

Abstract
INTRODUCTION: Delivering heated and humidified medical gas at 20–60 L/min, high-flow nasal cannula (HFNC) creates low levels of PEEP and ameliorates respiratory mechanics. It has become a common therapy for patients with respiratory failure. However, independent measurement of heat and humidity during HFNC and comparison of HFNC devices are lacking.
METHODS: We evaluated 2 HFNC (Airvo 2 and Optiflow system) devices. Each HFNC was connected to simulated external nares using the manufacturer's standard circuit. The Airvo 2 outlet-chamber temperature was set at 37°C. The Optiflow system incorporated an O2/air blender and a heated humidifier, which was set at 40°C/−3. For both systems, HFNC flow was tested at 20, 40, and 50 L/min. Simulating spontaneous breathing using a mechanical ventilator and TTL test lung, we tested tidal volumes (VT) of 300, 500, and 700 mL, and breathing frequencies of 10 and 20 breaths/min. The TTL was connected to the simulated external nares with a standard ventilator circuit. To prevent condensation, the circuit was placed in an incubator maintained at 37°C. Small, medium, and large nasal prongs were tested. Absolute humidity (AH) of inspired gas was measured at the simulated external nares.
RESULTS: At 20, 40, and 50 L/min of flow, respective AH values for the Airvo 2 were 35.3 ± 2.0, 37.1 ± 2.2, and 37.6 ± 2.1 mg/L, and for the Optiflow system, 33.1 ± 1.5, 35.9 ± 1.7, and 36.2 ± 1.8 mg/L. AH was lower at 20 L/min of HFNC flow than at 40 and 50 L/min (P < .01). While AH remained constant at 40 and 50 L/min, at 20 L/min of HFNC flow, AH decreased as VT increased for both devices.
CONCLUSIONS: During bench use of HFNC, AH increased with increasing HFNC flow. When the inspiratory flow of spontaneous breathing exceeded the HFNC flow, AH was influenced by VT. At all experimental settings, AH remained > 30 mg/L.
Introduction
Oxygen therapy is the first-line treatment for patients who suffer organ dysfunction,1–3 and nasal cannula is commonly used for low-flow oxygen delivery. This means of delivery is typically used for stable patients, for whom the FIO2 may vary according to breathing pattern. Oxygen flow is usually 1–6 L/min. Administration of > 6 L/min does not greatly improve FIO2 and leads to nasal dryness, bleeding, and other discomfort to the patient.4 A simple oxygen mask is used to deliver higher flow of 5–12 L/min. When it does not meet patient demand, room air is drawn around the mask. FIO2 varies with mask fit, delivered flow, and patient minute volume. When flow is low, carbon dioxide is rebreathed.
In ICUs, high-flow nasal cannula (HFNC) therapy has become common for patients with unstable respiratory function.5 HFNC can deliver up to 60 L/min of heated and humidified medical gas, and FIO2 can be adjusted using a wide-bore nasal cannula. HFNC therapy is considered to create low levels of PEEP6,7 and to reduce dead space. Effects on oxygenation, carbon dioxide (CO2) elimination, and respiratory mechanics have been reported,8–11 No independent measurements on heat and humidity delivered during HFNC have been published. In the field of humidification, it is important to provide independent measurements of device performances, as discrepancies may exist between data provided by the manufacturers and bedside clinical data.12 We carried out this bench study to evaluate humidification performance of HFNC devices under various spontaneous breathing (SB) patterns and with different prong sizes.
QUICK LOOK
Current knowledge
Heated and humidified high-flow oxygen via nasal cannula improves oxygenation by meeting patient inspiratory flow demand and providing a small positive airway pressures. Minute ventilation requirements are also reduced by washout of the upper airway anatomic dead space. Optimal heat and humidity levels are not known.
What this paper contributes to our knowledge
A bench study of two heated and humidified, high-flow nasal cannula systems demonstrated that an absolute humidity of > 30 mg of H2O/L was provided with both systems between 20 and 50 L/min. Absolute humidity decreased as tidal volume increased from 300 to 700 mL.
