

Abstract
BACKGROUND: Hospital admissions for COPD exacerbations account for 70% of total costs of COPD treatment, and the duration of hospital stay is directly related to this cost. The aim of this study was to investigate possible associations of demographic, clinical, laboratory, and functional parameters with stay of subjects admitted for COPD exacerbations and to provide a score for the prediction of the need for prolonged hospitalization.
METHODS: We included 164 consecutive subjects admitted to 2 respiratory medicine departments of 2 tertiary hospitals for a COPD exacerbation, and we evaluated laboratory, clinical, and functional parameters possibly related to the duration of hospital stay.
RESULTS: Seven parameters evaluated on subject admission (Antonisen type of exacerbation, number of Exacerbations in the previous year, Charlson index of comorbidities, Oxygenation, Partial pressure of PaCO2 in arterial blood gases, Dyspnea according to the Borg dyspnea scale, and history of chronic respiratory Failure) were able to predict stay and were included in a simple score named AECOPD-F. The area under the curve of the score for the prediction of prolonged hospital stay is 0.960, and a cutoff point ≥ 3 predicts prolonged stay with a sensitivity of 84.5% and a specificity of 92.5% (95% CI 0.917–0.984). The AECOPD-F score was validated in a second group of 88 subjects admitted to the hospital for a COPD exacerbation. In the validation group, subjects with a score ≥ 3 required prolonged stay compared with those with a score < 3 (8.0 [6.0–10.0] vs 6.5 [4.0–9.0] d, respectively, P = .007).
CONCLUSION: The AECOPD-F score could accurately predict stay in hospitalized COPD subjects. The implementation of this score in clinical practice could be useful in the discharge planning of such subjects.
Introduction
COPD is a leading cause of morbidity and mortality worldwide and results in an economic and social burden that is both substantial and increasing.1 COPD is one of the most common causes of acute hospital admission.2 A significant proportion of the cost of managing COPD is attributed to hospital admission due to exacerbations.3 It has been estimated that hospital episodes account for 70% of the total costs of COPD treatment.4 The cost of hospitalization is also significantly influenced by the duration of hospital stay.5 Consequently, the duration of in-patient episodes due to an exacerbation of COPD and related factors has attracted significant attention from health care providers.6,7
Despite the tremendous burden of hospital admissions, few studies have the duration of hospital stay and its association with subjects' characteristics as primary short-term outcome parameters.3,7–12 Such knowledge could help clinicians to identify subjects who require intensive treatment, targeting therapeutic goals to encounter all the parameters that are relevant to increased stay to allow for better utilization of medical resources.
The aim of the present study was to investigate possible associations of demographic, clinical, laboratory, and functional parameters with stay of subjects admitted with a COPD exacerbation and to create a simple score for the recognition of patients who will require prolonged stay. The understanding of these influences will help optimize care for COPD patients needing hospital admission.
QUICK LOOK
Current knowledge
COPD is a leading cause of morbidity and mortality worldwide, resulting in a substantial economic and social burden. A COPD exacerbation is one of the most common causes of acute hospital admission, accounting for 70% of the total costs of COPD treatment.
What this paper contributes to our knowledge
The AECOPD-F score includes seven parameters at admission: Antonisen type of exacerbation, number of Exacerbations in the previous year, Charlson index of comorbidities, Oxygenation, Partial pressure of PaCO2 in arterial blood gases, Dyspnea according to the Borg dyspnea scale, and history of chronic respiratory Failure. These parameters were able to predict length of stay. A score ≥ 3 was associated with prolonged hospitalization.
Methods
Study Participants
In this prospective study, we enrolled 164 consecutive COPD subjects who were admitted in 2 respiratory medicine departments of 2 tertiary hospitals (Third Respiratory Medicine Department of Sismanogleio General Hospital and the Respiratory Medicine Department of Amalia Fleming General Hospital, Athens, Greece) between January 2010 and June 2012, with a diagnosis of COPD exacerbation according to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) definition.1
Inclusion criteria involved subjects with a previous diagnosis of COPD established by a respiratory physician in their records, age ≥ 40 y, current or exsmokers with smoking history ≥ 10 pack-years, and a COPD exacerbation requiring hospital admission. Subjects with a diagnosis of another acute respiratory condition (eg, pneumonia, pneumothorax, or pulmonary embolism) or a history of respiratory disorders other than COPD (eg, asthma, bronchiectasis, or pulmonary fibrosis), subjects who were unable or unwilling to cooperate with the investigators, and subjects without spirometry data were excluded from the study. Exclusion criteria also involved COPD subjects who needed invasive or noninvasive mechanical ventilation on admission because of severe respiratory acidosis. The study protocol was approved by the local ethics committees, and all participants provided written informed consent.
