

Abstract
BACKGROUND: The aim of this retrospective long-term follow-up study was to assess 5-year outcomes after combined uvulopalatopharyngoplasty (UPPP) and midline glossectomy surgery for the treatment of obstructive sleep apnea-hypopnea syndrome (OSAHS).
METHODS: A total of 34 subjects with OSAHS with combinatory obstructions of posterior soft palate and posterior tongue area who underwent combined midline glossectomy and UPPP were successfully followed for 5 years to examine the therapeutic effect of treatment. All subjects were of Friedman stage II or III and had major stenoses at the base of the tongue. The apnea-hypopnea index (AHI), and mean lowest SpO2 were measured preoperatively and postoperatively to assess therapeutic efficacy.
RESULTS: The mean preoperative AHI was 56.0 ± 8.4 episodes/h, while the mean lowest SpO2 was 62.1 ± 10.6%. AHI and mean lowest SpO2 were significantly increased and decreased, respectively, from preoperative levels at each follow-up point after surgery, up to 5 years (P < .05). The average widened pharyngeal space after surgery was 42 mm2. At 6 months, surgery was classified as being curative in 27/34 (79.41%) of subjects, and markedly effective or effective in the remaining subjects. At 5 years, surgery was classified as being curative in 7/34 (20.59%) subjects, markedly effective or effective in 25/34 (73.53%) subjects, and not effective in 2/34 (5.88%) subjects. Five years after surgery the average body mass index for the subjects who were not cured was slightly higher than those who were cured, but the difference was not statistically significant (31.3 ± 3.7 kg/m2 vs 29.7 ± 3.6 kg/m2, P = .29). Subjects who were cured had lower supine AHI values than those who were not cured (2-year postoperative AHI 36.8 ± 9.2 episodes/h vs 43.8 ± 6.9 episodes/h, P = .03, 5-year post-operation AHI 32.1 ± 7.6 episodes/h vs 41.7 ± 8.2 episodes/h, P = .006).
CONCLUSIONS: These findings suggest that combined midline glossectomy and UPPP can be an effective treatment for subjects with Friedman stage II or III OSAHS and substantial stenosis around the base of the tongue.
Introduction
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a common disorder characterized by obstruction of the upper airway due to collapse or narrowing. Findings from a survey conducted in the United States in 2005 suggested that approximately 25% of adults had a high risk of OSA.1 This is problematic, since OSA is associated with depression, decreased quality of life, an increased risk of motor vehicle accidents, and cardiovascular complications.2–4 Of further concern, given the current obesity epidemic in many parts of the world and the strong link between obesity and OSA,5 is the likelihood that an increasing number of individuals will require treatment for OSAHS in the coming years.
Treatment for OSA depends on the underlying pathology, but may include lifestyle modifications (weight loss, avoidance of alcohol, sleeping position), intraoral devices, positive airway pressure ventilation, and various types of surgery.6,7 Surgery is typically reserved for cases (generally moderate to severe) where other less invasive options have failed. One surgical approach commonly used for the treatment of OSAHS is uvulopalatopharyngoplasty (UPPP).8 Unfortunately, UPPP does not appear to be effective in up to 50% of cases.7–9 Another surgical approach is midline laser glossectomy, the aim of which is to reduce the size of the tongue and thus enlarge the hypopharyngeal airway.10 To date, there have been relatively few reports published describing results for subjects with OSAHS following UPPP and midline glossectomy. Furthermore, the studies published have included a small numbers of subjects (< 23).10–13 Quite clearly, additional studies are needed to clarify whether the combination of UPPP and midline glossectomy is an effective treatment for OSAHS.
The aim of this study was to determine the 5-year therapeutic effect of midline glossectomy with combined UPPP in a relatively large cohort of subjects with OSAHS. The surgical approach used, complications, and outcomes are provided.
