

Abstract
BACKGROUND: In adults it is recommended that the minimum of 10,000 steps/day should be performed in order to consider an individual as active. The pedometer, a small device that counts steps, has been used to monitor and/or motivate physical activity in various populations.
OBJECTIVE: To investigate the short-term effects of a protocol using a pedometer or an informative booklet to increase daily physical activity in apparently healthy smokers who reached or did not reach the minimum public health recommendation of 10,000 steps/day.
METHODS: Subjects were randomly assigned to 2 groups: group pedometer (GP, n = 23), who wore a pedometer every day during 1 month, aiming to achieve 10,000 steps/day; and group booklet (GB, n = 17), who received a booklet with encouragement to walk as much as possible in everyday life. Each group was subdivided according to their baseline daily physical activity level: active (subjects who achieved 10,000 steps/day), and inactive (those who did not achieve this minimum).
RESULTS: Only the physically inactive GP increased significantly its daily physical activity (pre vs post 7,670 [6,159–9,402] steps/day vs 10,310 [9,483–11,110] steps/day, P < .001), with a concomitant increase in the 6-min walking test (6MWT) distance (mean and interquartile range 540 m [501–586 m] vs 566 m [525–604 m], P = .03). In GP, Δ post-pre steps/day correlated significantly with baseline number of steps/day (r = −0.63, P = .01), but not with 6MWT. In the inactive subjects (summing GP and GB), there were significant correlations between steps/day and cigarettes/day, pack-years, and Fagerström questionnaire (r = −0.55, −0.40, and −0.59, P ≤ .05 for all). Furthermore, improvement in steps/day in the inactive subjects of GP was correlated with baseline cigarettes smoked per day, pack-years, and Fagerström questionnaire (r = 0.51, 0.65 and 0.53, P ≤ .05 for all).
CONCLUSIONS: Physically inactive smokers improve their daily physical activity level by using a simple tool (pedometer), and larger improvement occurs in subjects with the lowest levels of physical activity.
Introduction
Smoking is the cause of high rates of morbidity and mortality worldwide, and is considered the leading cause of preventable death by the World Health Organization.1 Associated with smoking, physical inactivity also has an important role in the development of high morbidity and mortality rates. The concept that regular physical activity can prevent or delay the onset of various chronic diseases has solid scientific support.2 Therefore, the combination of physical inactivity and smoking generates deleterious health effects. This was well illustrated by Garcia-Aymerich et al,3 who showed that regular physical activity in smokers is associated with less pronounced decline in lung function over time, and consequently a lower risk for development of COPD.
Recently, reduction of physical activity in daily life, as well as the factors that influence this reduction, has been the object of study in several populations.4–8 In adults it is recommended that at least 30 min of daily moderate physical activity is necessary to maintain physical fitness,2 or that a minimum of 10,000 steps/day should be achieved to consider an individual as physically active.9 Since quantification is imperative, the use of motion sensors has been recommended in order to obtain an accurate assessment of daily physical activity. Motion sensors are instruments used to detect body movement and consequently quantify physical activity in daily life for a period of time in an objective manner.10 Among these instruments, pedometers stand out; they are simple, small, low cost, and easily applicable devices that count an individual's steps in a given period of time.11 Pedometers have been used not only to monitor the individual's number of steps in daily life,12 but also as a motivational tool for increasing physical activity of several populations.13–17
In recent years the scientific literature showed some studies concerning promotion of regular physical activity in smokers.18,19 The study by Green et al18 concluded that social initiatives can be successfully applied to increase physical activity, along with reduction of tobacco use. Prochaska et al,19 in a randomized controlled trial, concluded that physical activity promotion in addition to a smoking cessation program was associated with increased daily physical activity levels and to persistence of smoking abstinence in individuals who stopped smoking. However, in smokers there are still no studies that have compared changes in daily physical activity levels obtained by different motivational interventions, such as encouragement to increase the number of steps/day using pedometers and informative booklets.
Furthermore, it is unclear whether physically inactive smokers have more substantial increases in daily physical activity after intervention, in comparison to already physically active smokers. Therefore, the purpose of this study was to analyze the effects of a motivational protocol to increase daily physical activity using pedometers or informative booklets in smokers, achieving or not the minimum recommendation of 10,000 steps/day. Secondarily, it aimed to study the relationship between changes in daily physical activity and changes in exercise capacity, nicotine dependence, and smoking habits after the intervention.
QUICK LOOK
Current knowledge
A pedometer can be used to monitor and motivate physical activity in patients with cardiorespiratory disease. An active subject is defined as someone achieving a minimum of 10,000 steps per day.
