

Introduction
For acute respiratory distress or arrest, endotracheal intubation is a life-saving procedure in emergency airway management. There are many possible complications that may present with manipulation of the airway. This case will discuss factors that one may consider when adequate oxygenation or ventilation is not achieved after an endotracheal tube (ETT) is placed. Issues that can lead to difficulty in ventilation should be rapidly identified and reversed if respiratory acidosis, hypoxemia, and respiratory arrest are to be avoided. These include causes of air trapping, such as asthma or foreign body aspiration; ETT obstruction due to biting, tube kinking, or mucus plugging; and external lung compression from pneumothorax, hemothorax, or diaphragm rupture.
Case Summary
A 13-year-old, 40 kg male sustained a closed head injury after a bicycle accident. He was found unresponsive at the scene and was intubated in the field. He was then transferred to the emergency department by helicopter. The patient arrived with a 6.0 mm internal diameter (ID) ETT in place. The ETT was secured to a depth of 18 cm, measured at his upper lip. On initial presentation in the emergency department, the patient had equal, yet slightly diminished breath sounds. SpO2 was 100% with ventilation via a self-inflating resuscitation bag connected to 50 psi medical wall oxygen at 15 L/min. Adequate chest rise was assessed, and there was little resistance noted with manual ventilation. A monitor (Microstream CO2, Nellcor/Covidien, Boulder, Colorado) was attached between the ETT and the resuscitation bag, and the measured reading was 45 mm Hg. A chest x-ray was promptly obtained and revealed ETT placement with the tip at the level of the third thoracic vertebrae. Lung fields were clear, with no focal infiltrate, effusion, or pneumothorax. No fractures were seen (Fig. 1).

Chest x-ray upon admission.
The patient was placed on a mechanical ventilator (LTV 1000, CareFusion, San Diego, California), in pressure control synchronized intermittent mandatory ventilation (SIMV) mode, with a distending pressure of 25 cm H2O, a PEEP of 5 cm H2O, and an FIO2 of 1.0. Exhaled tidal volumes initially measured 300–320 mL. The patient was expeditiously transported to the CT scanner by order of the emergency department physician for the evaluation of the cervical spine, brain, chest, abdomen, and pelvis. After being moved onto the scanner table, the patient became increasingly difficult to ventilate. Breath sounds became further diminished and a decrease in chest rise was noted. Exhaled tidal volumes measured 80–120 mL, and the pressure alarm limit set at 35 cm H2O alarmed repeatedly. A 12-French suction catheter was introduced, met resistance, and thus was unable to be passed through the ETT. The patient was immediately taken off the ventilator and ventilated again with a resuscitation bag. Breath sounds were reassessed and were present yet diminished upon auscultation. The end-tidal CO2 monitor was utilized and read 70 mm Hg. An anesthesiologist was called immediately to the CT scanner to re-intubate the patient. When the anesthesiologist deflated the ETT cuff in preparation for extubation, the patient immediately began showing signs of improved compliance, chest rise, and respiratory status. The managing physician (author REL) was notified of the clinical changes and was requested to come and help evaluate possible causes. The CT images of the chest were reviewed (see Fig. 2). The images revealed that the cuff of the ETT was excessively over-inflated, to the point of near complete airway occlusion with tamponade of the ETT (see Fig. 2B). The remainder of the CT scan did not reveal any other anatomical abnormalities.