QUICK LOOK
Current knowledge
Obstructive sleep apnea-hypopnea syndrome (OSAHS) is a common disorder characterized by obstruction of the upper airway due to collapse or narrowing. Treatment for OSAHS depends on the underlying pathology, but may include lifestyle modifications, intraoral devices, positive airway pressure ventilation, and surgery. Midline laser glossectomy, to reduce the size of the tongue and enlarge the hypopharyngeal airway, can be combined with uvulopalatopharyngoplasty (UPPP) in severe cases.
What this paper contributes to our knowledge
Combined midline glossectomy and UPPP is associated with a high 6-month cure rate in patients with severe OSAHS. The cure rate decreases with time but remains effective in over 90% of cases after 5 years. Longer-term (> 5 years) effectiveness remains to be confirmed.
Methods
Subjects
In this retrospective cohort study, the outcomes of subjects with severe OSAHS and combinatory obstructions of posterior soft palate and posterior tongue area who underwent midline glossectomy and UPPP at the Second Affiliated Hospital of Xi'an Jiaotong University were followed from January 2003 to August 2005. OSAHS was diagnosed by polysomnography (PSG), with reference to the 2009 Chinese Diagnosis and Surgical Treatment Guidelines for OSAHS.14 A PSG sensor using the Australian Condi detector was used to assess: apnea-respiratory arrest > 20 s, accompanied by heart rate (< 100 beats/min), and (or) cyanosis, hypotonia, etc; hypopnea, hypoventilation-respiratory air flow reduced by > 50%, and with a > 4% reduction of oxyhemoglobin saturation. Respiratory effort related arousals were not included.
All the (consecutive) subjects treated during this period were classified as either Friedman stage II or III; there were no stage I subjects.15 Preoperative routine physical examination revealed hypertrophy of the soft palate, uvula, corpora allata, and tongue in all subjects. Hypertrophy of the soft palate was confirmed by 3-dimensional computed tomography (CT). The dorsum of the tongue was consistently elevated and the pharyngo-oral cavity was narrowed (Fig. 1). The CPAP device was offered to all subjects, but they did not tolerate CPAP and subsequently chose surgery. Only subjects who were followed up for ≥ 5 years were included in the study. Patients with thyroid or pituitary dysfunction were excluded.
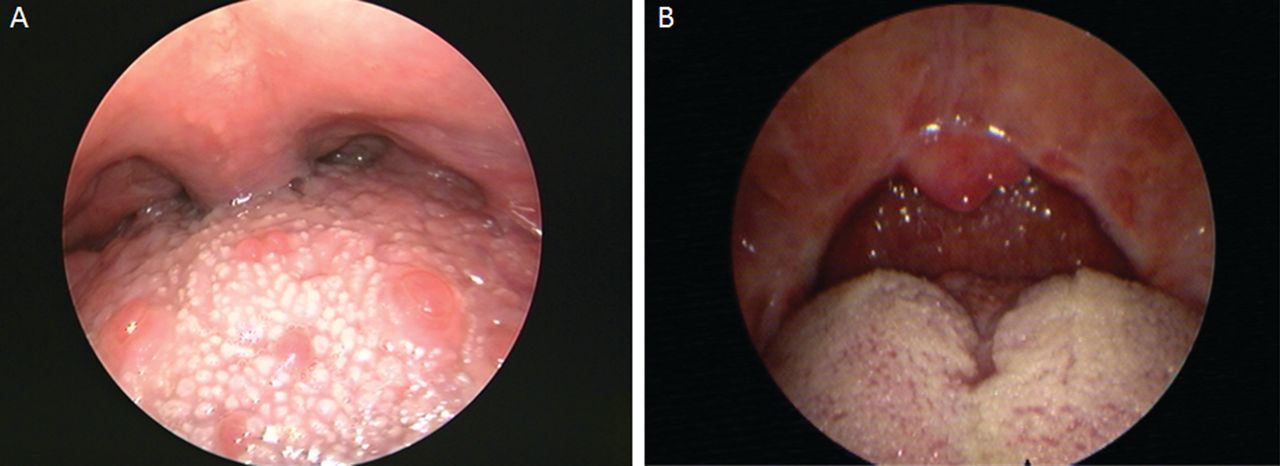
The same subject with severe obstructive sleep apnea-hypopnea syndrome before and after combined midline glossectomy and uvulopalatopharyngoplasty. A: Before the operation there was apparent hypertrophy in the base of tongue, causing oropharyngeal stenosis. The uvula is not visible without pressing down the tongue. B: Two years post-operation the base of the tongue forms a groove with an enlarged oropharyngeal airway.
