which presents a duration comparable to the other field tests. Therefore, the MIST can be an option when long corridors are not available for the 6MWT and shuttle walk test. Moreover, step training has been used as part of aerobic training in pulmonary rehabilitation programs, but the protocols for training are not standardized.32–36 Usually, aerobic training is based on a percentage of the maximum load reached in a maximum test. Thus, the step training should be done in the same way. In this context, we have suggested that, first, the subject undergo MIST to establish the peak work load, which is represented by the total number of steps, and then a percentage of it would be performed during the training session. High-intensity aerobic training has been recommended for patients with COPD.37 As the MIST resulted in a greater total number of steps, a greater absolute work load would be determined when using a percentage between 60–80% of the total number of steps. However, the effectiveness of this proposal should be tested in future studies. As in cycle ergometer tests, in which increment from 5 to 30 watts/min can be chosen based on the baseline physical capacity, we have speculated that the same should be done for step test with incremental pattern. From this point of view, depending on the major or minor exercise capacity, the step test should start with higher/lower rate and increments. Thus, we suggest for more severe patients that the MIST start with a lower rate than tested in this study and that larger increment be tested in mild COPD. In addition, studies analyzing the training step based on MIST should be conducted.
Study Limitations
The reproducibility of MIST was not tested, but in a pilot study of our group the MIST was highly reproducible.11 However, the main limitation to consider is the so-called ceiling effect. The maximum number of steps that a subject is able to perform per minute can be achieved without the subject interrupting the test by dyspnea and/or fatigue. However, the ceiling effect can be also observed in the 6MWT and shuttle test. Compared to the CST, the MIST seems to slow the ceiling effect because it starts with a slower pace and has smoother increments. For example, on average, our subjects performed 4 min of the CST, which corresponds to a rate of 20 steps per minute. For subjects to achieve this same number of steps during MIST requires 6 min of testing. Moreover, it is interesting to point out that none of our subjects reached the last stage of the CST, which has a pace of 35 steps per minute, which would only be achieved in MIST between 13 and 14 min of testing, the upper limit recommended by the American Thoracic Society/American College of Chest Physicians.23
Conclusions
In conclusion, our data show that metabolic, cardiovascular, and respiratory responses during both CST and MIST were similar at peak exercise, but differences in increment size determine a longer duration and higher total number of steps during MIST.
Footnotes
- Correspondence: Simone Dal Corso PT PhD, Rehabilitation Science Master's Program, Universidade Nove de Julho, Avenida Francisco Matarazzo, 612 - 1° Andar, Bairro Água Branca, São Paulo, 05001–100 Brazil. E-mail: simonedc{at}uninove.br.
Supported by a research grant from São Paulo Research Foundation (FAPESP 20120/09732-6).
Dr de Camargo was supported by Programa de Suporte à Pós-Graduação de Instituições de Ensino Particulares/Coordenação de Aperfeiçoamento de Pessoal de Nível Superior, Brazil Ministry of Education.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}