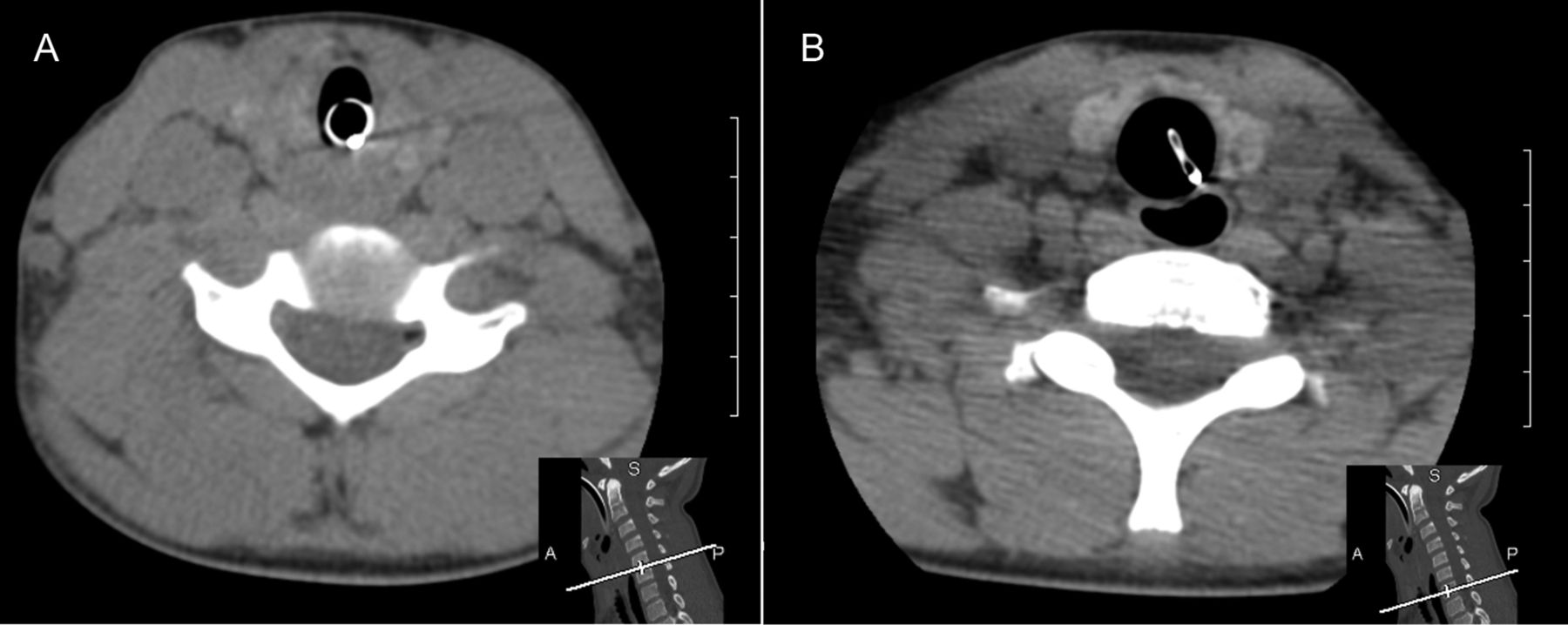
Computed tomography shows (A) full diameter of the endotracheal tube, and (B) obstruction of the endotracheal tube from excessive cuff pressure at level C7.
Discussion
Prior to this clinical scenario, we were unaware that it was possible to occlude an ETT by over-inflation of the cuff. A literature search through the PubMed database, using the key words endotracheal occlusion and obstruction, in the English language, revealed only one prior reported case of obstruction of the cross-sectional area of an ETT by over-inflation of the cuff.1 Our team attempted to mimic ETT collapse by cuff-overinflation in a non-clinical setting. We introduced air into the cuffs of ETTs of various sizes (IDs of 3.5, 4.0, 4.5, 5.0, 5.5, 6.0, 6.5, 7.0, 7.5, and 8.0 mm) and from varying manufacturers. The ETTs were heated to approximately 37°C, to mimic body temperature prior to testing the cuff. The ETTs were placed individually in the barrel of one of the following: a 3 mL, 5 mL, 10 mL, or a 12 mL syringe, depending on the size of the ETT. The cuffs of the ETTs were inflated with excess air. The inner diameters of the ETTs were then visually observed for possible occlusion. The results of this experiment demonstrated partial and near complete occlusion of the ETT with the introduction of ≥ 10 mL of air into the pilot balloons of ETTs ranging from sizes 3.5 mm ID to 6.5 mm ID. Cuff pressures measured were in excess of the 120 cm H2O maximum reading on the manometer (Cufflator, Posey, Arcadia, California) (120 cm H2O =88 mm Hg, and 1 mm Hg = 1.36 cm H2O). We were unable to replicate obstruction in the larger tubes, sizes 7.0 mm, 7.5 mm, and 8.0 mm ID. This basic experiment allowed us to conclude that over-inflation of air in the cuff of the ETT may obstruct the airway in ETTs ranging from 3.5 mm to 6.5 mm ID (Fig. 3).