This study was approved by the ethics committee of the Second Affiliated Hospital of Xi'an Jiaotong University.
Surgery
All subjects received CPAP treatment and blood pressure and blood glucose normalizing medications (where necessary) 5–7 days before surgery. No subjects were refused surgery based on their age or body mass index (BMI).
Uvulopalatopharyngoplasty
Subjects were anesthetized, tracheally intubated, and placed in a supine position. Tonsils were removed first using a conventional stripping method. The palatine velar cleft was dissected and the adipose tissue in the soft palate area was resected. The adipose tissue of the uvula was removed and the mucosa sutured; thus, the uvula was smaller.
Posterior Midline Glossectomy
The dorsum of the tongue was lowered to expand the oropharyngeal cavity. From a point 2 cm from the tip of the tongue to the epiglottis, the tongue surface and 1 cm deep muscles were gradually resected toward the base of the tongue. The anterior and posterior tissue at the base of the tongue close to the epiglottis was sutured. The resected spindle-shaped tongue tissue was approximately 4–5 cm long, 1–1.5 cm wide, and 1 cm thick. All surgical procedures were performed by 3 experienced surgeons.
Postoperative Care
Routine postoperative treatments included antibiotics, dicynone (3,000 mg/d for the first 3 d), cabenzamine (300 mg/d for the first 3 d), and dexamethasone (for subjects without hypertension, diabetes, or gastric ulcer: 10 mg/d for the first 3 d, and 5 mg/d for the ensuing 3 d). Subjects were encouraged to consume a liquid diet 2 days after surgery and a semi-liquid diet 4 days after surgery. All sutures at the base of the tongue were removed by the ninth day after surgery. Subjects were discharged after suture removal and were able to resume a normal diet 2 weeks after surgery. For those subjects who elected not to return for their postoperative visits, subject follow-up was conducted by telephone interview.
Measures
Clinical characteristics recorded included blood pressure, comorbidities (hypertension, diabetes), fasting plasma glucose concentration, lipid profile, Friedman classification,15 and daytime sleepiness (using the Chinese modified version of the Epworth Sleepiness Scale [ESS]; see the supplementary materials at http://www.rcjournal.com).16 Specific criteria for the ESS were as follows: subject's lethargy frequency (would never doze = 0, slight chance of dozing = 1, moderate chance of dozing = 2, high chance of dozing = 3). The situations used to determine sleepiness: sitting and reading; watching TV; sitting, inactive in a public place; as a passenger in a car for 1 hour; an environment that allows lying down to rest in the afternoon; sitting and talking to someone; not drinking alcohol after lunch and sitting quietly; in a car stopped for a few minutes in traffic. The numbers selected for the 8 situations in the ESS were added together to give a score for each subject (total between 0 and 24). These ESS scores were capable of distinguishing individuals and diagnostic groups over the entire range of daytime sleepiness. ESS scores from 6 to 11 points suggested mild drowsiness (daytime sleepiness); scores from 11 to 16 points suggested moderate drowsiness (daytime sleepiness); scores > 16 points indicated a high degree of (or severe) sleepiness. Subjects with BMI > 30 kg/m2 were considered to be obese, while those with BMI of 25–30 kg/m2 were considered to be overweight.