Methods
We evaluated two types of HFNC (Airvo 2 and Optiflow systems, Fisher & Paykel Healthcare, Auckland, New Zealand). In the Airvo 2, chamber-outlet temperature was set at 37°C. The Optiflow system incorporated an O2/air blender and a heated humidifier (MR850, Fisher & Paykel Healthcare). The MR850 was set in invasive mode (40°C/−3). For both systems, we tested HFNC flow of 20, 40, and 50 L/min. FIO2 was set at 0.21 for both devices. SB was simulated using a mechanical ventilator (Puritan-Bennett 840, Covidien, Carlsbad, California) and TTL test lung (TTL model 1601, Michigan Instruments, Grand Rapids, Michigan). To simulate SB, the muscle and lung compartment of the test lung were connected, after which the Puritan-Bennett 840 inflated the muscle compartment, and the lung compartment inspired medical gas delivered via HFNC and ambient air. One-way valves prevented mixing of inspired and expired gases. Compliance of the TTL test lung was 0.05 L/cm H2O, and resistance was 5 cm of H2O/L/s. We tested tidal volumes (VT) of 300, 500, and 700 mL, and breathing frequencies of 10 and 20 breaths/min. Inspiratory time was set at 1 s with square waveform, and it resulted in 18, 30, and 42 L/min of SB inspiratory flow. Before experimental testing, a ventilator self-test was performed.
HFNC creates PEEP and increases residual volume in the lung compartment. We measured the end-expiratory pressure of the lung compartment and, to keep the residual volume of the muscle compartment at the same level as the lung compartment, set corresponding levels of PEEP on the Puritan-Bennett 840. To confirm VT delivered to the lung compartment, flow to the lung compartment was measured using a pneumotachometer (4700 series, 0–160 L/min, Hans Rudolph, Inc, Shawnee, Kansas) with a differential pressure transducer (TP-602T, ± 5 cm H2O, Nihon Kohden, Tokyo, Japan).
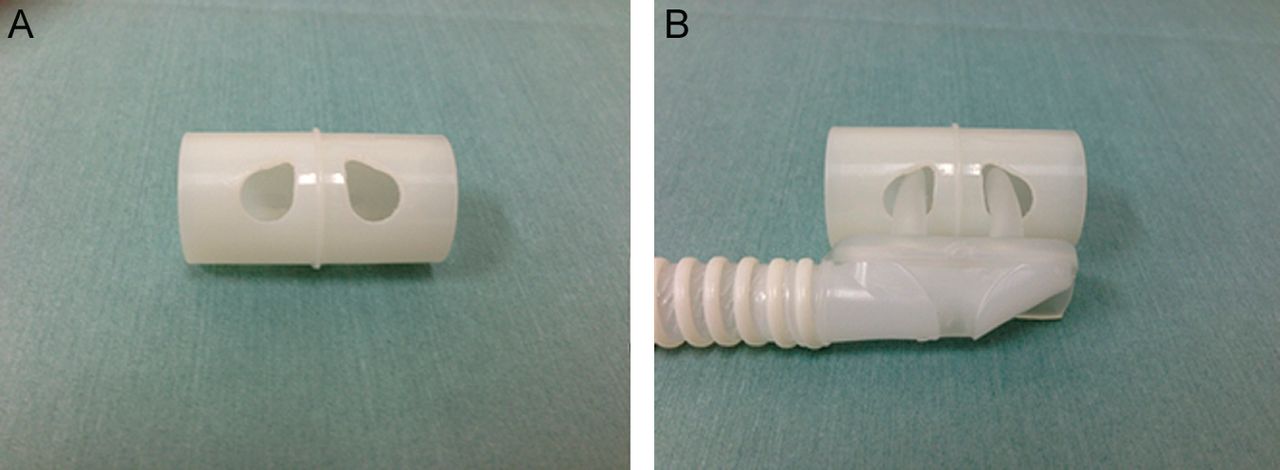
We made two holes in a polyvinyl chloride cylinder to simulate external nares (Fig. 1). Into these holes, we inserted and tested small, medium, and large nasal prongs: OPT842, OPT844, and OPT846 with the Airvo 2; and OPT542, OPT544, and OPT546 with the Optiflow. The nasal prongs were connected to the manufacturer's standard circuit (900PT501 for the Airvo 2 and RT202 for the Optiflow). The external nares were connected to the TTL test lung via a standard ventilator circuit (Smoothbore tube 5000000, Intersurgical, Berkshire, United Kingdom). To prevent condensation, the circuit was placed in an incubator (V-2100G, No. 8090508, Atom Medical, Tokyo, Japan) in which the temperature was maintained at 37°C. All experiments were performed in an air-conditioned room. See Figure 2 for experimental setup.

