

Abstract
Capnography is a graphic representation of the carbon dioxide concentration in the airways plotted against time. We report an unusual biphasic-shaped capnogram in a single-lung transplant recipient. In keeping with the only 2 prior reports of which we are aware, we ascribe the unusual biphasic pattern to differential emptying of the native and transplanted lungs. This experience reminds respiratory clinicians of the value of capnometry as a monitoring tool and hopefully will heighten awareness regarding the diagnostic value of usual and unusual capnographic patterns.
Introduction
Capnography is a graphic representation of the carbon dioxide concentration in the airways plotted against time. Capnography has become a standard of care in monitoring patients who are intubated and mechanically ventilated, as it allows approximation of the patient's PaCO2. The configuration of the capnogram has been reported to be diagnostically helpful, for example, the shape may have a delayed rise as in COPD or a dip that has been ascribed to the recovery of diaphragmatic function following paralysis. Continuous capnography during intubation helps in confirming tracheal intubation, monitoring the integrity of the endotracheal tube and ventilator circuit, assisting with the titration of mechanical ventilatory support, assessing pulmonary capillary blood flow, and monitoring for extubation readiness.1–3
Case Report
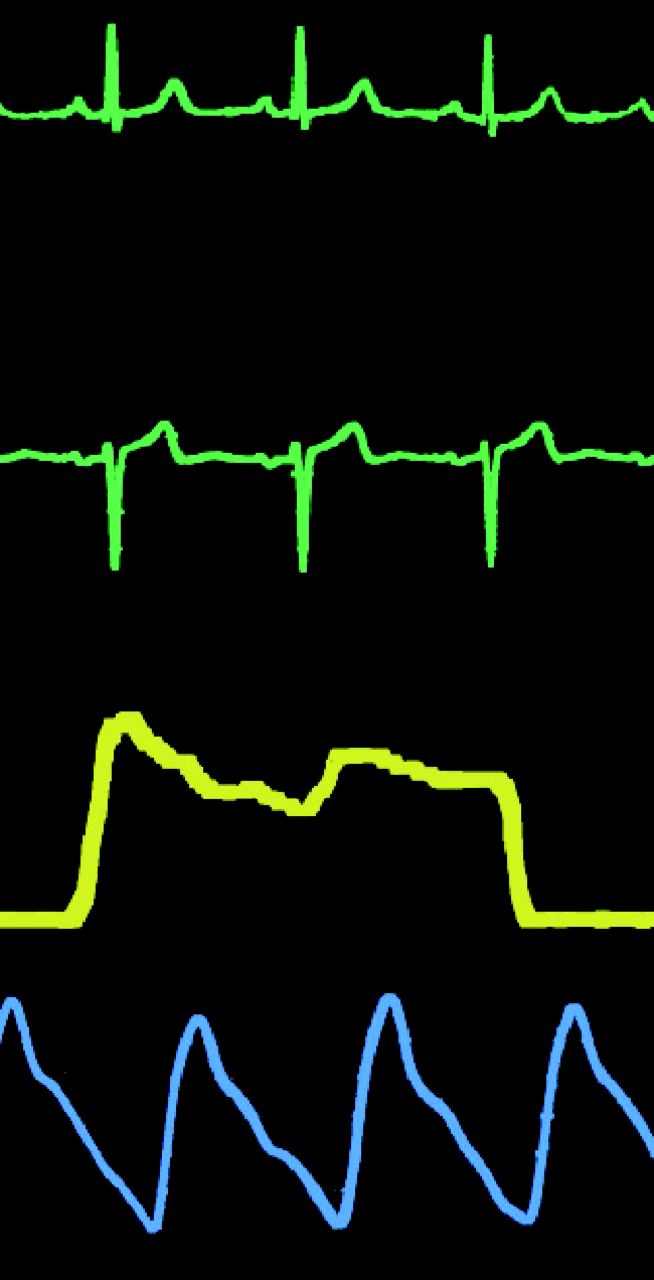
This report describes an unusual biphasic-shaped capnogram in a single-lung transplant recipient. The patient was a 68-y-old male, 84 pack-year former smoker who underwent a right single-lung transplantation for very severe COPD (FEV1 0.46 L [15% predicted], FVC 1.38 L [33% predicted], FEV1/FVC 0.33). A quantitative ventilation-perfusion scan performed prior to surgery showed right-lung and left-lung perfusion at 43.5% and 56.5%, respectively. The patient was initially orally intubated for surgery and later underwent tracheostomy tube placement when the need for prolonged mechanical ventilation became clear. Post-transplant chest radiography showed marked hyperinflation of the native lung with encroachment into the contralateral transplanted chest. The postoperative course was complicated by multiple infections (including multidrug-resistant Pseudomonas and Mycobacterium avium-intracellulare), repeated inability to wean from mechanical ventilation (with the longest duration of spontaneous breathing being 15 h despite maneuvers like bronchoscopic decompression and transient placement of bronchial blockers in the main bronchus of the native lung), and ultimately long-term ventilator dependence with a 10-month course in the weaning unit to date. The patient was mechanically ventilated with various modes, including pressure support (from 8 to 15 cm H2O) and pressure control modes, with an FIO2 of 0.35, inspiratory pressure of 16, breathing frequency of 24 breaths/min, PEEP of 5 cm H2O, inspiratory time of 0.80 s, and an inspiratory time/expiratory time of 1:2.1. Exhaled tidal volume was noted to be 470 mL. Monitoring with a mainstream continuous capnometer (Solar 8000i V5 with single-parameter module, GE Healthcare, Madison, Wisconsin) showed end-tidal CO2 values in the mid 30 to low 40 mm Hg range but an unusual biphasic capnogram (Fig. 1). This biphasic pattern differs from the usual pattern, in which the value of the exhaled CO2 progressively rises over time as the patient exhales and oscillates at the same frequency as the patient's breathing frequency.4