Preoperative laryngopharyngeal 3-dimensional CT was performed to assess stenosis of the posterior palate and tongue while subjects were asleep.17 The cross-section with the smallest area was defined as the main stenosis plane. PSG was performed to assess the response 1 week before surgery, and 6 months, 1 year, 2 years, and 5 years after surgery. Six months after surgery, pharynx 3-dimensional reconstruction CT scans were performed. The apnea-hypopnea index (AHI = episodes of apnea/h + episodes hypopnea/h), and mean lowest SpO2 were recorded. The criteria for assessing the therapeutic effect of treatment were as follows: AHI < 5 episodes/h = cure; AHI < 20 episodes/h and decrease of ≥ 50% = markedly effective; AHI decrease ≥ 50% = effective; AHI decrease < 50% = not effective. Postoperative complications were also recorded.
Statistical Analysis
Subject demographic, clinical characteristics, and treatment outcomes were summarized as mean ± SD for continuous variables and n (%) for categorical ones. The AHI and mean lowest SpO2 data are presented as a bar chart as for mean ± SD over time. The distributions of mean lowest SpO2 between time points were compared using the paired t test, whereas AHI was performed using the Mann-Whitney U test, due to the fact that the data were not normally distributed. The association of cure rate with subject daytime sleepiness level, hypertension, diabetes mellitus, BMI, and AHI were performed using the Fisher exact test in categorical data and the 2-sample t test in continuous data, respectively. All statistical assessments were considered significant if P < .05. Furthermore, P value < .01 (= 0.05/5) was also considered to indicate statistical significance for the multiple comparisons. Statistical analyses were performed using statistical software (SPSS 15.0, SPSS, Chicago, Illinois).
Results
Demographics and Clinical Characteristics
A total of 58 subjects with severe OSAHS underwent midline glossectomy and UPPP. Of these subjects, 34 were followed up for ≥ 5 years and included in the study (Table 1). All of the subjects were male, ranging in age from 26 to 57 years. Most (25/34, 73.5%) subjects suffered severe daytime sleepiness (based on the ESS scores). All subjects were overweight or obese (BMI > 24 kg/m2) and classified as either Friedman stage II or III. Approximately 25% of subjects had coexisting hypertension. For > 75% of the subjects, the main stenosis plane was located in the posterior palate and tongue. The mean total time spent below 88% O2 saturation was approximately 180 s.
Summary of Demographic and Clinical Characteristics (n = 34)
All 24 subjects lost to follow-up thought they were feeling better without important daytime sleepiness. Therefore, none of these subjects elected to return to the hospital for PSG monitoring and ESS score evaluations. Therefore, follow-up for these subjects was conducted by telephone interview.
Postoperative Complications
Two subjects experienced perioperative tongue swelling. These subjects were transferred to the ICU and extubated the day after surgery. After extubation, 3 subjects experienced a decreased SpO2 due to glossocoma. All 3 subjects recovered after insertion of an oropharyngeal catheter, which was removed the following day, once respiration had been stabilized. The suture at the base of the tongue detached 7 days after surgery in 3 subjects, and wound dehiscence at the base of the tongue occurred. However, no active bleeding was detected. These subjects recovered with conservative treatment. No long-term complications or side effects have been found during 5-year follow-up for any of the subjects. In addition, there were no adverse effects on subjects' quality life.
Apnea-Hypopnea Index and Mean Lowest SpO2
The mean preoperative AHI was 56.0 ± 8.4 episodes/h, while the mean lowest SpO2 was 62.1 ± 10.6%. AHI and mean lowest SpO2 were significantly increased and decreased, respectively, from preoperative levels at every follow-up time point after surgery (P < .05: Figs. 2 and 3).

Apnea-hypopnea index scores in subjects (n = 34) with obstructive sleep apnea-hypopnea syndrome before and after combined midline glossectomy and uvulopalatopharyngoplasty. The difference was significant at each postoperative time point.
