

Abstract
A 27-year-old woman was admitted to our ICU with acute hypoxemic respiratory failure and criteria for ARDS. Despite an FIO2 of 1.0 and a lung protective strategy, the patient died on day 15 without any improvement. The relatives gave consent for post-mortem analysis. The histopathologic study of the lung showed findings typical of an acute fibrinous and organizing pneumonia. Apropos of this case we performed a PubMed search. We found 13 articles, including a total of 29 patients. Acute fibrinous and organizing pneumonia is an unusual cause of acute lung injury. The diagnostic criterion is histopathologic. There is little information regarding the pathophysiology of this illness. Important questions remain regarding this disease, including predisposing factors and management. Patients who require mechanical ventilation have poor outcomes.
Introduction
Acute lung injury and ARDS are defined as an illness having an acute onset, with a PaO2/FIO2 ≤ 200 mm Hg (or ≤ 300 mm Hg for acute lung injury), the presence of bilateral infiltrates on frontal chest radiographs, and a pulmonary artery occlusion pressure ≤ 18 mm Hg if measured, or no clinical evidence of left atrial hypertension when not measured. There are a group of diffuse, noninfectious parenchymal lung diseases that often present in an acute fashion and fulfill all of the clinical, physiologic, and radiographic criteria for acute lung injury and ARDS. Some of these have distinct bronchoalveolar lavage characteristics and/or specific histologic findings.1 We present a patient with clinical criteria of ARDS but with histologic findings in the lung biopsy compatible with an acute fibrinous and organizing pneumonia.
Since its original description in 2002, few cases of acute fibrinous and organizing pneumonia have been reported in the literature. A PubMed search up to 2010 was conducted using the search terms acute fibrinous pneumonia and organizing pneumonia. The search was limited to adults, and no language restriction was used. Twenty-one articles were found in this search. We excluded 9 articles: 2 articles that included children, 3 articles describing other diseases, 3 articles that were editorial, reviews, or letters, and one describing adverse effects of amiodarone. We added another article after having reviewed the references of selected articles. Thirteen articles were finally included in this review, and represent a total of 29 patients (Table 1).2–14
Summary of Reported Cases of Acute Fibrinous and Organizing Pneumonia
Case Report
A 27-year-old woman with a medical history of Marden-Walker syndrome (a developmental disorder of the central nervous system, of which the main diagnostic criteria are blepharophimosis, congenital joint contractures, and mask-like face, and, as in our case, a patent ductus arteriosus (surgically corrected), ectopic spleen (removed due to thrombocytopenia), pneumococcal vaccine post-splenectomy, ureter duplication on the right side, for vesicoureteral reflux and recurrent urinary tract infections, and bronchial hyper-responsiveness. Since 1998 she had a permanent tracheostomy and nocturnal home oxygen therapy.
She was in her usual state of health until 2 days before presentation, when she developed shortness of breath and fever. She was started on antibiotic therapy without an improvement. On physical examination, at presentation to the emergency department, vital signs included a temperature of 38.5°C, a pulse of 130 beats/min, blood pressure of 84/50 mm Hg, respiratory rate of 35 breaths/min, and an arterial oxygen saturation of 75% while breathing ambient air. Cardiac examination was notable for a regular tachycardia without murmurs, and auscultation of the lung fields revealed rhonchi. Admission laboratory data were notable for a white blood cell count of 13,800 cells/μL, a C-reactive protein of 76.5 mg/L (reference value < 6 mg/dL), and a procalcitonin of 12.2 ng/dL (reference value < 0.5 ng/dL).
