

Abstract
BACKGROUND: For early detection of respiratory and hemodynamic changes during anesthesia, continuous end-tidal carbon dioxide concentration (PETCO2) is monitored by capnometry. However, the accuracy of CO2 monitoring during spontaneous breathing in extubated patients remains undetermined. Therefore, we aimed to compare PETCO2 measured by capnometry using an oxygen mask with a carbon dioxide sampling port (capnometry-type oxygen mask) and PCO2 in extubated subjects who had undergone abdominal surgery. Furthermore, we investigated whether spontaneous deep breathing affected dissociation between PaCO2 and PETCO2.
METHODS: Adult post-abdominal surgery subjects admitted to the ICU were enrolled in this study. After extubation, oxygen was supplied at 6 L/min using the capnometry-type oxygen mask. After 30 min of oxygen supply, PaCO2 blood gas analysis was performed, and PETCO2 was measured under resting and deep-breathing conditions. For both resting and deep-breathing conditions, the correlation between PaCO2 and PETCO2 was analyzed. Furthermore, bias, precision, and limits of agreement were calculated using the Bland-Altman method.
RESULTS: Twenty-five subjects (15 men, 10 women) with a mean age of 62 y (interquartile range of 57–76 y) and body mass index of 20–24 kg/m2 were studied. The correlation (r) between PaCO2 and PETCO2 under resting and deep-breathing conditions was 0.50 and 0.56, respectively. Compared with PaCO2, the bias and limits of agreement were −12.6 (−20.6 to −4.6) for resting PETCO2 and −9.1 (−16.0 to −2.1) for deep-breathing PETCO2. The association between PaCO2 and deep-breathing PETCO2 was significantly smaller compared with resting PETCO2 (P = .002).
CONCLUSIONS: It is possible to measure the PETCO2 under varying breathing conditions with the capnometry-type oxygen mask in subjects receiving oxygen supplementation after extubation following upper abdominal surgery to determine whether they are properly ventilating. (ClinicalTrials.gov registration UMIN000011925.)
Introduction
Compared with other surgeries, the incidence of pulmonary complications is higher after upper abdominal or chest surgery because both surgeries involve severe and prolonged alteration of pulmonary mechanics.1 After abdominal operations, active collapse of the lungs along with hypoventilation is the major cause of postoperative hypoxia and pulmonary complications.2,3 Furthermore, surgical trauma after thoracic and abdominal surgery affects respiratory muscles, leading to postoperative hypoxia and pulmonary complications.4 Three factors produce respiratory muscle dysfunction after abdominal surgery. First, muscle disruption by surgical incision impairs effectiveness of respiratory muscles. Second, postoperative pain may cause voluntary limitation of respiratory motion. Third, surgical trauma stimulates central nervous system reflexes mediated by both visceral and somatic nerves that produce reflex inhibition of the phrenic and other nerves, innervating respiratory muscles.4 Therefore, monitoring respiratory function in patients who have undergone abdominal surgery is one of the essential assessments carried out in ICUs.
Capnography is an increasingly popular procedure; its widespread clinical use may improve patient care and safety. Assessment of the extrapolated end-tidal carbon dioxide concentration (PETCO2) is one of the most useful aspects of capnography.5 The levels of alveolar (PETCO2) and arterial (PaCO2) CO2 are similar in healthy subjects (eg, difference of < 5 mm Hg). Therefore, in subjects with normal dead space, it is safe to use PETCO2 as a substitute for PaCO2.6–8 However, in patients who have undergone abdominal surgery, the levels of alveolar and arterial CO2 are altered due to changes in respiratory and hemodynamic conditions.
Physiological dead space is the sum of anatomical and alveolar dead space and is defined as the sum of all parts of the tidal volume that do not participate in gas exchange.9 In healthy subjects, physiological dead space is small and inconsiderable; however, in postoperative patients, respiratory mechanics are altered, and several changes lead to increased physiological dead space. The functional residual capacity continuously decreases after an operation, usually reaching its lowest value 1–2 d after the operation, before slowly returning to normal values within 1 week.10
The most common problem during surgery is ventilation/perfusion mismatching that leads to impaired gas exchange, which persists during the postoperative period. The PETCO2 is continuously monitored by capnometry for early detection of respiratory or hemodynamic changes during anesthesia. However, in extubated patients, PETCO2 monitoring requires a device that can draw a continuous gas sample for spectrographic measurements with the capnometer.11–13 Furthermore, the PETCO2 wave is normally unstable in non-intubated patients because the oxygen supply system is not closed compared with the oxygen system with mechanical ventilation using an endotracheal tube during anesthesia.