What this paper contributes to our knowledge
Physically inactive smokers may improve their daily physical activity level by using a pedometer. Subjects with the lowest level of physical activity may have the largest improvement with use of the pedometer.
Methods
Recruitment, Study Design, and Subjects
Seventy-six smokers were recruited by the current researchers, through advertisements in the media, buses, and health centers. The announcement invited asymptomatic or mildly symptomatic smokers, over 18 years old and of both sexes, to participate in a program of physical activity promotion.
Inclusion criteria were: current smokers (regardless of duration of smoking) over 18 years old, of both sexes, normal spirometry (ie, without spirometric alterations), and absence of pathological conditions that could influence the performance of physical activities in daily life (eg, cerebrovascular, rheumatic, or orthopedic disease). Exclusion criteria were: inability to understand or cooperate with the application of questionnaires and other tests, and failure to attend the final evaluation. The study was approved by our Ethics Committee in Research, and data were collected from June 2008 to April 2010 at our research laboratory. All subjects gave formal consent to participate in the study by signing an informed consent term prior to their inclusion.
In a longitudinal design, the included smokers were submitted to a series of assessments immediately before and immediately after the completion of a 1-month protocol that aimed to increase their daily physical activity by using pedometers or informative booklets. Both before and after the protocol, the tests included lung function (spirometry), functional exercise capacity (6-min walking test [6MWT]), nicotine dependence, and smoking habits, besides the quantification of daily physical activity with a pedometer (steps/day). The methodology involved in the tests is described in more detail below.
After the initial assessment, subjects were randomly divided through blocks of 10 opaque concealed envelopes into 2 groups: group pedometer (GP, n = 39) and group booklet (GB, n = 37). Allocation and random sequence were generated by a researcher not involved in the present study, whereas assignment to the interventions was done by the current researchers. GP subjects were instructed to use a pedometer daily for a 1-month period in order to achieve the minimum of 10,000 steps/day as a target. Subjects were also instructed to record the number of daily steps achieved by the end of each day, as well as any information they judged necessary about their daily physical activity. The accuracy of all pedometers was tested prior to the study onset. GB subjects received a booklet highlighting information about the benefits of walking regularly and encouragement to walk as much as possible in daily life, however, with no written control of their physical activity. The booklet also contained information about the dangers of smoking. It was self-explanatory, with some drawings, pictures, and simple tips on how to increase physical activity in daily life, such as: taking the staircase instead of the elevator; giving preference to walk rather than drive when shopping or going somewhere closer to home; walking the dog more often; taking advantage of spare time and weekends not only to rest but also for walking and hiking, instead of sitting in front of the television for a long time. The procedure of delivering the booklet included reading only parts of the pamphlet where the importance of physical activity was highlighted, but as happens in most motivational booklets, subjects were instructed to read on their own during the period of one month and turn the tips into proposals of change of daily habits.
In order to stratify the included subjects according to their level of physical activity in daily life, the baseline number of steps/day was used to divide the subjects of both GP and GB into 2 subgroups: physically active (subjects who achieved a daily average of 10,000 steps in the initial assessment) and physically inactive (subjects who did not achieve this daily average).
Lung Function Assessment (Spirometry)
Simple spirometry was performed according to the American Thoracic Society and European Respiratory Society guidelines.20 The device used was the Spirobank G (MIR —Medical International Research, Rome, Italy), and reference values were those from the Brazilian population.21
Functional Exercise Capacity Assessment
The 6MWT was carried out according to international standards22 in a 30 meter corridor. Two tests were performed, with at least 30 min of interval, and the highest value was used for analysis. The reference values were those from Gibbons et al.23
Assessment of Physical Activity in Daily Life
The individual level of daily physical activity was assessed through 6 days of monitoring with a pedometer, from Sunday to Friday. The subjects were instructed to reset the device and place it at the waist just after waking up, and remove it just before bedtime. In addition, subjects were also instructed to remove the device only when bathing or when extremely necessary, and not to manipulate the buttons or any other part of the instrument at any time during the day, at risk of losing data. Concomitantly with the pedometer, subjects received a diary in which they reported the time they started using the device in the morning, the time in the evening that they removed it, and the number on its display at the time. In the diary, the subject also reported if the pedometer was removed during the day, for how long, and why. According to the diary data, the number of steps/day was obtained, and the daily physical activity level was determined by the average of the 6 days of assessment. Pre-protocol assessment was performed in the week immediately before initiation of the 1-month period. Post-protocol assessment consisted of either the last week of the 1-month period in GP or the first week after the 1-month period in GB.