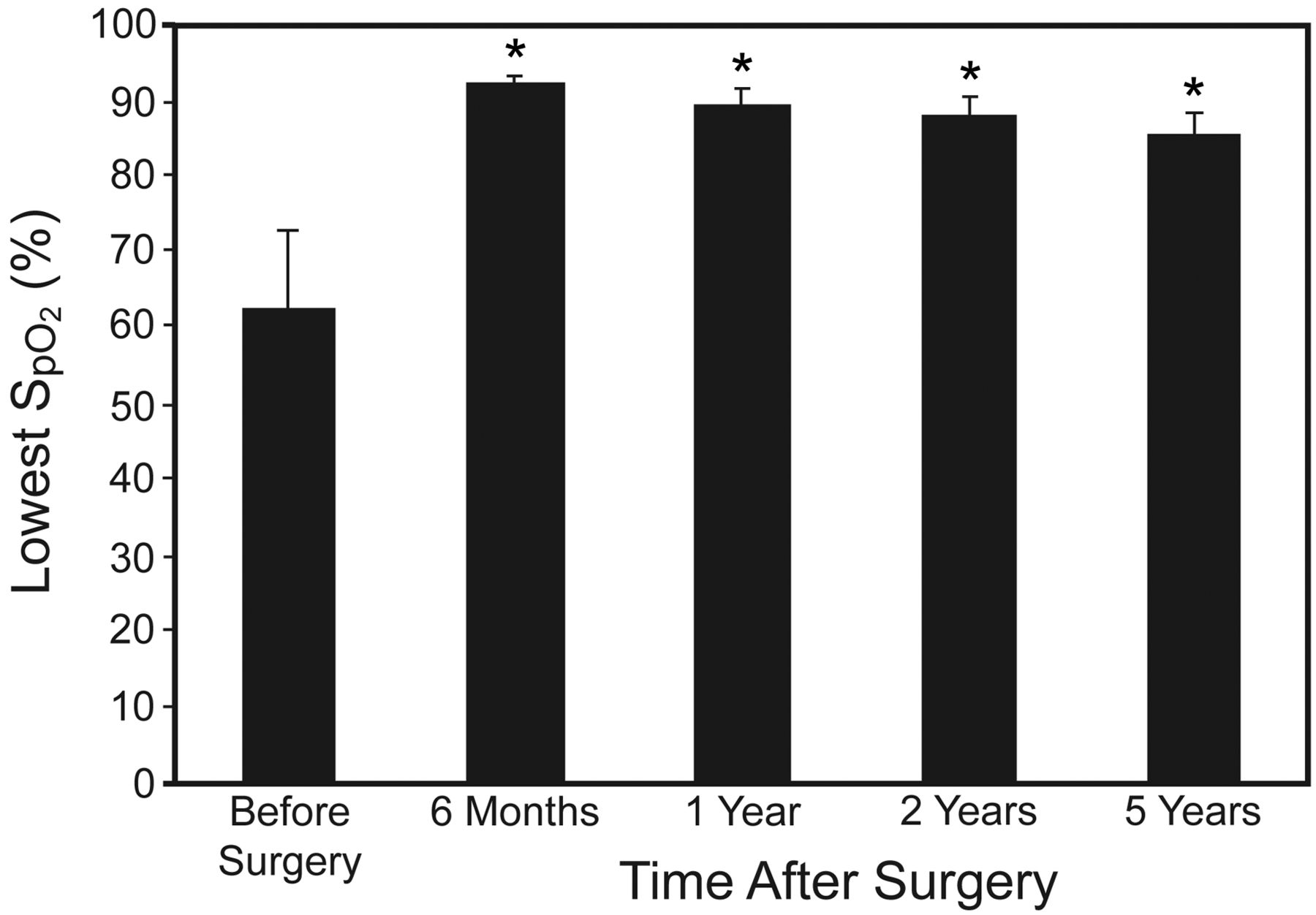
Mean lowest SpO2 in subjects (n = 34) with obstructive sleep apnea-hypopnea syndrome before and after combined midline glossectomy and uvulopalatopharyngoplasty. The difference was significant at each postoperative time point.