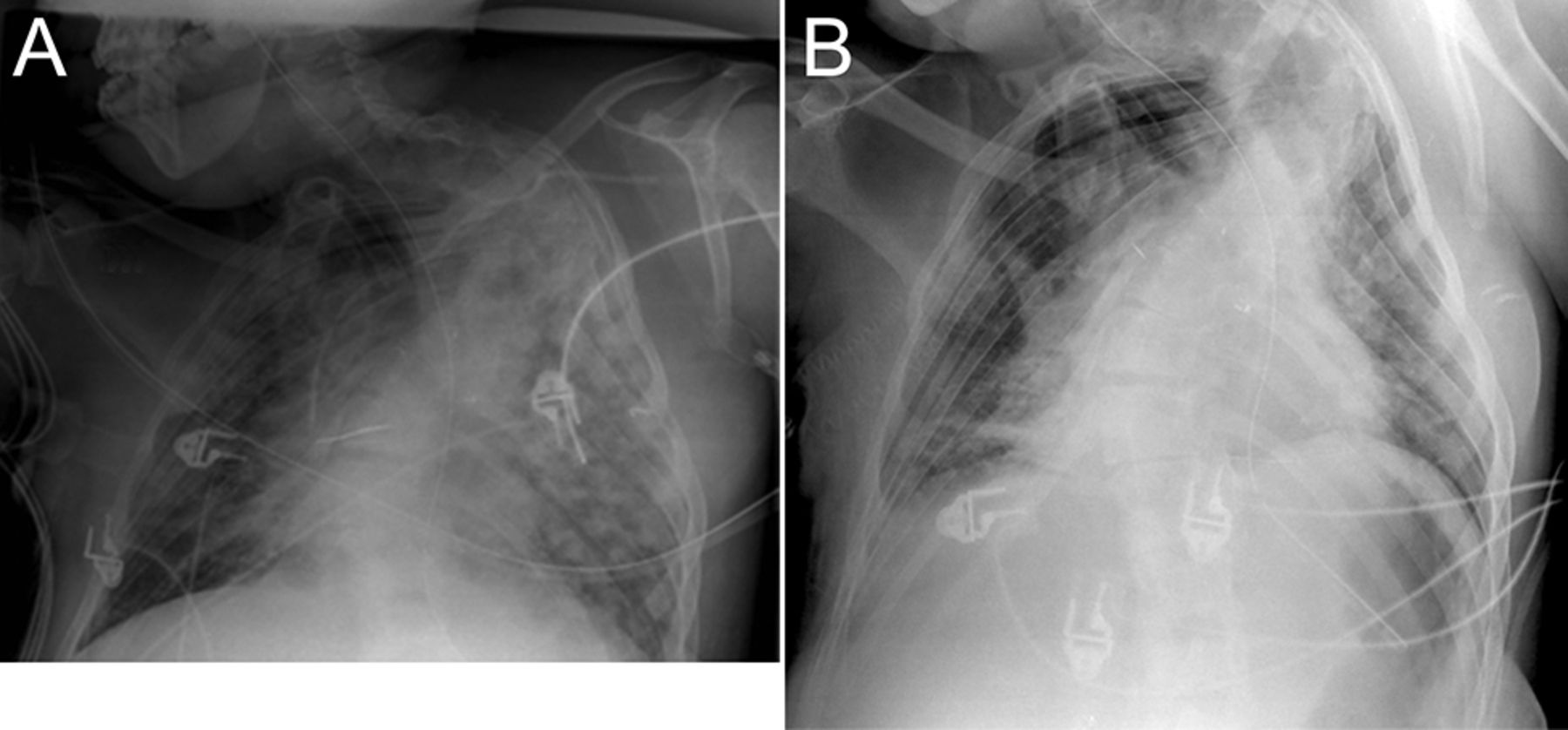
The patient was given bronchodilators and intravenous steroids, without any improvement in oxygenation. Suddenly she had a cardiac arrest, in asystole, recovering rhythm and pulse after 5 min of cardiopulmonary resuscitation. The patient was admitted to ICU. On admission the patient met criteria of sepsis secondary to healthcare associated pneumonia. She was given vancomycin, ceftazidime, and amikacin. All the microbiological samples and urine antigen tests for Legionella and Streptococcus pneumoniae were negative. Chest roentgenogram (Fig. 1) revealed diffuse and bilateral infiltrates, and arterial blood gas analysis obtained while she was on mechanical ventilation with an FIO2 of 1.0 showed a PO2 of 70 mm Hg, confirming the clinical diagnosis of ARDS.

A: At admission in the ICU. B: At day 13 after admission the chest x-ray revealed diffuse and bilateral alveolar infiltrates.
She was ventilated with continuous mandatory ventilation with AutoFlow mode (Evita 4, Dräger, Lübeck, Germany), a tidal volume of 400–450 mL (corresponding to 6–8 mL/kg of predicted body weight), a respiratory rate to maintain a PaCO2 of 40–45 mm Hg, a PEEP of 0 cm H2O (the compliance worsened with PEEP > 5 cm H2O), and the inspiratory-expiratory ratio ranged from 1:1 to 1:3. Despite the lung-protective ventilatory strategy, high airway pressures were detected (plateau pressure > 35 cm H2O). She required cardiovascular support with norepinephrine, and developed a hematologic dysfunction (anemia, thrombocytopenia, and coagulopathy). From admission, she had clinical criteria of anoxic encephalopathy (best Glasgow coma score 8 points, and myoclonus) with a serum neuron-specific enolase concentration of 45 μg/L (reference value 15 μg/L). After 15 days of management without improvement, the support assistance was withdrawn. Her relatives gave consent for post-mortem analysis.