The pedometer used was the Yamax Digiwalker SW-200 (Yamax, Tokyo, Japan), which has been extensively tested by several authors and has been considered one of the most reliable pedometers on the market.24,25
Smoking Habits
Subjects were questioned about their basic smoking habits (ie, time since they initiated smoking, and number of cigarettes/day). From these data the number of pack-years was calculated (multiplying the number of total years of smoking by the number of packs smoked per day).
The degree of nicotine dependence was assessed by the Fagerström Tolerance Questionnaire.26,27 It is an easily understood and quickly applied instrument, and consists of 6 items. The test score allows the classification of nicotine dependence into 5 levels: very low (0–2 points), low (3–4 points), moderate (5 points), high (6–7 points), and very high (8–10 points).
Statistical Analysis
The primary outcome of the study was the number of steps/day. Secondary outcomes included lung function variables, 6MWT, and smoking habits.
Statistical software (GraphPad Prism 5.0, GraphPad Software, San Diego, California) was used. Due to the relatively small sample size, nonparametric statistical analysis was performed, and results are presented as median and interquartile range. For intra-group analysis (pre and post-protocol), the Wilcoxon signed-rank test was used. Comparisons between groups were performed using the Mann-Whitney test. Correlations were evaluated using the Spearman correlation coefficient. Comparison between the number of drop-outs and male/female subjects in each group was performed with the Fisher exact test. Comparisons of proportions taking into consideration the occupational status and the improvement in physical activity were performed with the chi-square test. All tests had a significance level of P ≤ .05.
Results
Sixteen GP and 20 GB subjects did not complete the study. The study flow chart (including the reasons for dropping out) is described in Figure 1. Therefore, the final assessment consisted of 23 individuals in GP and 17 in GB. The proportion of drop-outs in the 2 groups (GB 54% and GP 41%) was not statistically different (P = .35).

Overview of the study.
There was no significant difference between GP and GB in the baseline assessment. The groups' characteristics are described in Table 1. Occupational status of the sample was as follows: 7.5% (3) of the participants were retired, 5% (2) were students, 15% (6) were housewives, and 72.5% (29) worked mostly at administrative tasks, sales staff, and technical jobs, at a variety of companies and public institutions, such as retail shops, schools, banks, and health institutions. When comparing the proportion of formally employed workers versus non-workers (retired, students, and housewives) between the groups GP and GB, there was no significant difference (workers in GP 74% [17 out of 23] and in GB 82% [14 out of 17], P = .47). No participant changed his/her occupational status during the period of the study. When taking into consideration the worker/non-worker status and the presence/absence of improvement in physical activity in daily life in both groups (GP and GB) and in the whole group, no statistical difference was found.
Characteristics of the Study Groups
Out of the 23 smokers included in the GP, 8 were classified as physically active and 15 as inactive according to the baseline assessment of physical activity in daily life. The only difference between the physically active and inactive subgroups in the GP was the number of steps/day (P < .001), with no other baseline differences. Out of the 17 smokers included in the GB, 8 were classified as physically active and 9 as inactive according to the baseline assessment of physical activity in daily life. Once again, the only difference between the physically active and inactive subgroups was the number of steps/day (P < .001), with no other baseline differences (Table 2).
Comparison Between the Subdivision of Group Pedometer and Group Booklet in Physically Active and Physically Inactive Subjects
In the GP the physically active group showed no significant change in the number of steps/day after the protocol (12,330 [10,990–12,640] steps/day vs 12,010 [10,610–12,950] steps/day, P = .84). On the other hand, the physically inactive group showed a significant increase in the number of steps/day after the protocol (7,670 [6,159–9,402] steps/day vs 10,310 [9,483–11,110] steps/day, P < .001), as shown in Figure 2. The post-pre protocol change in the number of steps (Δ steps/day) between GP active and inactive subgroups showed a statistically significant difference (−257 [–1,061 to –934] steps/day vs 2,019 [1,676–4,415] steps/day, respectively, P = .001). These values are equivalent to a 2% average reduction in steps/day in the active subgroup and a 26% average increase in the inactive subgroup.