Study Design
Demographic data, including gender, age, body mass index, and smoking history, were recorded on admission. Exacerbation history (the number of exacerbations within the calendar year preceding the current episode), exacerbation severity according to the Anthonisen criteria,13 use of long-term oxygen therapy at home before hospitalization, and comorbid diseases were also recorded. Arterial blood gases were measured, and PaO2/FIO2 was calculated. The level of dyspnea was assessed using the modified Borg dyspnea scale on admission and before initiation of any treatment.14
Blood samples for complete blood count, routine biochemistry, and C-reactive protein were also collected. C-reactive protein was determined quantitatively using a particle-enhanced turbidimetric immunoassay test with the upper limit of normal value being 6 mg/L (Cobas Integra 400 for quantitative immunological determination of human C-reactive protein in serum and plasma, Roche Diagnostics, Rotkreuz, Switzerland).
Within 72 h of admission, all subjects underwent pulmonary function testing, including post-bronchodilation flow-volume loop, diffusing capacity for carbon monoxide, and body plethysmography evaluation of lung volumes. All tests were performed according to American Thoracic Society/European Respiratory Society guidelines.15–17
Evaluation of Comorbidities
The Charlson comorbidity index score was calculated for each subject, as this index has been shown to predict mortality.18
Medical Treatment and Discharge
All subjects were offered optimal medical treatment, including nebulized bronchodilators and steroids, systemic steroids, and antibiotics when needed according to the GOLD guidelines1 and Anthonisen criteria.13 O2 was titrated according to the results of blood gas analyses.
Decisions to discharge were based on the GOLD guidelines,1 according to which a subject could leave the hospital at the time when he was able to use inhaled bronchodilators, needed inhaled therapy with short-acting β agonists no more frequently than every 4 h, was able to walk across the room (if previously ambulatory), was able to eat and sleep without being awakened by dyspnea, had been clinically stable for 12–24 h, and understood completely the correct use of medications and when the subject and the physician were confident that the subject could manage successfully at home.1 All decisions for treatment and discharge were made by the attending physicians of the departments, and data on duration of stay were recorded on discharge.
Statistical Analysis
Categorical variables are presented as n (%), whereas numerical variables are presented as mean ± SD or median (interquartile range [IQR]). Comparisons between groups were performed using chi-square tests for categorical data, as well as unpaired t tests or Mann-Whitney U tests for normally distributed or skewed numerical data, respectively. We used the median stay (which in our case was 7 d) to categorize our subjects in 2 different groups, the group of normal stay (ie, stay < median stay recorded in the study) and the group of prolonged stay (ie, stay ≥ median stay recorded in the study). All variables that had a statistically significant difference in these 2 groups were used to create receiver operating characteristic (ROC) curves for the prediction of late discharge. The cutoff value of each parameter presenting the best combination of sensitivity and specificity was used to dichotomize the variables. The variables presenting an area under the ROC curve ≥ 0.8 were considered as possible important predictors of stay and were used in the development of a scoring system. In this scoring system, one point was given for the presence of each variable, and the total score was calculated by adding the points of each variable. This scoring system was subsequently validated in a second cohort of subjects.
Data were analyzed using SPSS 18.0 (SPSS, Chicago, Illinois), and P values < .05 were considered statistically significant.
Results
Between February 2010 and June 2012, 164 consecutive subjects were admitted to the respiratory medicine departments of Sismanogleio General Hospital and Amalia Fleming General Hospital with a diagnosis of COPD exacerbation. The demographic and functional characteristics of the 164 subjects who were included in the study are presented in Table 1. Our subjects presented a median stay of 7 d (minimum stay of 2 d and maximum stay of 30 d) and were divided in 2 groups: stay < 7 d (usual stay) and stay ≥ 7 d (prolonged stay). As shown in Table 1, the majority of demographic, functional, and laboratory characteristics of the study subjects differed between the normal-stay and prolonged-stay groups, showing that subjects who needed a prolonged stay had greater functional and biological impairment compared with the normal-stay group.