The pathologic study of the lung showed patchy involvement of lung parenchyma by fibrin deposits in the form of “fibrin balls” in alveolar ducts and alveoli, and diffuse organizing pneumonia (Fig. 2). These findings are typical of an acute fibrinous and organizing pneumonia.2

A: The specimens from the left upper lung lobe show alveolar spaces filled with fibrinous and neutrophilic plugs, alternating with fibroid polyps (organizing pneumonia). Hyaline membranes and eosinophils are absent. Hematoxylin and eosin stain (40×). B: Other view from the same lung lobe, showing intra-alveolar fibrin “balls” associated with neutrophilic infiltrates, characteristic features of fibrinoid pneumonia. Hematoxylin and eosin stain (40×).
Discussion
In 2002, Beasley et al2 described a new histological pattern of diffuse infiltrative lung disease that was termed acute fibrinous and organizing pneumonia. The characteristic histological pattern of acute fibrinous organizing pneumonia is an intra-alveolar deposit of fibrin forming fibrin balls and an organizing pneumonia with a patchy distribution. This pattern, and the absence of hyaline membranes and extensive abscess formation, distinguishes this entity from diffuse alveolar damage and bronchiolitis obliterans organizing pneumonia. A lack of prominent eosinophilic infiltrates makes it different from eosinophilic pneumonia.
So far, excluding our case, 29 cases of this entity have been reported (see Table 1). This disease has been described more often in males in the fifth to sixth decade of life. In most of the reported cases no risk or predisposing factor was found.2–4,10–12 However, it has been associated with infection,2,13 connective tissue disorders,2,6,12 hematological malignancies,2,7 and occupational and drug exposure.2,5,9 In our case, we suspect the infectious etiology. She had an increase in the biomarkers of infection (leukocytosis, high levels of C-protein reactive and procalcitonin). Nevertheless, all cultures obtained were negative, although the patient had received antibiotherapy previous to admission to hospital.
Presenting symptoms of this pulmonary disease can be acute or subacute. Beasley et al2 described 2 different patterns of disease progression and outcome: acute illness with rapid progression to death, and a subacute course (onset of dyspnea and cough of < 2 months of evolution) with recovery. The subacute course occurs more often2–6,8–13 than the fulminant form of the disease.2,7 Our patient had an acute onset of the illness (symptoms began 2 days before coming to the hospital) requiring mechanical ventilation from admission to hospital. At admission, she met clinical criteria of ARDS, but the histological pattern did not show diffuse alveolar damage, the histopathologic finding that corresponds to the clinical entity of ARDS. So we could consider acute fibrinous and organizing pneumonia as another “imitator” of ARDS.1
Different radiological patterns have been described for this entity. The most common finding is a bilateral patchy infiltrate. Because of its patchy distribution, the definitive diagnosis requires an open lung biopsy. Schwarz and Albert1 suggest that patients thought to have ARDS without a defined predisposing condition should undergo bronchoalveolar lavage. If the bronchoalveolar lavage results are not specific, a lung biopsy should be attempted to establish a definitive diagnosis, and an appropriate therapy should be administered. In our literature review, in 31% (9 of 29 patients) a bronchoalveolar lavage was performed before obtaining lung biopsy. No conclusive findings were found. In all the cases, histopathologic samples were necessary for the definitive diagnosis.
Acute fibrinous and organizing pneumonia has no specific treatment. In 11 cases2,4,8,9 the initial treatment was antibiotherapy, because symptoms and chest radiographs can be compatible with pulmonary infection. Also, steroids have been used in this entity: after antibiotherapy, due to a lack of response2,4,9,11,13; at the same time as antibiotics2,5,7; or as initial treatment.2,3,6,10,12 In some of the cases related with drugs, the discontinuation of the responsible agent was enough for improvement.5,9
In conclusion, acute fibrinous and organizing pneumonia is an unusual cause of acute lung injury. The diagnosis is histopathologic. There is little information regarding the pathophysiology of this illness. Many important questions remain regarding this disease, including predisposing factors and management. Patients who require mechanical ventilation have a poor outcome.
Footnotes
- Correspondence: Sonia López-Cuenca MD, Intensive Care Unit, Hospital Universitario de Getafe, Carretera de Toledo Km 12.500, 28905 Getafe, Madrid, Spain. E-mail: sonia_l_c{at}hotmail.com.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}