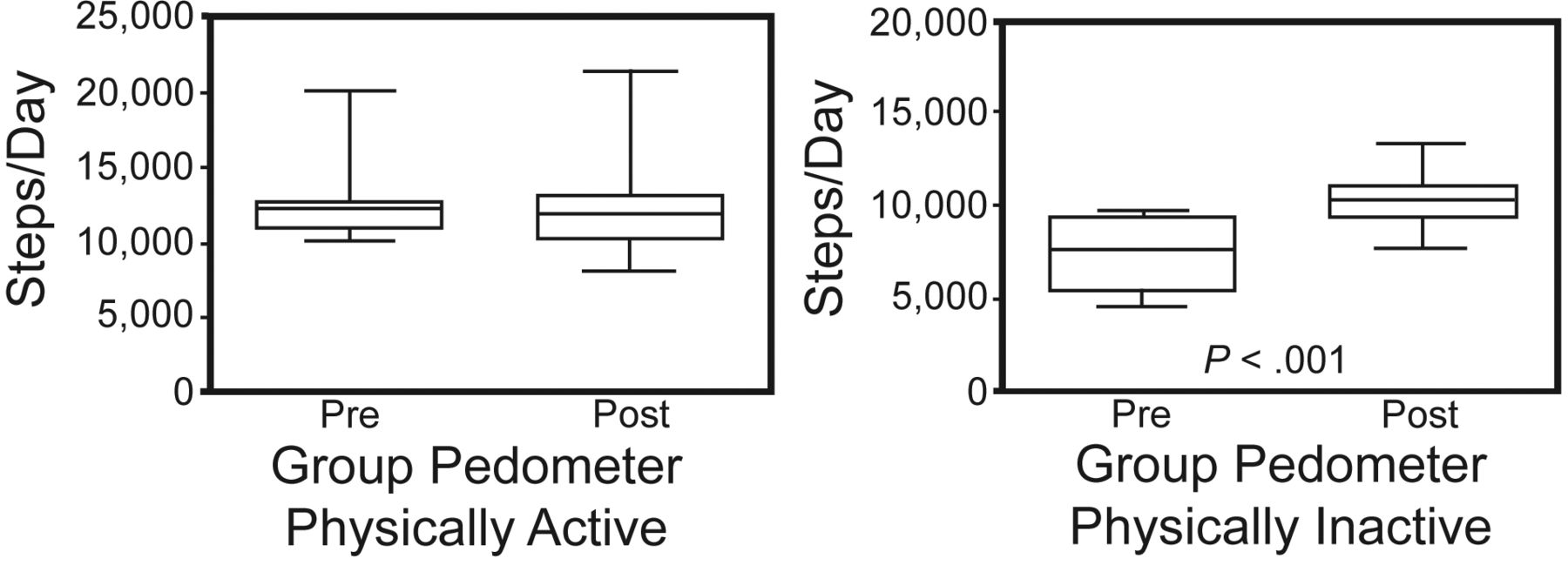
Comparison between number of steps/day pre and post protocol in the physically active and inactive subgroups of group pedometer.
Also in the GP, 100% of subjects initially classified as inactive (n = 15) showed an increase in the number of steps/day after the protocol, and 53% (n = 8) exceeded the target of 10,000 steps/day initially proposed, while another 27% of them (n = 4) reached at least 9,500 steps/day (ie, they reached a difference of < 5% of the target).
In GB the physically active group showed no significant change in the number of steps/day (pre vs post 11,020 [10,830–12,670] steps/day vs 12,180 [11,490–14,120] steps/day, P = .64). The physically inactive group also showed no significant change in the number of steps/day after the protocol (5,982 [3770–7971] steps/day vs 6,848 [3,415–9,346] steps/day, P = .16). The Δ steps/day between GB active and inactive subgroups showed no statistically significant difference (844 [–924 to 2,181] steps/day vs 866 [–524 to 2,790] steps/day, respectively, P = .89).
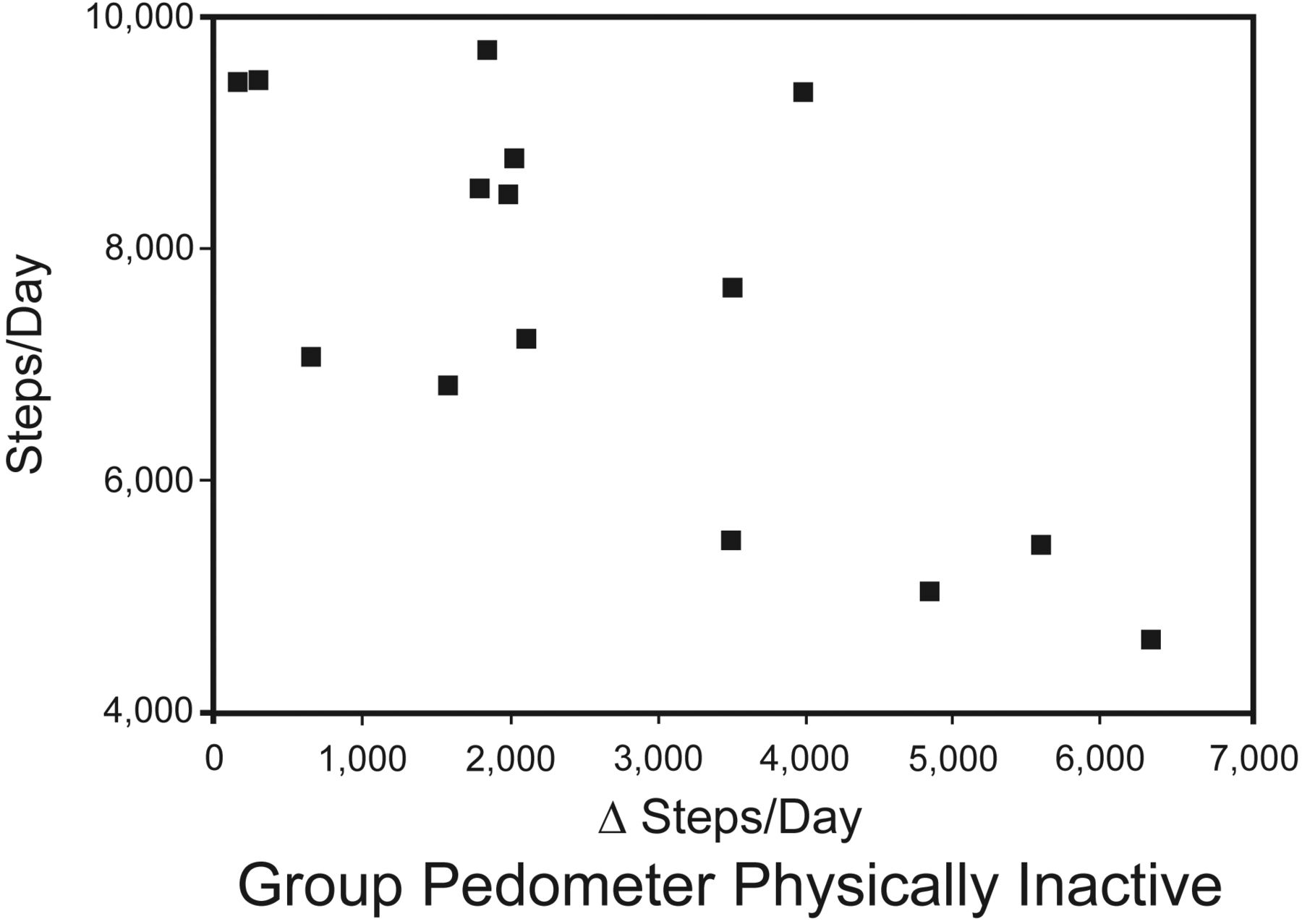
In the GP physically inactive subgroup there was a significant negative correlation of Δ steps/day with the baseline number of steps/day (r = −0.63, P = .01, Fig. 3). In the GB physically inactive subgroup there was no significant correlation of Δ steps/day with any baseline outcome.

Correlation between protocol post and pre changes in steps/day (Δ steps/day) and baseline (ie, pre-protocol) number of steps/day in the physically inactive subgroup of group pedometer (r = −0.63, P = .01)