Demographic and Functional Characteristics of the Study Subjects
Parameters Related to Hospital Stay
The area under the curve of the ROC curves and the optimal cutoff point for each variable used to predict prolonged stay are shown in Table 2. Variables of the ROC curves for which the area under the curve was ≥ 0.8 were considered to play an important role in the prediction of stay. This variables were the Anthonisen type of COPD exacerbation (Anthonisen type I), the number of COPD exacerbations in the previous year (2 or more exacerbations), the Charlson comorbidity index score (score ≥ 3), PaO2/FIO2 on admission (≤ 290.48 mm Hg), PaCO2 on admission (≥ 45 mm Hg), the level of dyspnea on admission according to the Borg scale (≥ 5), and the previous history of chronic respiratory failure requiring long-term oxygen therapy.
Random Prediction of Outcome Curves of Predictors of Late Hospital Discharge
Calculation of a Simple Score for the Prediction of Stay
To predict the difference in stay by combining the aforementioned factors, we created a score that is calculated according to the presence or absence of the aforementioned 7 factors. The method of calculating the score is provided in Table 3. This score was named AECOPD-F for the initials of the variables that are included: A for Antonisen type of exacerbation, E for number of exacerbations in the previous year, C for Charlson comorbidity index score, O for oxygenation on admission (according to PaO2/FIO2), P for partial pressure of CO2 in arterial blood gases on admission, D for dyspnea according to the Borg dyspnea scale, and F for medical history of chronic respiratory failure.
Calculation of the AECOPD-F Score for Prediction of Stay
The area under the curve of the score for the prediction of prolonged hospital stay is 0.960 (95% CI 0.917–0.984), and a cutoff point of ≥ 3 predicts prolonged stay with a sensitivity of 84.5% and a specificity of 92.5%. The ROC curve of the AECOPD-F score is provided in Figure 1. The difference between subjects with a score < 3 and those with a score ≥ 3 regarding hospital days is shown in Figure 2 and was 4 (IQR 3–5) versus 9 (IQR 7–13), respectively (P < .001).