Endotracheal tube (6.0 mm inner diameter) with over-inflated cuff. On the right, the tube and cuff are inside the barrel of a 10 mL syringe. Note the partial occlusion of the tube.
There are several acute management steps to consider when assessing the deterioration of ventilation or oxygenation in an intubated patient. It is common practice to extubate the patient when cardiopulmonary status is deteriorating, due to the possibility of ETT complications, and to provide bag mask ventilation or re-intubate. Use of the DOPE mnemonic, as outlined by the Pediatric Advanced Life Support guidelines, to troubleshoot acute deterioration in a mechanically ventilated patient, may be helpful. As a reminder, D is for dislodgement of the ETT, O is for obstruction of the ETT, P is for suspected pneumothorax, and E is for equipment or operator problem.2
In the mechanically ventilated patient, obstruction of the airway should be suspected by observing abnormally high peak inspiratory pressures, a decrease in compliance of the lungs, an increase in resistance to inflation, and a notable difference between measured inhaled and exhaled tidal volumes. Obstruction in the intubated patient may also be identified by passing an appropriate size suction catheter to assure patency of the ETT. Other things to consider are equal breath sounds upon auscultation, review of the chest radiograph to assess appropriate ETT position, the observation of dampened chest rise with manual or mechanical ventilation, and a change in vital signs and saturation. End-tidal CO2 monitors and end-tidal CO2 detection devices may be of benefit for assuring airway patency and the position of the ETT.
As reflected in this case, occlusion of the ETT due to hyperinflation of the cuff might be remedied by frequent measurement and adjustment of the ETT cuff pressure. There are several cuff inflator measuring devices available to evaluate the cuff pressures of the ETT. When intermittently connected to the pilot balloon these devices measure the pressure of the cuff. The therapist can then inflate or deflate the cuff to the desired measurement (Cufflator, and Endotest, Rusch/Teleflex, Limerick, Pennsylvania). There is another cuff pressure controller device on the market (PressureEasy, Smiths Medical, St Paul, Minnesota) that continuously monitors tracheal cuff pressure; connected to the pilot balloon, an indicator color signals that the cuff pressure is within the recommended limit.
A study by Svenson et al revealed that many patients intubated in the emergency department or pre-hospital setting did not routinely have the ETT cuff pressure measured, and, when measured, the pressure was too high (> 40 cm H2O) in 58% of the patients.3
Although more and more practitioners are measuring cuff pressure immediately after intubation, this practice has not become commonplace or the standard of care.4
Teaching Points
Cuff pressures should be measured immediately post intubation and routinely in all intubated patients.
Even a slightly over-inflated cuff can exert too much pressure against the trachea, which may impede mucosal blood flow and eventually cause ischemic complications.5 It is recommended to maintain cuff pressure > 18 mm Hg to prevent aspiration, and < 25 mm Hg to reduce the risk of tracheal ischemia6 and ETT obstruction.
When assessing the ETT for obstruction, it is always important to assess whether the cuff pressure is within recommended normal limits.
Footnotes
- Correspondence: Kevin M Johnson RRT-NPS, Department of Respiratory Care, Santa Barbara Cottage Hospital, 400 West Pueblo Street, Santa Barbara CA 93105. E-mail: kjohnson{at}sbch.org.
The authors have disclosed no conflicts of interest.
- Copyright © 2012 by Daedalus Enterprises Inc.





{kind=link}
{kind=link}
{kind=link}