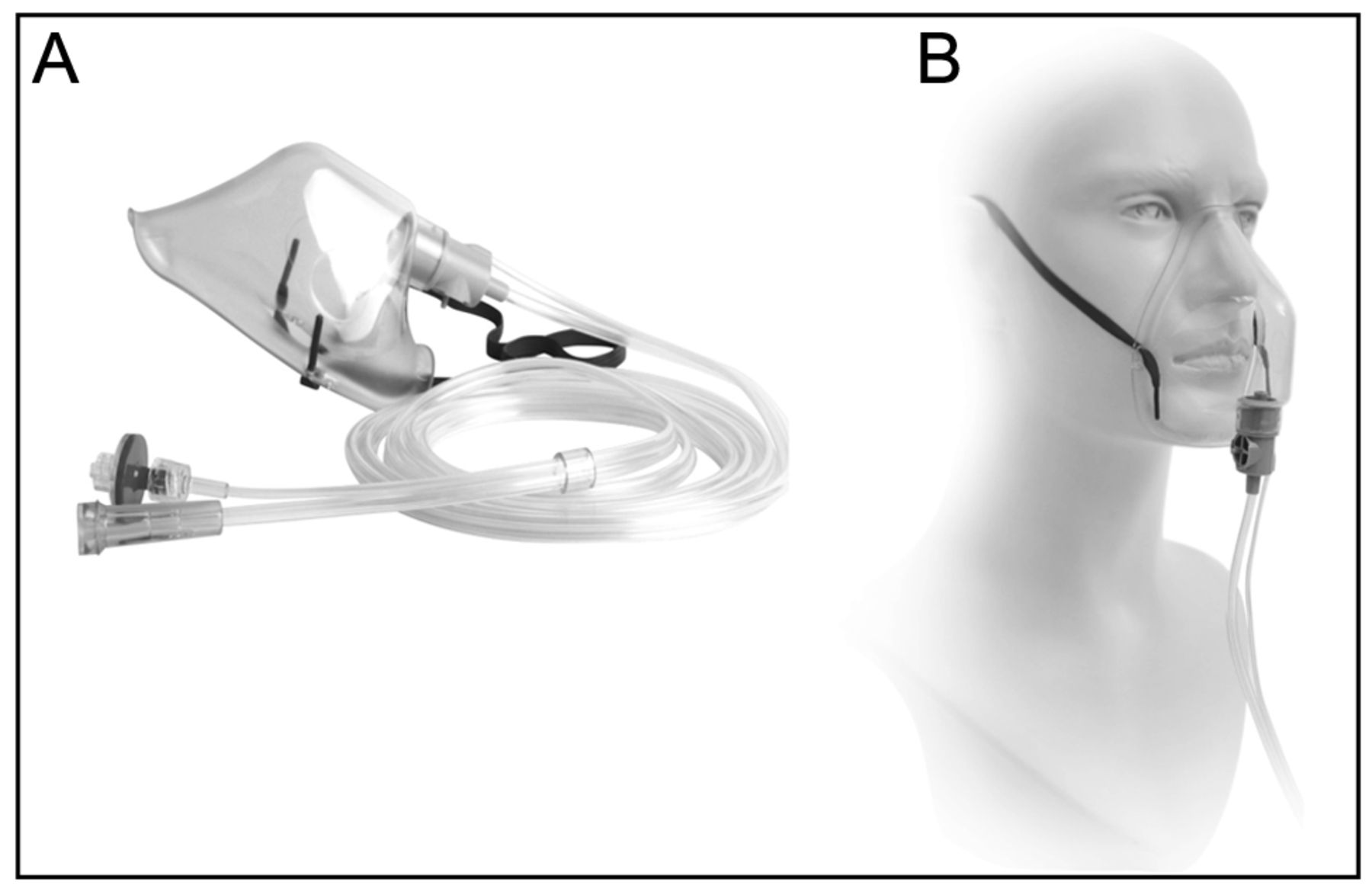
The newly developed capnometry-type oxygen mask (Japan Medical Next, Tokyo, Japan) has a PETCO2 sampling line for use in spontaneously breathing patients (Fig. 1). Previous studies have shown that this device is useful for monitoring respiration in extubated subjects.14,15 However, dissociation between PETCO2 and PaCO2 has not been investigated, and the precision of CO2 monitoring by oxygen mask capnometry remains unclear.

