

Abstract
Inadvertent ventilator triggering can occur for various reasons. Leaks in the ventilator circuit, endotracheal tube leaks, tracheal cuff leaks, cardiac oscillations, water condensate causing oscillations in the circuit tubing, ventilator expiratory valve integrity, and overly sensitive triggering mechanism settings may precipitate this phenomena. We present a case of inadvertent ventilator triggering caused by electrical stimulation of the diaphragm from surgically placed pacing wires post cardiothoracic surgery. A 47-year-old woman underwent surgical placement of a left (LVAD) and right (RVAD) ventricular assist device for severe end stage cardiomyopathy, as a bridge to cardiac transplantation. The patient was observed to have inadvertent ventilator triggering while deeply sedated postoperatively. The ventilator set respiratory rate was 16 breaths/min, with patient respiratory rate of 30 breaths/min while deeply sedated. Upon assessment of ventilator waveforms and arterial blood gas revealing a profound respiratory alkalosis, the pressure/time waveform demonstrated a −2 cm H2O decrease in pressure prior to each cycled breath. The ventilator was subsequently changed from flow trigger sensitivity of 3 L/min to pressure trigger sensitivity of −3 cm H2O to eliminate the autotriggering. Later in the patient's ICU stay, inadvertent ventilator triggering was again observed. Further adjustment of the pressure trigger sensitivity to −3 cm H2O eliminated the autotriggering. Clinical assessment found the pacing wires were responsible for stimulating the patient's diaphragm, therefore causing airway pressure decreases and premature breath delivery. Once the electrical amplitude of the pacemaker was decreased, the inadvertent ventilator triggering resolved and normal trigger sensitivity and pH was restored.
- inadvertent triggering
- autotriggering
- external pacemaker
- pressure trigger
- flow trigger
- waveforms
- respiratory alkalosis
Introduction
Inadvertent ventilator triggering is the unintended initiation of breath delivery by the mechanical ventilator. This phenomenon occurs for various reasons such as circuit, endotracheal, and tracheal tube cuff leaks; cardiac oscillations; pressure oscillations created from the movement of condensate water in the ventilator circuit; ventilator expiratory valve integrity; and over-sensitive triggering mechanism setting.1–5 Medical complications such as decreased pulmonary vascular resistance, arrhythmias, tachycardia, seizures, hypokalemia, and decreased urine output can be associated with the resultant hyperventilation induced respiratory alkalosis.6 Furthermore, there are reported cases of inadvertent breath triggering in patients with brain death who failed apnea testing, resulting in delayed brain death determination.7
Modern ventilators are manufactured with either a pressure or flow triggering mechanism to initiate an assisted breath. Ventilator operators set either an inspiratory pressure or flow threshold that must be met for breath initiation.8 We report a case of inadvertent ventilator triggering associated with the use of flow trigger sensitivity setting, secondary to diaphragmatic contraction due to electrical stimulation from pacing wires placed at the time of right (RVAD) and left (LVAD) ventricular assist device placement in a patient with end stage cardiomyopathy. The inadvertent ventilator triggering was initially resolved by changing the trigger sensitivity to pressure trigger, and eventually by reducing the pacemaker's electrical amplitude.
Case Report
A 47-year-old woman was admitted to the cardiac surgery ICU with severe end stage cardiomyopathy following placement of RVAD and LVAD for biventricular cardiac support as a bridge to heart transplantation. The patient had a previous implanted permanent internal pacemaker and transthoracic pacing wires placed at the time of her current surgery. During the cardiothoracic procedure it was found that the internal pacer wires had been transected, necessitating the need for external pacing. Four days following a complicated postoperative course, while the patient was heavily sedated on high dose sedation/analgesia and multiple pressors, an arterial blood gas revealed a respiratory alkalosis (pH 7.61, PaCO2 23 mm Hg) secondary to hyperventilation. Ventilator settings using the Galileo ventilator (Hamilton, Bonaduz, Switzerland) at the time were pressure control continuous mandatory ventilation mode, pressure control setting of 25 cm H2O, target exhaled tidal volume 300 mL (8.8 mL/kg predicted body weight), PEEP 5 cm H2O, flow trigger setting of 3 L/min, set respiratory rate of 16 breaths/min, and a measured total patient respiratory rate of 30 breaths/min.
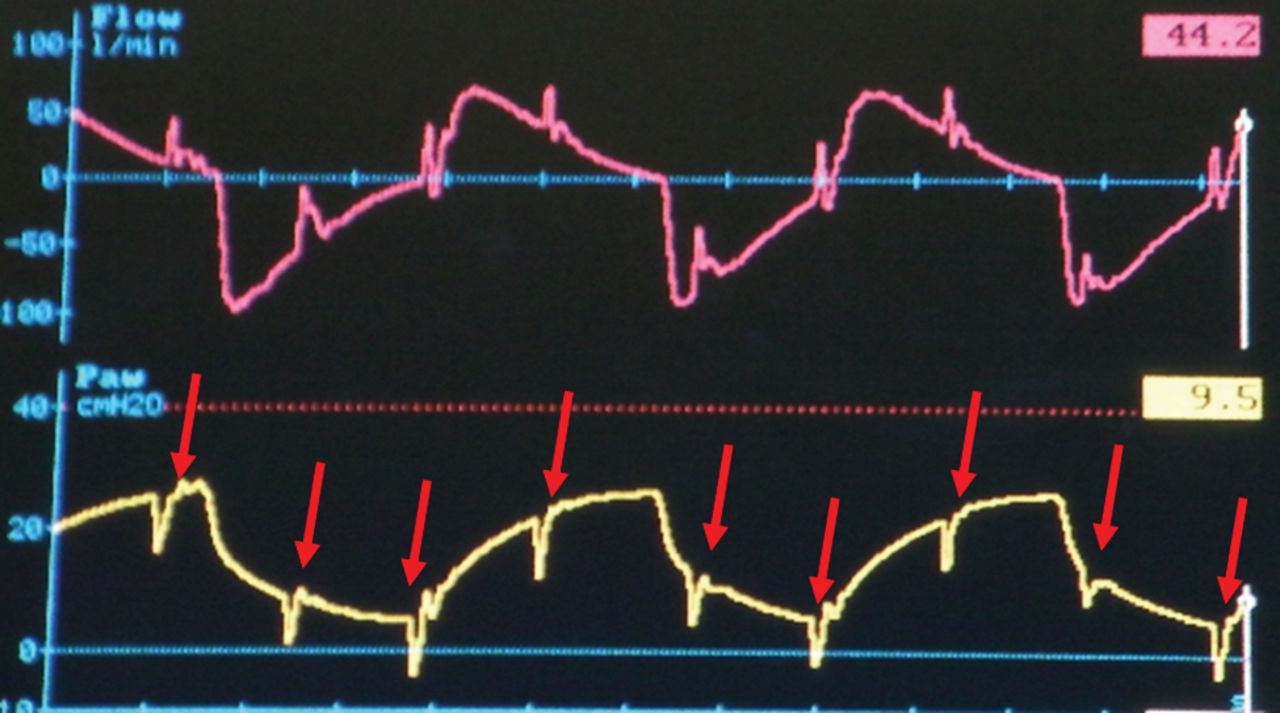
It was determined that the ventilator was autotriggering, and the suspected cause initially was cardiac oscillations from the ventricular assist devices. The pressure/time waveform demonstrated a −2 cm H2O decrease in pressure prior to each delivered breath. The ventilator was subsequently changed from flow-trigger sensitivity of 3 L/min to pressure trigger sensitivity of −3.0 cm H2O to eliminate the inadvertent triggering. Four days later an arterial blood gas revealed a pH of 7.55 and a PaCO2 35 mm Hg with the patient well sedated and utilizing a pressure trigger setting of −3.0 cm H2O. Once again there was a suspicion of inadvertent triggering. An assessment of circuit integrity, including checking for leaks in the circuit connections, endotracheal tube cuff, and humidifier canister, was performed without a resolution of the problem. With inspection of the ventilator waveforms and increasing pressure trigger sensitivity to −5 cm H2O, decreases in airway pressure were observed, which coincided with the patient's heart rate (Fig. 1).