Telemetry showing biphasic capnograph (yellow), pulse oximetry (blue), and electrocardiograph (green) after single-lung transplantation.
Discussion
In keeping with the 2 earlier reports of biphasic capnograms in the setting of prior single-lung transplantation,5,6 we suspect that this unusual biphasic pattern reflects differential ventilation of the 2 lungs, with the initial peak reflecting allograft emptying (given the relatively preserved compliance and airway resistance of the transplanted lung) and the delayed peak representing the slowed emptying of the emphysematous native lung. The differential ventilation is a reflection of differences in ventilation/perfusion ratios between the lungs. Notably, in contrast to the report by Srinivasa et al,6 this pattern of the capnogram seemed consistent and persistent over the patient's protracted course in the weaning unit and did not vary over short time intervals.
Abnormal configurations of the capnogram reflecting presumed differential lung emptying have been described previously in the setting of kyphoscoliosis7 and right mainstem bronchial intubation,8 neither of which was present in our patient. Also, the configuration of our patient's capnogram is different from the so-called curare cleft, which has been ascribed to the recovery of diaphragmatic function and spontaneous breathing following fading pharmacologic paralysis.
In summary, we report what is, to our knowledge, the third reported experience of a biphasic capnogram in a patient who had undergone single-lung transplantation. Clinicians should be vigilant about the presence and diagnostic implications of abnormal capnographic shapes and should recognize the biphasic capnogram as a manifestation of differential lung ventilation, which can occur following single-lung transplantation. To the extent that this finding is uniquely identifiable by capnography, this experience lends support to more widespread use of capnometry in managing mechanically ventilated patients.
Footnotes
- Correspondence: Hardeep S Rai MD, Respiratory Institute, Cleveland Clinic, A-90, Cleveland, OH 44195. E-mail: raih{at}ccf.org.
The authors have disclosed no conflicts of interest.
- Copyright © 2014 by Daedalus Enterprises





{kind=link}