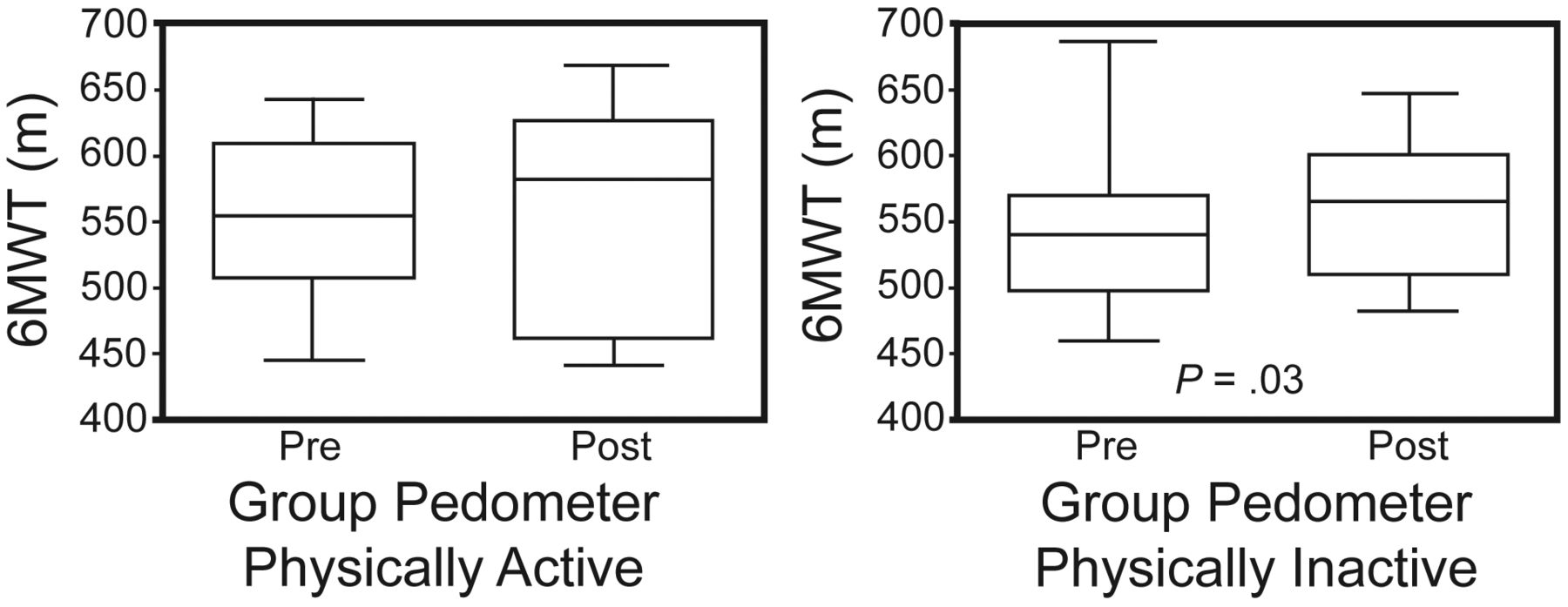
In GP there was a significant increase of 6MWT in the physically inactive subgroup (pre vs post 540 [501–586] m vs 566 [525–604] m, P = .03) (Fig. 4). The improvement in the 6MWT did not correlate significantly with Δ steps/day in this same group (r = 0.28, P = .30). There was no improvement of the 6MWT in the GP physically active subgroup (554 [517–600] m vs 582 [475–622] m, P = .31). In GB the 6MWT also increased only in physically inactive subjects (566 [526–625] m vs 600 [558–647] m, P = .004), but not in the physically active ones (563 [511–607] m vs 580 [510−658] m, P = .15).
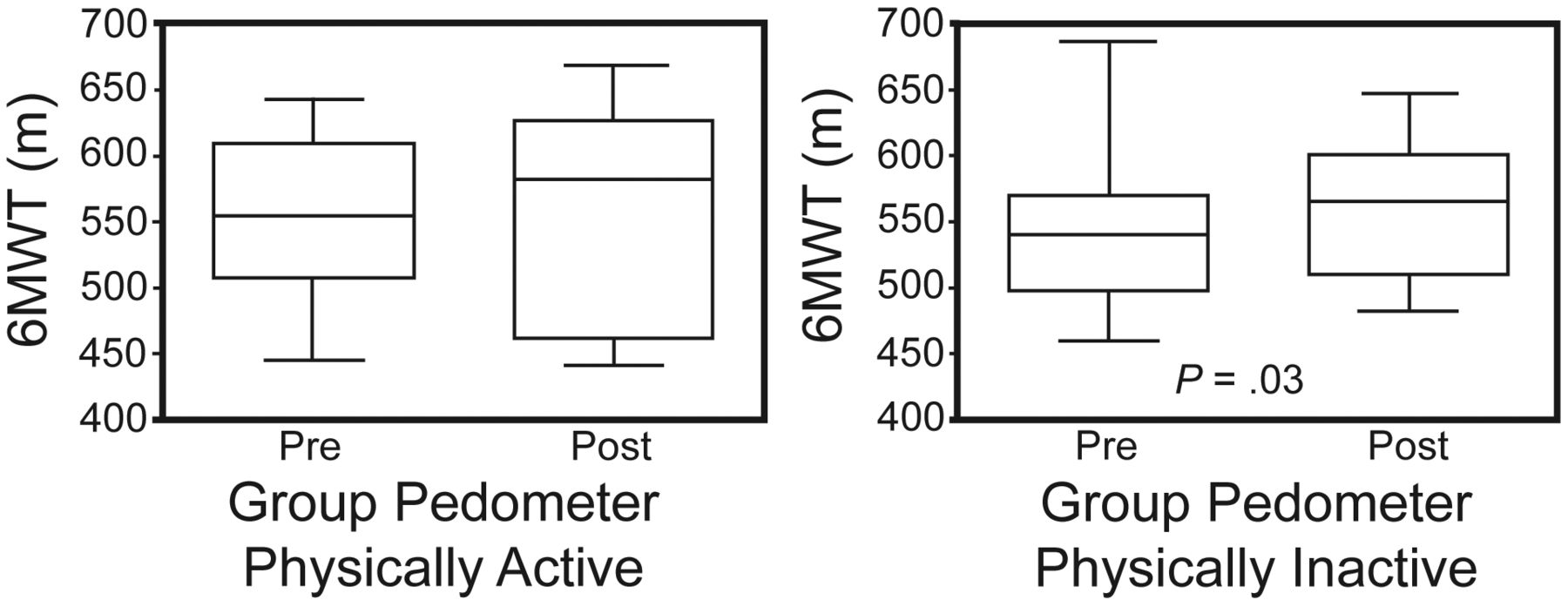
Comparison between 6-min walking test (6MWT) values pre and post protocol in the physically active and inactive subgroups of group pedometer.