Clinical Outcomes
The mean widened pharyngeal space after surgery was 42 mm2. Six months after surgery, the majority (27/34, 79.41%) of subjects were classified as being cured, while surgery was classified as being markedly effective or effective in the remaining subjects (Table 2). Thereafter, the percentage of subjects classified as being cured gradually decreased, such that by 5 years after surgery, slightly over 20% of subjects were classified as cured. At 5 years follow-up, surgery was classified as being markedly effective or effective in the majority (25/34, 73.53%) of subjects. At 5 years follow-up, surgery was classified as being not effective in 2 of 34 (5.88%) subjects. The mean pharyngeal space after surgery was 42 mm2 as determined by CT. Figures 4 and 5 are examples of representative CT photographs before and after surgery.
Summary of Treatment Outcomes After Combined Midline Glossectomy and Uvulopalatopharyngoplasty in Patients With Obstructive Sleep Apnea-Hypopnea Syndrome (n = 34)

Representative computed tomography photograph before surgery, showing a pharyngeal space of 17.6 mm2.
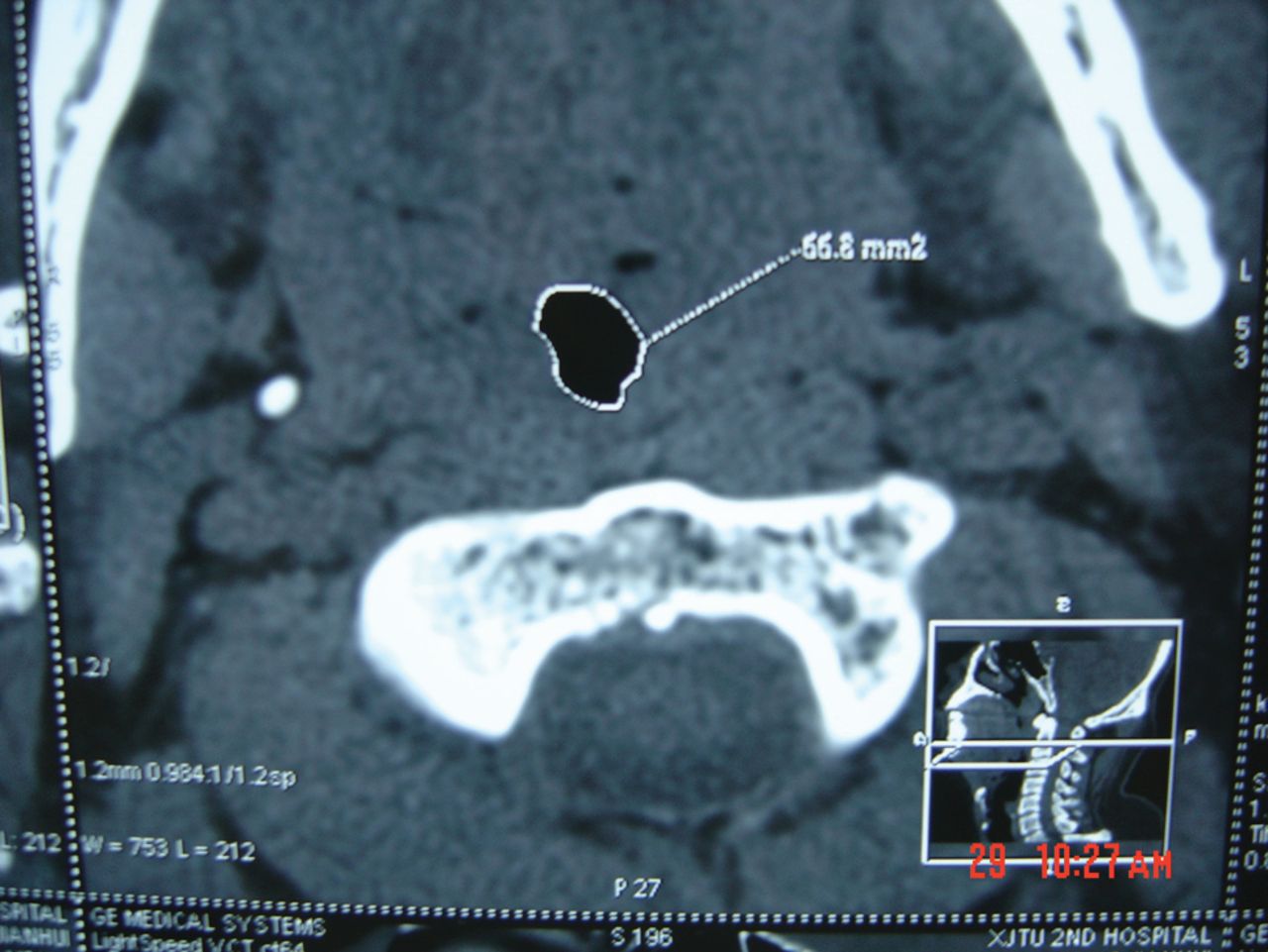
Representative computed tomography photograph after surgery, showing a pharyngeal space of 66.8 mm2.
The daytime sleepiness level of the subjects was not associated with their medical history with respect to hypertension and diabetes mellitus (data not shown). However, their sleepiness level was associated with supine AHI. The average BMI for the subjects who were not cured was slightly higher than those who were cured at 5 years after surgery, but the difference was not statistically significant (31.3 ± 3.7 kg/m2 vs 29.7 ± 3.6 kg/m2, P = .29). Subjects who were cured had lower supine AHI values than those who were not cured (2 years postoperative 36.8 ± 9.2 episodes/h vs 43.8 ± 6.9 episodes/h, P = .03, 5 years postoperative 32.1 ± 7.6 episodes/h vs 41.7 ± 8.2 episodes/h, P = .006). In the non-supine AHI there was no significant difference observed between cured and non-cured subjects.
Discussion