A: Capnometry-type oxygen mask. This mask has a CO2 sampling port next to the oxygen supply port. B: A capnometry-type oxygen mask is fitted like a normal face mask and can supply normal oxygen flow. Expiratory flow is drawn into the sidestream for measurement of end-tidal carbon dioxide concentration.
The purpose of this study was to compare PETCO2 measured by capnometry using the capnometry-type oxygen mask with PaCO2 obtained by blood gas analysis. The secondary goal was to evaluate the association between PaCO2 and PETCO2 under different breathing conditions. Because functional residual capacity is frequently reduced in patients undergoing surgery near the diaphragm (ie, upper abdominal or thoracic incisions),16 we assessed whether deep breathing that decreases the physiological dead space leads to dissociation between PETCO2 and PaCO2.
QUICK LOOK
Current knowledge
End-tidal carbon dioxide concentration monitoring with capnometry in anesthesia is a standard of care. Capnometry assures appropriate airway position and provides early detection of changes in ventilation and perfusion. The accuracy of carbon dioxide monitoring during spontaneous breathing in extubated patients receiving oxygen therapy is less reliable.
What this paper contributes to our knowledge
A simple mask modified to allow sidestream sampling of gases was able to reliably monitor expired carbon dioxide in a group of postoperative subjects. The system was effective across a range of breathing patterns during oxygen delivery.
Methods
This prospective study was conducted at the Yokohama City University Hospital, a teaching hospital in Japan. The ethics committee of the Yokohama City University Hospital approved the design of this study. This study was registered with the University Hospital Medical Information Network Center (UMIN000011925), and informed consent was obtained from all subjects. For this study, adult subjects admitted to the ICU after extubation in the operating room for an abdominal operation were included. These subjects were monitored in the ICU for preventive postoperative complications, such as bleeding, respiratory dysfunction, and hemodynamic instability. The exclusion criteria were: < 18 y old, inability to maintain an SpO2 of > 95% with an oxygen mask, need for noninvasive mechanical ventilation, body mass index of > 30 kg/m2, and absence of epidural anesthesia because conditions such as obesity and surgical trauma pain probably influence postoperative respiratory function, leading to ventilation-perfusion mismatching.4,17 In this study, we focused on accuracy of PETCO2 measurement using a capnometry-type oxygen mask in subjects without a past medical history of pulmonary disease.
The capnometer was calibrated before oxygen administration. Immediately after admission to the ICU, oxygen at 6 L/min was administered via an adult-size capnometry-type oxygen mask. The capnometry mask was positioned such that the bedside monitor displayed a normally shaped capnography waveform and a normal PETCO2 value. The PETCO2 was measured with a sidestream capnometer by spectrophotometry.
A blood sample for blood gas analysis was obtained from an artery before measurement of PETCO2. After blood gas analysis, PETCO2 under the resting condition was measured using the capnometry-type oxygen mask; next, the subject was encouraged to take a few deep breaths, and PETCO2 under the deep-breathing condition was measured using the same device. Blood gas analysis and PETCO2 measurement were performed after a constant and normally shaped capnography waveform was confirmed after 30 min of oxygen administration.
Subjects who had episodes of apnea, dyspnea, and arterial desaturation (defined as SpO2 < 95%) were eliminated from this study. The study period was 30 min for each subject.