Regarding smoking habits, the majority of smokers presented moderate to high nicotine dependence in the GP (47% high and very high dependence, 6% moderate, and 47% low and very low) as well as in GB (48% high and very high dependence, 30% moderate, and 22% low and very low). No significant decrease was found in the number of cigarettes smoked per day after the protocol in GP (pre vs post 20 [16–20] cigarettes/day vs 20 [12–20] cigarettes/day, P = .15), as well as in GB (20 [17–35] cigarettes/day vs 20 [15–30] cigarettes/day, P = .31).
There was no significant correlation between steps/day and the level of nicotine dependence (cigarettes smoked per day, pack-years, and Fagerström Tolerance Questionnaire) in the whole group of smokers (n = 40) at baseline. For further sub-analysis, we added together the active subjects from both GP and GB (n = 16) and inactive subjects from both GP and GB (n = 24), also at baseline. In active subjects there was no significant correlation between steps/day and level of nicotine dependence (r < 0.13 and P > .50 for all). On the other hand, in the inactive subjects, there were significant correlations between steps/day and cigarettes smoked per day, pack-years, and Fagerström questionnaire (r = −0.55, −0.40 and −0.59, P ≤ .05 for all). Furthermore, improvement in steps/day in the inactive subjects of GP (the main target population of the intervention) was correlated with baseline cigarettes smoked per day, pack-years, and Fagerström questionnaire (r = 0.51, 0.65, and 0.53, P ≤ .05 for all).
Discussion
The present study showed that the pedometer, a simple and relatively inexpensive step counter, can be effectively used to promote the increase of daily physical activity in apparently healthy but physically inactive smokers. Moreover, a negative relationship was observed between baseline physical activity and post-protocol change, showing that the subjects who benefit the most from pedometer use as a motivational factor are those with lower levels of physical activity. Since no participant changed his/her occupational status during the study period, it is likely that the improvement in steps/day derives indeed from the pedometer's motivational role. These findings yield important clinical implications, since the use of pedometers is a relatively simple and promising therapeutic option to counteract the disastrous combination of smoking and physical inactivity, and can be used in comprehensive public health campaigns. Since the use of pedometers does not primarily aim at smoking cessation, a combined intervention of pedometers with a smoking cessation program involving counseling and pharmacologic treatment can further enhance the beneficial effects of this instrument.
Prochaska et al19 aimed at using the increase in physical activity as an adjunct factor to smoking cessation, and a small subgroup of their sample used the pedometer with the objective of motivating subjects to increase their number of steps/day. In fact, a 16% average increase in daily physical activity was observed in this subgroup. However, despite these promising results, a characteristic of this study was the fact that the studied subjects were also receiving pharmacologic treatment for smoking cessation, and therefore it cannot be determined if the daily physical activity increase was due to the use of pedometers, the smoking cessation itself, or a combination of both factors. Moreover, according to the same study, the profile of the patients who effectively benefit from the pedometer use in order to increase physical activity could not be identified. The present study is the first to use pedometers as the only intervention in smokers, and the first to divide smokers according to their baseline physical activity level, which fills the gaps in the study by Prochaska et al19 and generates 2 important implications:
An intervention using only pedometers (ie, not accompanied by other smoking cessation measures) can significantly increase the level of daily physical activity of apparently healthy smokers.
The subgroup who actually benefits from the routine use of pedometers is composed of those smokers who are physically inactive.
And, perhaps even more important, the lower the baseline number of steps/day, the greater the increase reached in the physical activity level, to the point that the vast majority of these subjects reach or closely approach the minimum daily physical activity recommendation.
As mentioned earlier, the study by Prochaska et al19 had a 16% average increase of the number of steps/day in smokers submitted to the use of pedometers as a motivational factor. In this study, physically active smokers showed an insignificant reduction in the number of steps/day after the protocol (2% on average), whereas physically inactive smokers had a significant increase (26% on average). This discrepancy in numbers between the 2 studies is clearly due to the fact that the present study divided the subjects into physically active or inactive, since for the whole group (adding active and inactive subgroups), there was an 18% average increase, similar to the 16% observed in the study by Prochaska et al.19
The association between smoking and a sedentary lifestyle is already known; since smoking is described as more prevalent in sedentary people, physical exercise is considered a protective factor against the onset of smoking.28,29 However, in this study, about 60% of smokers were classified as inactive. This classification was based only on the subjects' number of steps/day, but not on the intensity in which this walking activity was performed. Possibly, if an activity monitor had been used to quantify the intensity of the physical activities, the proportion of smokers classified as physically inactive may have been higher, and the results could have been even more encouraging. However, the use of another more technologically advanced device would have a considerably higher cost, which could hinder the implementation of this protocol as a public health strategy. One of the most important implications of this study is precisely the fact that a simple and low cost tool can provide a significant increase in daily physical activity in subjects at high risk, such as physically inactive smokers, which allows the application of comprehensive interventions and tangible short-term benefits in terms of public health.