In the present report, the outcomes following combined midline glossectomy and UPPP in subjects with severe OSAHS (Friedman stage II or III with substantial stenosis around the tongue base) have been summarized. To our knowledge, this trial included the largest number of subjects in a study of this nature to date. Subject CT photographs demonstrated that the surgical procedure was effective in expanding the pharyngeal space. The majority (approximately 80%) of subjects were classified as cured 6 months after surgery. Although the percentage of subjects classified as being cured decreased substantially with time (the 5 year cure rate was approximately 20%), therapy was considered to be effective in the majority of subjects (32/34, 94.1%) 5 years after surgery. The daytime sleepiness level of the subjects appeared to be unrelated to hypertension or diabetes mellitus. However, their level of sleepiness did appear to be associated with supine AHI (2 and 5 years post-operation).
The cure rate (indicated by AHI < 5 episodes/h) in this study was 79.41% 6 months after combined midline glossectomy and UPPP. The corresponding cure rate 5 years after surgery was 20.59%. Previous studies examining the effects of glossectomy and UPPP in subjects with OSAHS assessed outcomes using various criteria. Fujita et al10 and Elasfour et al12 reported that 42% and 61% of subjects, respectively, responded to treatment as indicated by AHI decreases ≥ 50% within 2 years after surgery. Using different criteria, Mickelson and Rosenthal11 found that 25% of subjects responded to treatment, as indicated by a respiratory disturbance index < 20 episodes/h, 74 days, on average, after surgery. In another study, Andsberg and Jessen13 reported that the apnea index was reduced by 50% in 59% of subjects and normalized in 32% of subjects 1 year after surgery. These researchers further reported that the apnea index was normalized in 25% of subjects an average of 8.4 years after surgery.13 These longer-term findings are broadly consistent with the results of the current study; however, it is difficult to compare findings between this and other studies, given the different criteria used and the variable lengths of follow-up.