Statistics
Quantitative variables are expressed as median and interquartile range. The relationship between PETCO2 and PaCO2 was analyzed by the Pearson product moment correlation coefficient for assessing validity and reliability. Because a few measurements were obtained for each subject, the mean bias and limits of agreement were estimated by a component of variance technique.18 The agreement between PETCO2 and PaCO2 was assessed using a Bland-Altman plot. Dissociation between PETCO2 and PaCO2 under 2 breathing conditions was compared by the Student t test. For 2-tailed tests, P < .05 was considered statistically significant. Statistical analyses were performed with Prism 6 for Mac OS X 6.9b (GraphPad Software, San Diego, California).
Sample size was calculated based on power analysis performed with R 2.13.0 statistical software (R Foundation for Statistical Computing, Vienna, Austria), which showed that 20 samples were required for a 2-sided test with a significance of 0.05, power of 0.8, and estimated correlation coefficient of 0.6. Therefore, 27 subjects were enrolled in this study, considering the imminent elimination of subjects.
Results
Twenty-seven adult subjects were enrolled, and 2 subjects were excluded because their body mass index was > 30 kg/m2. The characteristics of the subjects are provided in Table 1.
Demographic and Perioperative Characteristics of Subjects
The results show that the capnometry-type oxygen mask was well tolerated by all subjects. No episodes of apnea or arterial desaturation were experienced during the study period. The correlation between PETCO2 and PaCO2 under resting and deep-breathing conditions was statistically significant (Fig. 2). Pearson correlation analysis provided the following results: PaCO2 versus resting PETCO2, r = 0.50 (95% CI 0.126–0.745, P = .01); and PaCO2 versus deep-breathing PETCO2, r = 0.56 (95% CI 0.205–0.787, P = .001).

Relationship between PaCO2 and end-tidal carbon dioxide concentration (PETCO2) under resting (RE) and deep-breathing (DB) conditions. PETCO2 and PaCO2 were statistically correlated (r = 0.50 and 0.56, respectively).
The Bland-Altman plot shows the relationship between blood gas analysis and PETCO2 for each subject (Fig. 3). The bias and limits of agreement were −12.6 (−20.6 to −4.6) for resting PETCO2 and −9.1 (−16.1 to −2.1) for deep-breathing PETCO2. The dissociation between deep-breathing PETCO2 and PaCO2 was significantly smaller than that between resting PETCO2 and PaCO2 (P = .002).

A: The Bland-Altman plot shows differences in measurement of end-tidal carbon dioxide concentration (PETCO2) under the resting condition (RE) and PaCO2 at 6 L/min. The bias and limits of agreement were −12.6 (−20.6 to −4.6). B: The Bland-Altman plot shows differences in measurement of PETCO2 under the deep-breathing condition (DB) and PaCO2 at 6 L/min. The bias and limits of agreement were −9.1 (−16.1 to −2.1).
Discussion
To evaluate the use of a capnometry-type oxygen mask for continuous monitoring of CO2 in subjects extubated after abdominal surgery, we compared PETCO2 measured by capnometry using the new capnometry-type oxygen mask with PaCO2 measured by blood gas analysis. We also compared the dissociation between PaCO2 and PETCO2 under resting and deep-breathing conditions.
In our study, PaCO2 and PETCO2 were significantly correlated under various breathing conditions (resting condition, r = 0.50; deep breathing, r = 0.56). Normally, dissociation between PaCO2 and PETCO2 depends on the sum of space composed of apparatus, anatomical, and physiological dead space. In the postoperative situation, various factors affect dead space, leading to the dissociation between PaCO2 and PETCO2. In our study, similar subjects with fewer respiratory complications were enrolled. Therefore, the sum of dead space was probably similar for all subjects, resulting in the statistically significant correlation between PaCO2 and PETCO2. However, the effect of other factors, such as comorbidity, skin incision, and postoperative pain, on postoperative respiratory function varied between subjects. These various perioperative conditions might affect a wide range of the limits of agreement. It was difficult to estimate the extent of dead space between subjects.