In addition to the increase in daily physical activity after the protocol, the initially inactive subgroup also improved functional exercise capacity assessed by the 6MWT, although there was no correlation between changes in these 2 outcomes. This is possibly due to the fact that the subjects in general already had a preserved exercise capacity at baseline, as demonstrated by the relatively normal values of 6MWT in terms of percentage of the predicted values (see Table 1). A previous study30 noted that the distance covered by smokers in the 6MWT was significantly lower than expected, indicating more severe exercise tolerance limitation in that population and suggesting that smoking may promote important changes in their functional ability. However, that study used a different formula to calculate predicted values, in comparison to the present one. Also, that study was limited by presenting its data in absolute and predicted values in meters, although the percentage of the predicted values would better reflect the subjects' functional disability. Moreover, the present study also supports the concept that daily physical activity and functional exercise capacity do not necessarily reflect the same domain: functional exercise capacity indicates what the individual is capable of doing, while the daily physical activity indicates what the individual actually does.31
In the same line of reasoning, inactive subjects of GB in the present study showed significant improvement in functional exercise capacity, yet not accompanied by a significant increase in daily physical activity. Although the booklet is more accessible and even less expensive than a pedometer, GB showed a modest (and nonsignificant) increase in daily physical activity. Furthermore, there was a slightly higher drop-out rate in this group, compared to the GP. In combination, these factors may indicate that the booklet was not as effective as the pedometer to counteract physical inactivity in smokers.
At baseline, the present results showed negative correlation between physical activity and smoking habits in sedentary (ie, inactive) smokers, in accordance with the previous literature.32 Interestingly, we have added to the literature the fact that the smokers with worse smoking habits (and consequently lower physical activity levels) are more likely to improve their physical activity level after using the pedometer for 1 month, even without reducing their cigarette consumption during this period of time. As previously discussed, a combined intervention of pedometers with a smoking cessation program involving counseling and pharmacologic treatment might be a very interesting venture for future research.
One possible limitation of the present study was the relatively small number of participants. No sample size was determined prior to initiation of the study. However, the study was powered enough to show relevant and statistically significant differences in the proposed outcomes, notably the primary one. Furthermore, the dropout rate was relatively high; however, similar rates have been previously described in the literature concerning smokers.33,34 We hypothesized that at least one factor may be related to this: despite being smokers, these subjects were apparently healthy by definition, and therefore could have been less prone to pursue a change in daily habits and persevere in it. On the other hand, we cannot rule out that the high dropout rate and relatively small sample size may limit the external validity and generalization of the findings.
Conclusions
These results suggest that physically inactive smokers increase their daily physical activity when submitted to a 1-month simple protocol that uses pedometers to monitor daily number of steps, and more than half of them improve to the point of reaching the minimum recommendation of daily physical activity in order to be considered physically active. Furthermore, in this study the most inactive smokers prior to the protocol were the ones who increased the most their daily physical activity. These preliminary results indicate the pedometer as a promising tool for studies involving health improvement in this population. Future larger studies, involving long-term interventions using pedometers and in combination with smoking cessation programs, can further enhance the beneficial effects of this instrument for public health.
Acknowledgments
The authors would like to thank the colleagues from the Laboratory of Research in Respiratory Therapy, and especially Professor Dr Antonio Fernando Brunetto (in memoriam), for their valuable contributions.
Footnotes
- Correspondence: Fabio Pitta PhD, Departamento de Fisioterapia, Universidade Estadual de Londrina, Rua Robert Koch, 60 Vila Operaria, Londrina, Paraná, 86038–440 Brazil. E-mail: fabiopitta{at}uol.com.br.
This research was partly supported by Fundação Araucária/Paraná, Ministério da Saúde, Brazil. Couto Furlanetto PT was supported by Conselho Nacional de Desenvolvimento Científico e Tecnológico, Brazil.
Dr Pitta presented a version of this paper at the Annual Congress of the European Respiratory Society, held September 18–22, 2010, in Barcelona, Spain.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}
{kind=link}