There have been a number of other reports describing combined UPPP with other therapies for treating OSAHS. For instance, Friedman et al18 examined the effectiveness of combined UPPP and radiofrequency tongue base reduction, and found that 51.1% of patients with stage II OSAHS and 33.0% of patients with stage III OSAHA were cured 6 months after surgery. These rates of cure are well below the mean rate of cure in our study. In a similar study, van den Broek et al19 found that 49% of patients with mild to severe OSAHS were cured after combined UPPP and radiofrequency thermotherapy of the tongue base. Unfortunately, the timing of postsurgical assessment was not stated in this report; hence, it is difficult to compare the findings with our own. In another study, Omur et al20 reported that 81.8% of patients with severe OSAHS who underwent combined UPPP and tongue base suspension were cured at an average of 14 months after surgery. This cure rate (the definition is the same as “markedly effective” in the current study) was similar to this study.
We found that several clinical symptoms recurred with time after surgery in some subjects. Polysomnographic monitoring revealed that AHI gradually increased and that nighttime mean lowest SpO2 gradually decreased. There are several potential explanations for these changes. First, scar tissue compliance may have gradually increased, while pharyngeal soft tissue tension may have decreased. Furthermore, subjects may have failed to control their weight, leading to re-accumulation of fat tissue beneath the pharyngeal mucosa and recurrence (to varying degrees) of pharyngeal stenosis with possible soft tissue collapse. Nevertheless, this surgical approach involves resecting a substantial amount of muscular tissue beneath the pharyngeal mucosa and tissue at the base of the tongue, such that postoperative recurrence of hypertrophy is unlikely to cause OSAHS symptoms as severe as those before surgery. The finding of the current study that surgery was ineffective in only 2 out of 34 subjects 5 years after surgery supports this assertion. Further study is needed to elucidate the precise mechanism(s) underlying the recurrence of clinical symptoms after surgery.
The current study has several limitations that must be acknowledged. First, the study did not include a control group and involved only male subjects. However, not treating a sub-cohort of subjects to control for the treated subjects would have been unethical. Certainly, direct comparisons of outcomes between combined midline glossectomy and UPPP and other surgical treatments (ie, UPPP alone) are needed to further examine the efficacy of this approach. The inclusion of only male subjects reflects the fact that OSAHS is a predominately a condition found in males. Second, subject-rated symptom improvement was not quantitatively assessed. However, most subjects reported that their symptoms were improved after surgery, corresponding with a widened pharyngeal space (mean of 42 mm2), as determined by CT. In the future, we plan to perform preoperative and postoperative assessments to determine subject-rated symptom improvement. Hypertension and diabetes were not monitored after surgery. Therefore, treatment effect and cure in this study were based solely on PSG criteria. A final limitation is that a high percentage of subjects (24/58, 41%) were not followed up for 5 years. The majority of these subjects felt that their symptoms had improved and therefore declined to return for follow-up examinations.
Conclusions
In summary, the study results suggest that combined midline glossectomy and UPPP is associated with a very high 6-month cure rate in subjects with severe OSAHS (Friedman stage II or III with substantial stenosis around the tongue base). Although this cure rate decreased with time, surgery was curative, markedly effective, or effective in 94% (32/34) of subjects 5 years after surgery. The longer-term (> 5 years) effectiveness of this treatment remains to be confirmed.
Footnotes
- Correspondence: Quanqing Kang MD, Department of Otolaryngology, Head and Neck Surgery, Second Affiliated Hospital, Xi'an Jiaotong University School of Medicine, Xi'an, PR China, 710004. E-mail: KangQuanqing123{at}163.com.
The authors have disclosed no conflicts of interest.
Supplementary material related to this paper is available at http://www.rcjournal.com.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}