Photographs of external nares. A: to simulate external nares, two holes were opened in a polyvinyl chloride cylinder. B: medium prongs attached to high-flow nasal cannula inserted into the simulated external nares. During the experiment, prongs were secured on the nares using tape.
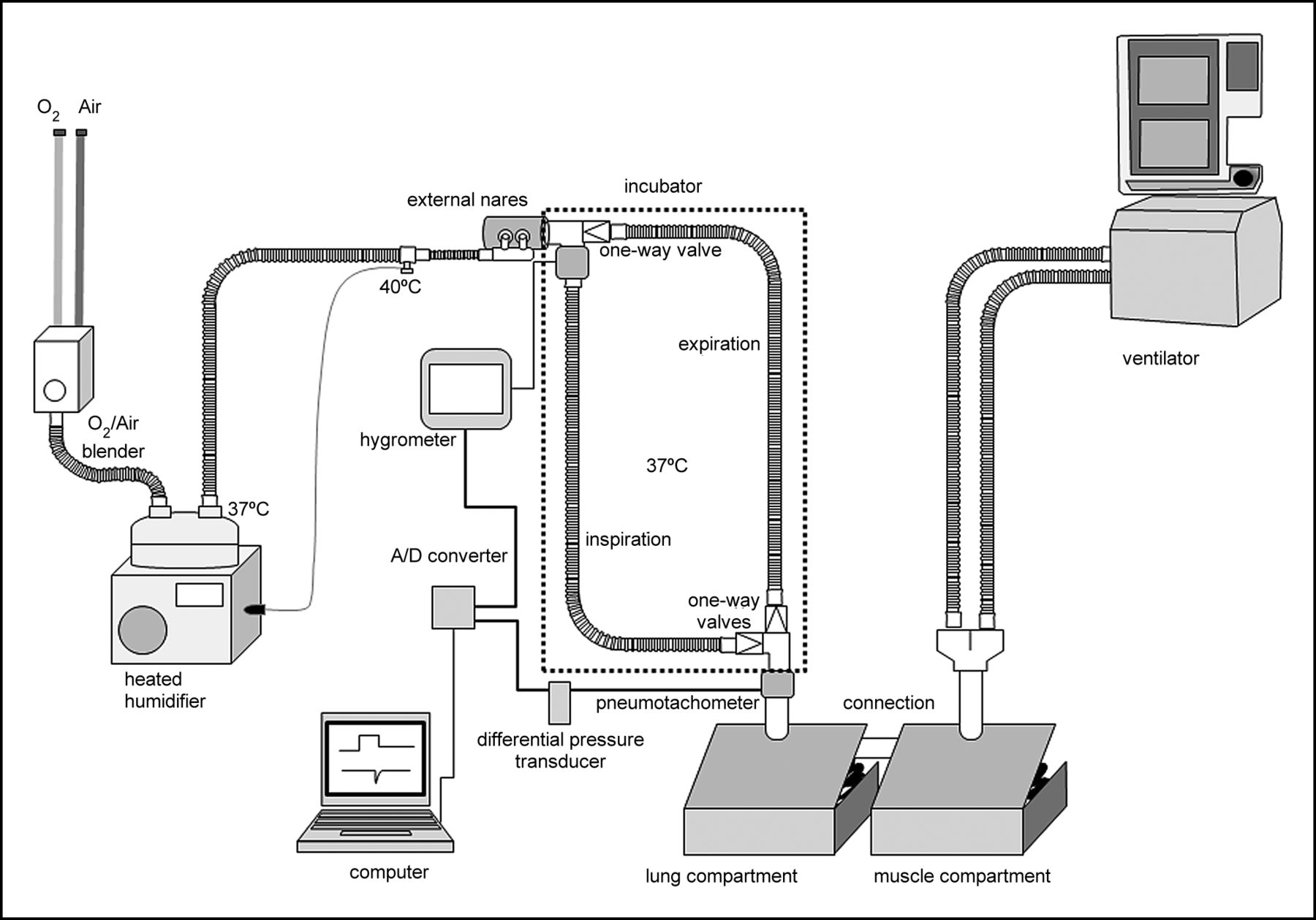
A ventilator and TTL test lung were used to simulate spontaneous breathing. When a ventilator sends gas to the muscle compartment, the lung compartment attached to it starts inspiration. During simulated inspiration, ambient air is drawn into the lung compartment through the hygrometer. When the expiratory phase starts, gas in the lung compartment is expired to ambient space. We modeled external nares, which were connected to the simulated trachea. Each high-flow nasal cannula was connected to the simulated external nares using the manufacturer's standard circuit. The Airvo 2 was set at 37°C, and the Optiflow was set to 40°C at the distal end of the breathing circuit and 37°C at the chamber outlet. The simulated trachea was placed in an incubator. To prevent condensation, the internal temperature of the incubator was maintained at 37°C. One-way valves were connected on the limb of the simulated trachea to separate inspiratory and expiratory gases.