Six second sweep of flow/time and pressure/time waveforms prior to pacer amplitude change. The arrows depict an airway pressure (Paw) decrease with each diaphragm contraction. Total patient respiratory rate of 30 breaths/min with ventilator set rate at 16 breaths/min. Instances of cardiac contractions are 90 beats/min, matching pacemaker rate.
Specifically, the pressure-time waveform displayed rhythmic negative deflections mimicking diaphragm contractions through all phases of the ventilator breath waveform. Further inspection with close physical examination revealed slight contraction of the diaphragm with each heart contraction. Subsequently the atrial pacing wire output from the external pacemaker box was adjusted from 20 to 10 milliamps, with resolution of inadvertent triggering (Fig. 2). Reproducible observations of inadvertent triggering at the 20 milliamp energy level allowed us to determine that the patient's external pacemaker was the cause of the inadvertent breath triggering. We hypothesized that the electrical energy from the wires was in close enough proximity to the diaphragm that it caused the diaphragm to contract.

Twelve second sweep of flow/time and pressure/time waveforms following pacer amplitude adjustment from 20 to 10 milliamps. Set and patient total respiratory rate is 16 breaths/min.
Discussion
This case demonstrates a situation in which ventilator waveforms confirmed the presence of ventilator autotriggering and that by adjustment of pacing wire pacemaker amplitude settings we could eliminate inadvertent breath triggering in a reproducible fashion. We were then able to use normal trigger settings and correct the severe respiratory alkalosis caused by the pacer-induced diaphragmatic contraction. After discussion with ICU nursing staff, it was found that pacing amperage adjustment is a common practice to obtain electrical capture of either the atrium or the ventricle. Capture is defined as the depolarization of the atria and/or ventricles by an artificial pacemaker, thereby stimulating the heart to contract.9 The amount of energy required to capture can change over time because of endothelial tissue injury around the electrode tips.9 Undetected pacemaker-induced inadvertent ventilator triggering can cause respiratory alkalosis secondary to hyperventilation.5 At an increased respiratory rate this could potentially lead to autoPEEP with resultant hypotension from increased intrathoracic pressure, decreased urine output, weaning difficulties, decreased cardiac output, and the patient's being unable to trigger the ventilator.10
With the newer microprocessor ventilators, interpreting waveforms has become an essential skill for the bedside therapist. However, even though waveform analysis is a very important part of our ventilator assessment, we were unable to initially diagnose the real reason for the autotriggering. Regardless of which type of triggering method was used, this case study illustrates the effect that other patient care devices can have on our ability to ventilate patients. As a result we are more aware of inadvertent ventilator triggering and better able to intervene by either manipulating the cardiac device or the triggering method used.
Footnotes
- Correspondence: Timothy E France RRT, Department of Respiratory Care, Sentara Norfolk General Hospital, 600 Gresham Drive, Norfolk VA 23507. E-mail: tefrance{at}sentara.com.
Mr France and Mr Grooms have disclosed relationships with Hamilton Medical. Dr Garnett has disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}