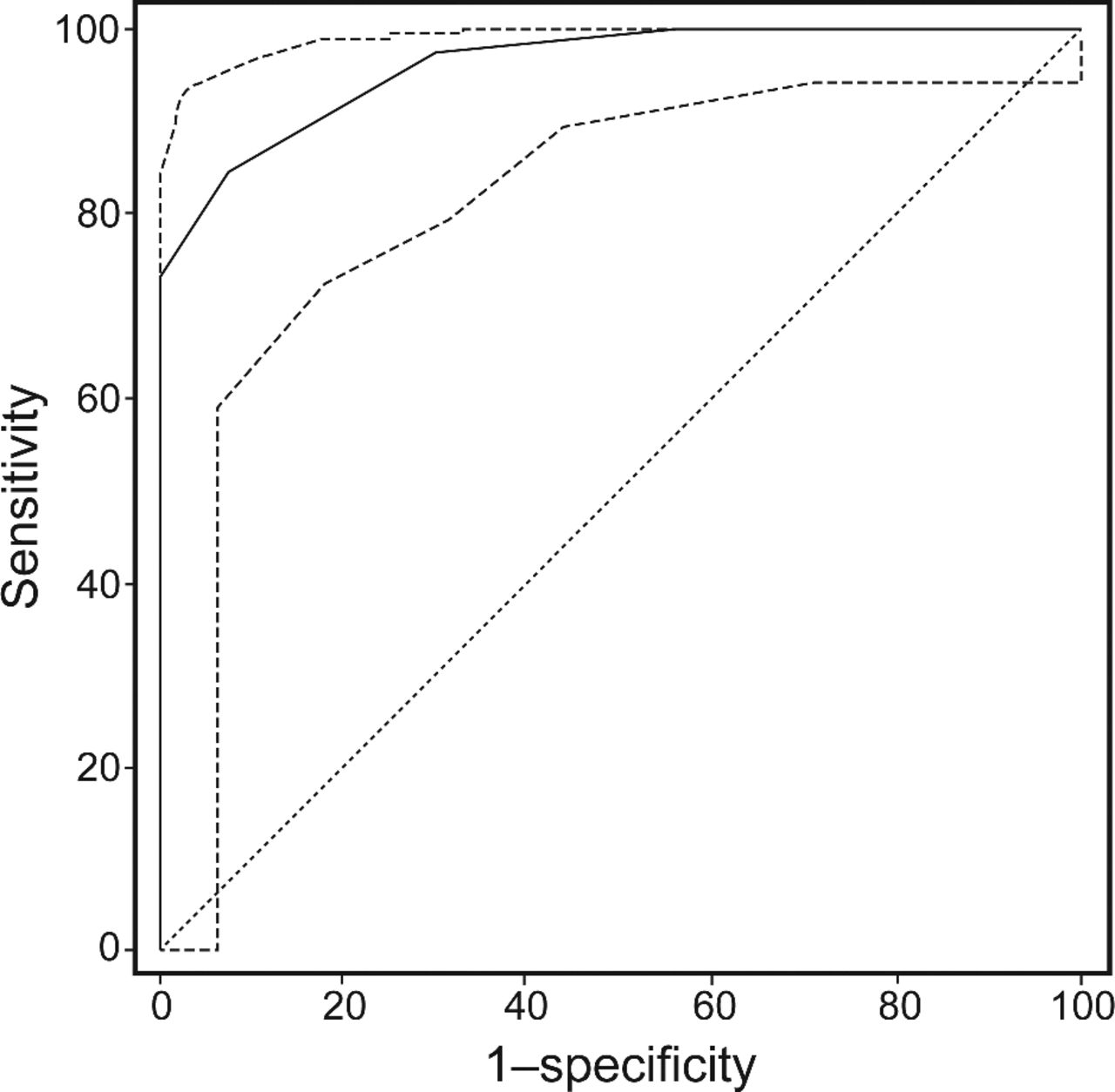
Receiver operating characteristic curve of the AECOPD-F score. Area under the curve: 0.960; standard error: 0.016; 95% CI 0.917–0.984; P < .001. A cutoff point ≥ 3 predicts prolonged stay with a sensitivity of 84.5% and a specificity of 92.5%.

Hospital stay for subjects with an AECOPD-F score of < 3 and those with a score of ≥ 3 in the original study cohort. Whiskers refer to the minimum and maximum values. Box lines represent the lower and upper quartiles. The line in the box represents the median value.
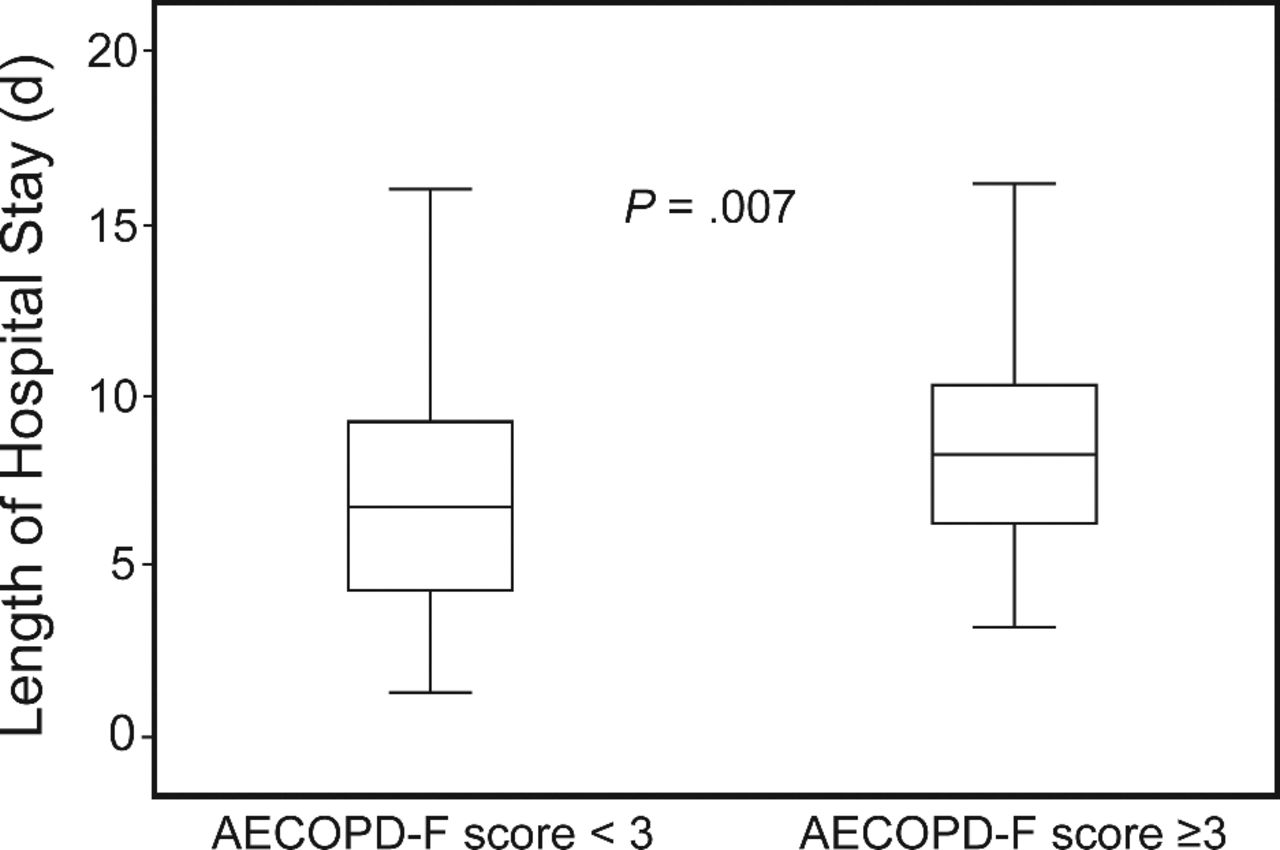
In the following months, we evaluated this score in an additional group of 88 consecutive subjects with COPD exacerbation admitted in our department. The subjects' demographic characteristics are shown in Table 4. These additional subjects were also divided in 2 groups according to the AECOPD-F score (≥ 3 and < 3), and stay was recorded. We observed that subjects with a score ≥ 3 on admission required prolonged stay compared with subjects with a score < 3 (8.0 [IQR 6.0–10.0] vs 6.5 [IQR 4.0–9.0] d, respectively, P = .007) (Fig. 3).
Demographic Characteristics of the 88 Subjects Used for the Evaluation of the AECOPD-F Score

Hospital stay for subjects with an AECOPD-F score of < 3 and those with a score of ≥ 3 in the validation group. Whiskers refer to the minimum and maximum values. Box lines represent the lower and upper quartiles. The line in the box represents the median value.
Discussion
In this study, we found that a simple clinical score (which includes 7 parameters that can be easily obtained on admission for a COPD exacerbation) can identify subjects at risk for prolonged hospitalization. People hospitalized for COPD exacerbations have a subsequent increased risk of death,3,8 suggesting the importance of factors affecting the duration of hospital stay.