After each experimental setting was changed, we allowed at least 30 min for stabilization. Temperature, relative humidity, and absolute humidity (AH) of inspired gas downstream of the external nares were measured using a moisture sensor (Moiscope, Senko Medical, Tokyo, Japan; capacitance type, response time 3 s in the range 40–100%). The hygrometer was calibrated at two points by using a cooler/heater water source (HHC-51, Senko Medical). Because condensation on sensor surfaces compromises the accuracy of humidity measurement, the sensor was withdrawn from the circuit during stabilization periods; after insertion for measurement, we monitored temperature, relative humidity, and AH for 10 min, and after confirming the constancy of the values, we recorded temperature, relative humidity, and AH for the final 5 min. All signals were processed through an analog/digital converter and saved on a computer at 50 Hz/channel using data acquisition software (WinDaq, Dataq Instruments, Akron, Ohio). For each experimental setting, we measured temperature and AH for 5 breaths. The results were expressed as mean ± SD.
Analysis of variance was performed using repeated measures analysis of variance. All statistical tests were two-sided, and P < .01 was considered statistically significant. All statistical analysis was performed using commercial software (SPSS 11.01, SPSS, Chicago, Illinois).
Results
AH was 36.5 ± 2.3 mg/L with the Airvo 2, and 35.1 ± 2.2 mg/L with the Optiflow system (P < .01) at 20, 40, and 50 L/min, respectively; AH with the Airvo 2 was 35.2 ± 2.6, 36.9 ± 2.2, and 37.4 ± 2.1 mg/L; and with the Optiflow, it was 33.1 ± 1.5, 35.9 ± 1.7, and 36.2 ± 1.7 mg/L (Fig. 3). With both systems, AH was significantly higher at 40 and 50 L/min than at 20 L/min (P < .01). AH remained the same at 40 and 50 L/min.

Effects of flow and tidal volume (VT) on absolute humidity (AH). At high-flow nasal cannula (HFNC) flow of 20 L/min, when VT increased from 300 to 700 mL, AH decreased; at HFNC flow of 40 and 50 L/min, AH did not vary according to VT. A: Airvo 2 HFNC. B: OptiFlow HFNC.
At 300, 500, and 700 mL of VT respectively, AH with the Airvo 2 was 35.6 ± 1.9, 36.9 ± 2.0, and 37.1 ± 2.6 mg/L and, with the Optiflow, 34.7 ± 1.9, 35.3 ± 1.9, and 35.3 ± 2.7 mg/L. While VT affected AH at 20 L/min HFNC flow (Fig. 3), at 40 and 50 L/min of HFNC flow, AH remained the same at 300, 500, and 700 mL of VT. As breathing frequencies increased, AH increased (P < .01). Prong size did not affect humidification for both devices.
Throughout the protocol, AH and the temperature of ambient air remained at 12.9 ± 1.5 mg/L and 25.6 ± 0.5°C.
Discussion
In this first study to evaluate humidification performance under various SB patterns during HFNC, we found AH was > 30 mg/L at all tested settings.