Statistically, the dissociation between PaCO2 and deep-breathing PETCO2 was significantly smaller than that between PaCO2 and resting PETCO2 (P = .002). We believe that the change in dissociation may be due to reduced ventilation/perfusion mismatching caused by a decrease in physiological dead space. Although continuous CO2 monitoring with deep-breathing PETCO2 may be useful in clinical settings, it is difficult to predict the precise value of PaCO2 under the 2 breathing conditions. Because the limits of agreement have a wide range and are similar for both breathing patterns (16.0 [resting] vs 14.0 [deep breathing]), the bias of PaCO2 and PETCO2 becomes smaller during deep breathing (−12.6 to −9.1). Therefore, it is difficult to postulate which breathing pattern is superior for the prediction of PaCO2. Moreover, monitoring PETCO2 may not be useful for evaluating the absolute value of PaCO2; however, it may be useful for assessing the PaCO2 trend.
In extubated subjects after general anesthesia, continuous monitoring of CO2 using the capnometry-type oxygen mask correlated with PaCO2, especially under the deep-breathing condition. Continuous capnometric monitoring previously required the patient to be intubated; therefore, its use was limited mostly to ventilated patients. A nasal cannula and face mask have been developed to monitor spontaneous breathing patterns in subjects requiring supplemental oxygen.11–13,19,20 However, a nasal cannula carries the risk of leakage if a patient exhales CO2 through the mouth. The accuracy of CO2 monitoring by a capnometer has been described; however, the relationship between PETCO2 under the deep-breathing condition and PaCO2 has not been elucidated.
Continuous monitoring of PETCO2 is useful for arterial CO2 assessment, particularly in patients with normal ventilation/perfusion relationships.5 However, in cases of impaired ventilation/perfusion relationships, such as postabdominal operations, PETCO2 monitoring for arterial CO2 assessment is equivocal.
When patients resort to mouth breathing after extubation, nasal devices do not work. However, the capnometry-type oxygen mask samples expired CO2 from both the nose and mouth, reducing the risk of false alarms. However, this mask also carries the risk of rebreathing that is exacerbated by high breathing rates and use of long sampling catheters.21,22 Because the risk of rebreathing CO2 during oxygen delivery at a low rate has not been evaluated, it seems advisable to reserve this device for patients who require a supplemental oxygen flow conventionally used for oxygen face masks (> 5 L/min). In our study, the oxygen supplementation rate was 6 L/min, which minimized the risk of CO2 rebreathing and is probably why none of the subjects developed CO2 retention.
This study has several limitations. First, the sample size was small (25 subjects), and subjects who underwent open upper abdominal surgery or laparotomy were included. These diverse operation methods lead to varying extents of postoperative pain and respiratory muscle dysfunction. Functional disruption of respiratory muscles by incision, even after surgical repair, may impair their effectiveness. Furthermore, postoperative pain may limit respiratory motion and influence CO2 production. Therefore, the usefulness of the capnometry-type oxygen mask in other conditions remains unclear. Second, smokers and subjects with COPD were enrolled in this study. However, previous studies on PETCO2 monitoring showed limited accuracy in both intubated and non-intubated subjects with pulmonary disease.23,24 These comorbidities may affect pulmonary mechanisms after extubation. Third, data collection was not blinded, which may have affected PETCO2 measurement under the deep-breathing condition. This relates to our conclusion that deep breathing elevates PETCO2 due to reduction of ventilation/perfusion mismatching. However, in a few subjects, PETCO2 decreased after deep breathing compared with that under the resting condition. The PETCO2 was measured only twice by blood gas analysis. Therefore, it was difficult to confirm the usefulness of this device for continuous respiratory monitoring.
Conclusions
Further studies should be undertaken on continuous monitoring of PETCO2 during the entire postoperative period using this device following similar surgeries with similar pulmonary conditions. In summary, our study shows that it is possible to measure the PETCO2 under varying breathing conditions with the capnometry-type oxygen mask in subjects receiving oxygen supplementation after extubation following upper abdominal surgery to determine whether they are properly ventilating.
Footnotes
- Correspondence: Shunsuke Takaki MD PhD, Department of Anesthesiology and Intensive Care Unit, Yokohama City University Hospital, 3-9 Fukuura, Kanazawa-ku, Yokohama city, Kanagawa 236-0004, Japan. E-mail: shunty5323{at}gmail.com.
The study was supported by the Yokohama City University Hospital. The authors have disclosed no conflicts of interest.
- Copyright © 2015 by Daedalus Enterprises





{kind=link}
{kind=link}
{kind=link}