Previous studies have reported a variety of factors that determine stay following a COPD exacerbation.7–11 Factors associated with longer stay include increased dyspnea,7 high breathing frequency, high PaCO2,19,20 comorbidities, advanced age, poor performance status, low FEV1,21 and cause of exacerbations (exacerbations due to infective causes were associated with longer stay).8 Furthermore, socioeconomic deprivation22 and comorbid depressive symptoms23,24 in subjects with COPD have been also related to longer hospital stay. In our study, several demographic, clinical, and laboratory parameters possibly related to stay were investigated. Although almost all of them differed significantly between the 2 groups of subjects (normal-stay and prolonged-stay groups), only 7 parameters were finally found to be significant in the ROC analysis and were included in the prediction score.
Data on the impact of age on stay in subjects hospitalized for a COPD exacerbation are controversial. Although there is evidence that age is an independent predictor of stay,8,21,25 for subjects older than 80 y requiring longer hospitalizations compared with those 40–59 y old,8 it has been suggested that stay time was probably affected by the presence of multiple comorbidities, living alone, and the use of respiratory depressant drugs rather than age.26 In agreement with the aforementioned study, age was not a predictor of late discharge in our group of subjects.
Anthonisen-type I/II exacerbation was an independent predictor of late recovery in out-patients with COPD exacerbation.10 To our knowledge, there are no relevant data about the impact of Anthonisen-type exacerbation in hospitalized COPD subjects. Our data showed that Anthonisen-type I exacerbation was a strong predictor of stay.