For face mask administration, Chanques et al13 previously reported median AH was 29.7 (24.4–30.6) mg/L; AH in the present study was higher. In their study, median flow was 7.8 (5.1–10.9) L/min, which was less than HFNC flow in the present study. In our experiment, we tested HFNC flow at 20, 40, and 50 L/min. Assuming that all delivered gas is inspired, humidity would depend on the inspiratory flow of SB and HFNC flow. When inspiratory flow is less than HFNC flow, patients would inspire only the gas delivered via HFNC, and humidification would depend almost entirely on the humidity of delivered gas. If inspiratory flow is greater than HFNC flow, patients would inspire both delivered gas and room air. SB inspiratory flow, respectively, was 18, 30, and 42 L/min at VT of 300, 500, and 700 mL. Consequently, when HFNC flow is 20 L/min, inspiratory flow would be greater than HFNC flow at VT 500 and 700 mL. We did, in fact, find with 20 L/min of HFNC flow that AH was lower at 500 and 700 mL of VT than at 300 mL of VT. Meanwhile, with 40 and 50 L/min of HFNC, humidification did not differ according to VT, because the flow was similar to or greater than SB inspiratory flow. Chikata et al,14 simulating high-flow oxygen for tracheostomized patients in a bench study, reported findings similar to the present study; AH decreases as VT increases.
It is also necessary to ensure adequate humidification of the gas delivered via HFNC. Chanques et al13 compared bubble and heated humidifiers. With a heated humidifier, AH was 2 times higher than with a bubble humidifier. That study also used an MR850, which comprises a humidification chamber and a heated-wire circuit with 22 mm diameter tubing; the heated wire was set to maintain proximal temperature at 34°C and chamber temperature at 31°C. Using the same heated humidifier for the Optiflow, our proximal temperature setting was 40°C and chamber setting was 37°C. These setting differences enabled higher inspiratory AH in the present study. For the Airvo 2, we set only the chamber temperature, which was 37°C. The Airvo 2 servo-controls the proximal temperature at approximately 40°C. In this way we obtained similar, higher than previously reported, AH values with the Airvo 2 and with the Optiflow.
AH was higher with the Airvo 2 than with the Optiflow. As described above, temperature control mechanisms differs between the devices, and it may cause higher AH with the Airvo 2. In addition, Airvo 2 measures ambient temperature because it uses ambient air, while the manufacturer does not provide an algorithm to control gas temperature by measuring ambient temperature. Another possibility was volume of the water chamber. Airvo 2 contains a larger volume of water, and this means more heat quantity.
Aside from being a bench study, our experiment was limited in other ways. For example, we tested only two HFNC devices, both from the same manufacturer, because they are the only ones currently available in Japan. We chose 20, 40, and 50 L/min of HFNC flow because they are in the range commonly selected when using these devices. Oto et al have reported on humidification and mouth dryness during noninvasive ventilation.15 Measuring AH inside face masks during noninvasive ventilation, they found AH varied in the range from 23.1 to 33.3 mg of H2O/L. If patients breathe through the mouth, they inspire more ambient air. Moreover, the VT of human beings varies,16 and AH might even vary breath-by-breath in clinical patients. In HFNC therapy, flow is delivered at a constant rate, and AH of delivered gas might be more stable than with noninvasive ventilation.
We cannot assume, however, that HFNC always provides more stable humidification; results from our bench test cannot be directly applied to clinical settings. We firmly fixed the nasal prongs into the simulated external nares. In real life, the prongs usually move frequently. The present study was done only at FIO2 = 0.21. Optiflow uses only medical gases, air and oxygen are mixed upstream of the water chamber, and AH is not influenced by FIO2. In contrast, Airvo 2 uses ambient air, and dry oxygen is added upstream of the water chamber. Under high FIO2, AH could decrease. We set the invasive mode of MR850 with the Optiflow. Vapor output is different between the invasive and noninvasive modes, and AH must be lower in noninvasive mode.
Conclusions
We bench-tested inspiratory gas humidification during HFNC therapies with a simulated SB. At all experimental settings, AH was > 30 mg/L. During bench use of HFNC, AH increased with increasing HFNC flow. Although SB inspiratory flow exceeded HFNC flow, AH was influenced by VT; humidification is sufficient for patients with SB at 20–50 L/min of HFNC flow with the devices investigated in the present study.
Footnotes
- Correspondence: Masaji Nishimura MD, Department of Emergency and Critical Care Medicine, University of Tokushima Graduate School, 3-18-15 Kuramoto, Tokushima, Japan 770-8503. E-mail: nmasaji{at}tokushima-u.ac.jp.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}