The most accurate method to identify the frequent exacerbators in clinical practice is examination of previous exacerbation history. In a study of a large cohort of out-patients with COPD exacerbation,10 history of frequent exacerbations was one of the main factors associated with late recovery (≥ 8 d). There are no studies examining the influence of previous hospitalizations due to a COPD exacerbation on stay. According to our data, 2 or more exacerbations in the year before current admission could predict prolonged stay.
Comorbidities are among the most frequently identified prognostic factors of in-hospital outcome27 and were independent predictors of stay in previous studies.8,9,20,28,29 It is reasonable to expect stay to be longer in subjects with multiple underlying health conditions. A Charlson comorbidity index score ≥ 3 in our study identified subjects with prolonged stay.
Low PaO2/FIO230 and preadmission long-term oxygen therapy11 independently predict 6-month mortality and high readmission rates. However, none of these parameters have been studied in relation to stay. These indices probably reflect the severity of both the acute illness and the underlying condition; thus, we hypothesized that they could also predict the duration of hospital stay. Our data confirmed that PaO2/FIO2 ≤ 290 mm Hg on admission could predict prolonged stay. Chronic respiratory failure with long-term oxygen therapy could also predict increased hospital stay. In previous studies,19,20 high PaCO2 levels were associated with the need for longer hospital stay. Our results are in concordance with these previous data showing that PaCO2 ≥ 45 mm Hg on admission was correlated with longer stay.
Increased breathlessness is the principal symptom of a COPD exacerbation. There is only one study evaluating the impact of dyspnea on stay.7 However, in the aforementioned study, dyspnea was measured according to the Medical Research Council scale. We believe that the modified Borg scale is more accurate in reflecting progressive breathlessness occurring during the time course of a COPD exacerbation. The modified Borg dyspnea scale consists of 10 statements with small differences in perception of symptoms from level to level, whereas the Medical Research Council scale comprises a 5-statement scale with larger differences in perceived symptoms between levels. Moreover, the Medical Research Council scale represents more of an exercise tolerance than a dyspnea assessment tool. In our study, a Borg score on admission of ≥ 5 was the strongest predictor of stay, and this further supports the central role of dyspnea in the evaluation of subjects on admission for a COPD exacerbation.
We noted certain limitations of our study. First, subjects with severe respiratory acidosis (pH < 7.30) who were candidates for noninvasive mechanical ventilation were not included in the study. It would be useful for our score to be applied to subjects with COPD exacerbation who need noninvasive mechanical ventilation, as it seems possible that it could also be capable of predicting stay in this group of subjects. Second, data about important covariates that previous studies have shown to determine stay (eg, socioeconomic status or anxiety and depression) were not evaluated in this study. Finally, in our study, the number of female subjects was lower compared with that of male subjects, and the AECOPD-F score has not been validated separately in male and female subjects. The difference in the number of male and female subjects probably reflects the different incidence of COPD between genders in our Greek population.31 Despite the above limitations, our study described a simple prediction score of hospitalization duration in subjects with COPD exacerbations, and this score was further validated in a second cohort of subjects from our hospital. Our data could be applied to subjects managed by assisted discharge schemes, which many countries now use. Although many studies have shown that the supported discharge programs allow a significant reduction in stay of subjects hospitalized for COPD and reduce the utilization of hospital resources without increasing the risk of hospital readmissions, subjects' inclusion criteria for early discharge were not clearly defined.32–35 The AECOPD-F score could be used to identify subjects who could be discharged earlier and those who may need more prolonged hospitalization and/or extended support at home. The implementation of this score in the planning of the management of such subjects could be evaluated in a future study.
Conclusions
Our study detected predictors of stay from a large number of evaluated parameters and provided a simple clinical score implementing 7 parameters easily obtained on subject admission. The AECOPD-F score can accurately predict prolonged hospitalization for a COPD exacerbation, and the implementation of this score in clinical practice could be very useful in the discharge planning of such subjects. Given the substantial economic consequences of stay on hospital costs, this result could help improve the management of individual COPD subjects and contribute to the optimization of health care resource utilization.
Footnotes
- Correspondence: Filia Diamantea MD, Third Respiratory Medicine Department, Sismanogleio General Hospital, Sismanogleiou 1, 15126 Marousi Athens, Greece. E-mail: fdiamantea2001{at}yahoo.co.uk.
This research was supported by the Hellenic Thoracic Society. The authors have reported no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}